Hypotony maculopathy is a condition in which persistent low intraocular pressure (IOP) due to various causes leads to the formation of chorioretinal folds at the posterior pole of the fundus, resulting in visual dysfunction. It is often accompanied by optic disc edema, dilation and tortuosity of retinal veins, and dilation of choroidal veins, with common subjective symptoms including decreased visual acuity and metamorphopsia.
This disease was first reported by Dellaporta in 1954 as fundus changes associated with low IOP, and in 1972 Gass proposed the term “hypotony maculopathy” to clarify the pathogenesis of visual loss related to choroidal folds8). Although low IOP itself is relatively common after surgery or trauma, only a subset of cases develop maculopathy leading to visual dysfunction. Individual factors such as scleral rigidity and axial length influence the onset.
Hypotony maculopathy can develop at IOP levels of 8–10 mmHg or lower, with the incidence increasing at 5 mmHg or below. Statistically, an IOP of less than 6.5 mmHg (more than 3 standard deviations below the mean IOP) is defined as “hypotony.” Clinically, it refers to a state where IOP is low enough to cause visual dysfunction.
Basic Concept of Pathophysiology (Gass Hypothesis)
Gass’s hypothesis, which states that mechanical strain on the retinal pigment epithelium (RPE) and photoreceptors due to chorioretinal folds is the main cause of visual dysfunction, is widely accepted. When the ocular wall collapses inward due to low IOP, redundancy in the choroid and retina leads to the formation of folds. If this change resolves within a short period, visual function may recover, but if it persists for a long time, irreversible visual dysfunction may result.
QWhat is the IOP level (in mmHg) defined as hypotony?
A
Statistically, hypotony is defined as an IOP less than 6.5 mmHg, which is 3 standard deviations below the mean IOP. However, hypotony maculopathy can develop at IOP levels of 8–10 mmHg or lower, and the incidence clearly increases at 5 mmHg or below. At 4 mmHg or below, severe visual loss (corrected visual acuity of 0.2 or worse) often occurs. Clinically, the level of hypotony that impairs visual function is the concern.
The most common cause is excessive filtration after glaucomafiltration surgery, particularly after trabeculectomy with mitomycin C (MMC). According to the glaucoma practice guidelines, the frequency of hypotony maculopathy as a complication that can cause visual dysfunction one month or more after surgery is reported to be 0.9–5% 1). In a review by Costa & Arcieri (2007), the incidence is summarized as ranging from 1.3% to 18% 8). The next most common cause is cyclodialysis associated with blunt trauma.
It is known to occur more frequently in young individuals and those with high myopia2). In young and myopic eyes, the scleral rigidity is low, so the sclera tends to collapse inward under low intraocular pressure, and choroidal folds are easily formed. Elderly patients are more prone to choroidal effusion, while young patients tend to develop hypotony maculopathy. Since the use of antimetabolites became widespread, reports of hypotony maculopathy after filtration surgery have increased.
The causes of hypotony maculopathy are broadly divided into increased aqueous outflow and decreased aqueous production.
Overfiltration after glaucomafiltration surgery: This is the most common cause. It can occur when intraocular pressure drops significantly after trabeculectomy with MMC. Contributing factors include aqueous leakage from the conjunctival wound, excessive aqueous outflow through the scleral flap, and direct toxicity of MMC to the ciliary body.
Ciliary body detachment after blunt trauma: When ciliary body detachment occurs in the angle, aqueous humor flows into the suprachoroidal space, and aqueous production also decreases. Pathological increase in uveoscleral outflow leads to marked hypotony.
Uveitis / cyclitis: Hypotony occurs due to decreased aqueous production.
Progression of anterior proliferative vitreoretinopathy: Prolonged peripheral retinal and ciliary body detachment reduces aqueous production capacity.
After retinal detachment surgery / vitrectomy: Leakage from sclerotomy sites or transient hypotony due to postoperative inflammation is the cause. Previous vitrectomy, young age, and myopia are risk factors 9).
After tube shunt surgery: The TVT study showed that bleb leakage, hypotony maculopathy, and bleb infection were more common in the trabeculectomy group, while corneal endothelial damage and implant exposure were more common in the tube shunt group 1).
After intravitreal anti-VEGF injection: Onset has been reported in cases with pseudoxanthoma elasticum, high myopia, or scleral fragility after vitrectomy11).
Bilateral hypotony: Causes include osmotic dehydration, diabetic coma, uremia, and myotonic dystrophy.
Fannin et al. (2003) identified the following risk factors for hypotony maculopathy 7).
Young age: Scleral rigidity is low, making collapse easier. The healing response of the scleral flap is weak, and overfiltration tends to persist.
Male sex: Incidence tends to be higher in males than females.
Myopia (especially high myopia): The sclera is thin and soft, making folds more likely to form.
First glaucomafiltration surgery: Risk is higher before becoming proficient in postoperative management.
Use of antifibrotic agents: MMC carries a higher risk than 5-FU.
High preoperative intraocular pressure: The higher the preoperative IOP, the greater the postoperative drop.
QWhy are young people and myopic individuals at higher risk?
A
In young patients, the scleral flap heals with weaker scarring, and excessive filtration tends to persist postoperatively. In myopic individuals, especially those with high myopia, the sclera is thin and fragile, so even with the same low IOP, chorioretinal folds are more likely to form. When these factors combine, the risk increases further.
The development of hypotony maculopathy involves a close interplay between abnormal aqueous humor dynamics and mechanical deformation of the ocular wall.
Abnormalities in aqueous humor dynamics leading to hypotony can be broadly divided into two categories.
Increased aqueous outflow: Leakage from surgical wound, excessive filtering bleb, aqueous outflow from cyclodialysis cleft. In cyclodialysis, uveoscleral outflow is pathologically increased.
Decreased aqueous production: Ciliary body inflammation, direct damage to ciliary body (trauma, surgery, drug toxicity), ciliary body dysfunction due to anterior proliferative vitreoretinopathy.
In cyclodialysis after trauma, an open communication pathway is created in the ciliary body, allowing aqueous humor to flow into the suprachoroidal space, while damage to the ciliary epithelium reduces aqueous production. In filtering surgery using antimetabolites (MMC, 5-FU), scarring around the scleral flap is suppressed, increasing aqueous leakage1).
When ocular hypotony occurs, the scleral wall collapses inward, creating redundancy in the choroid and retina, leading to characteristic chorioretinal folds. The anteroposterior diameter of the eye shortens, resulting in hyperopic shift as a refractive error.
Sakamoto et al. (2018) reported that excessive scleral contraction, rather than choroidal thickening, is a major contributing factor in the development of hypotony maculopathy after trabeculectomy2). Persistent hypotony leads to relaxation and contraction of scleral collagen fibers, causing irreversible shortening of the axial length.
Gass Hypothesis and Mechanism of Visual Dysfunction
In the hypothesis proposed by Gass in 1972, chorioretinal folds cause mechanical strain on the RPE and photoreceptors, which is considered the essence of visual dysfunction. This hypothesis remains widely accepted.
Recent OCT studies have identified photoreceptor folds distinct from choroidal folds9). Photoreceptor folds form directly beneath choroidal folds and are accompanied by disruption of the photoreceptor outer segments. This mechanical damage to photoreceptors is the main cause of irreversible central vision loss; even if choroidal folds resolve, if photoreceptor damage persists, visual recovery is poor9).
With ocular hypotony, the lamina cribrosa bulges forward, restricting axonal flow and causing optic disc edema in the acute phase. In advanced glaucoma with few surviving axons, disc swelling may be inconspicuous even with hypotony.
When the posterior segment of the eye buckles due to low intraocular pressure, retinal venous outflow is obstructed, leading to stasis. This is clinically observed as dilation and tortuosity of retinal veins.
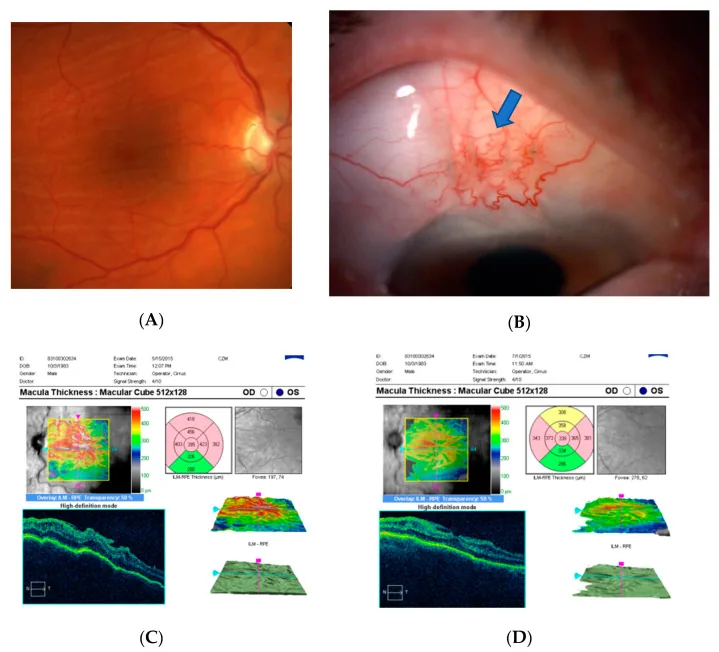
Kosior-Jarecka E, et al. Bleb Compressive Sutures in the Management of Hypotony Maculopathy after Glaucoma Surgery. J Clin Med. 2021. Figure 4. PMCID: PMC8196590. License: CC BY.
(A) Fundus photograph of hypotony maculopathy, (B) Compression suture on postoperative day 1 (blue arrow), (C) Macular OCT before suture, (D) Macular OCT after suture. This corresponds to hypotony maculopathy discussed in the section “4. Clinical Features”.
Decreased visual acuity: May be slowly progressive or sudden. When intraocular pressure is 4 mmHg or less, corrected visual acuity often becomes 0.2 or worse.
Hyperopic shift: Refractive change due to shortening of the axial length.
Asymptomatic: Early or mild cases may be completely asymptomatic and sometimes discovered incidentally on routine OCT.
The duration of hypotony does not necessarily correlate with final visual acuity, but early recovery of intraocular pressure can lead to improvement in visual function.
Recent OCT studies have identified not only choroidal folds but also photoreceptor folds, and mechanical damage to the photoreceptor layer is considered the main cause of irreversible central vision loss 9). Hyperreflectivity of the Henle fiber layer has also been reported as a characteristic OCT finding 9).
When hypotony persists, the sclera contracts excessively, shortening the axial length. Sakamoto et al. (2018) reported that excessive scleral contraction contributes more to the development of hypotony maculopathy after trabeculectomy than choroidal thickening 2). Ultrasound B-scan may show thickening of the posterior sclera and choroid, and many cases are accompanied by choroidal detachment.
Maheshwari et al. (2022) reported a case of a 70-year-old man with primary open-angle glaucoma3). After combined cataract and glaucoma surgery, severe hypotony (1 mmHg) and 360-degree choroidal detachment occurred, leading to hypotony maculopathy. Transconjunctival scleral flap suturing resolved the choroidal detachment, and both intraocular pressure and visual acuity improved.
The diagnosis of hypotony maculopathy is relatively straightforward based on history, confirmation of low intraocular pressure by tonometry, and characteristic fundus findings.
OCT is the first-line test and has higher detection ability than fundus examination. It is important to carefully check all radial scans. Even when the fundus appears clinically normal, OCT can detect pathological changes 9).
Fluorescein angiography (FA) characteristically shows linear hypofluorescence corresponding to RPE thinning at the folds and enhanced choroidal fluorescence at the fold peaks. Indocyanine green angiography (ICG) is useful as a complementary test in cases difficult to diagnose with FA, showing dilated and tortuous choroidal veins and multiple linear hypofluorescences.
OCT can detect chorioretinal folds with high precision and can identify subtle folds that may be missed on fundus examination. Furthermore, it can evaluate findings related to visual prognosis, such as photoreceptor folds and hyperreflectivity of the Henle fiber layer 9). It is also useful for follow-up after treatment, allowing objective assessment of fold improvement and residual photoreceptor damage.
Diagnosis is made by the combination of hypotony and characteristic fundus findings. Inquire about history of glaucoma surgery, trauma, vitreous surgery, and anti-VEGF injections.
E (Extraocular hardware): Scleral buckle, radiation plaque, etc.
Proceed with differential diagnosis considering the presence of hypotony, history of glaucoma surgery, and trauma history.
QCan the chorioretinal folds of hypotony maculopathy also be seen in other diseases?
A
As the THIN RPE mnemonic indicates, chorioretinal folds can occur in many diseases such as tumors, inflammation, papilledema, and orbital space-occupying lesions. It is necessary to proceed with differential diagnosis considering the presence of hypotony, history of glaucoma surgery, and trauma history.
Treatment of hypotony maculopathy prioritizes identifying and addressing the cause. Since many cases resolve spontaneously, conservative treatment is first attempted, and if no improvement occurs, active intervention is considered stepwise.
Important time constraint: It has been reported that hypotony maculopathy persisting for more than 3 months tends to leave permanent visual impairment. Surgical treatment is recommended before visual dysfunction becomes permanent, and a decision is generally made within 1 to 6 months. Marked hypotony of 4 mmHg or less persisting for 2 to 3 months tends to leave metamorphopsia and relative central scotoma. On the other hand, if intraocular pressure is higher than 4 mmHg, visual function may recover even if it persists for about half a year.
1% atropine eye drops: With continued conservative treatment, sudden elevation of intraocular pressure often leads to spontaneous resolution of cyclodialysis.
Steroid eye drops: Anti-inflammatory.
Ciliary body hypotony (after PVR): Effective treatments are limited, mainly anti-inflammatory eye drops.
Ciliary body hypotony (after PVR): Effective treatments are limited, mainly anti-inflammatory eye drops.
If conservative treatment does not improve, consider the following interventions.
Autologous blood injection: Inject autologous blood into and around the filtering bleb to reduce filtration 4, 5, 6). Caution is needed as it may cause a sudden rise in intraocular pressure10).
Transconjunctival scleral flap suture: A method of suturing the scleral flap directly with nylon thread through the conjunctiva, shown to be effective long-term for hypotony maculopathy 3, 12).
Intracameral injection of viscoelastic material or air: Restores anterior chamber volume and temporarily increases intraocular pressure. Can be repeated but the effect is often temporary.
Additional scleral suture: Surgically reopen the conjunctiva and suture the scleral flap under direct visualization. If there is marked choroidal detachment, it may be necessary to drain fluid from the suprachoroidal space via sclerostomy.
Surgical options if the above do not improve or if intraocular pressure recovery is not achieved are as follows.
Laser photocoagulation (of the cyclodialysis cleft): Indicated if cyclodialysis does not resolve within 1-2 weeks. Use green or yellow wavelength laser, spot size 100-200 μm, duration 0.2-0.5 seconds, power 200 mW or more, to achieve slight contraction of the ciliary body and minimal fibrin exudation. Repeat after a few days if ineffective. Often causes transient ocular hypertension before intraocular pressure recovery.
Cyclopexy: Create a half-thickness scleral incision or scleral flap about 3.5 mm from the limbus, and suture the detached ciliary body epithelium to the sclera with absorbable sutures.
Bleb revision (conjunctival advancement): Excise the thinned bleb and reconstruct the bleb by advancing the conjunctiva13).
Other surgeries: Diathermy coagulation, cyclocryotherapy, scleral buckling, encircling band, intravitreal gas injection, intraocular lens suturing, etc. have been reported.
The stages and timing of treatment are summarized as follows.
Laser photocoagulation (to the cyclodialysis cleft), continued observation
Within 6 months
Surgery (cyclopexy, bleb revision, scleral buckling, etc.)
QIs urgent surgery necessary for hypotony maculopathy?
A
Hypotony maculopathy may resolve spontaneously, so conservative treatment is attempted first. However, if low intraocular pressure persists for more than 3 months, permanent visual impairment is likely, so surgical intervention should be considered within 1 to 6 months if conservative treatment fails. In particular, for marked hypotony with intraocular pressure of 4 mmHg or less, restoration of intraocular pressure within 2 months is desirable.
QWhat happens if hypotony maculopathy is left untreated?
A
If intraocular pressure of 4 mmHg or less continues for a long time, fibrosis within the retina, sclera, and choroid may progress, leading to irreversible visual impairment. Restoration of intraocular pressure within 2 months is considered an important guideline. If intraocular pressure is higher than 4 mmHg, recovery may be possible even after about six months.
If intraocular pressure is restored early, improvement in visual function can be expected. On the other hand, if photoreceptor folds or fibrosis of the sclera and choroid become established, irreversible visual impairment remains 9). If intraocular pressure of 4 mmHg or less persists for 2 to 3 months, metamorphopsia and relative central scotoma tend to remain.
Lee & Woo (2021) reported two cases of hypotony maculopathy (53-year-old woman and 20-year-old man, South Korea) that developed after vitrectomy for epiretinal membrane removal. Both presented with unmeasurable low intraocular pressure after 25-gauge sutureless vitrectomy, and OCT identified characteristic photoreceptor folds and hyperreflectivity of the Henle fiber layer. Even after normalization of intraocular pressure, photoreceptor damage persisted, and visual acuity at one year was worse than before surgery. Previous vitrectomy history, young age, and myopia were listed as risk factors for hypotony maculopathy 9).
Barbosa et al. (2022) reported a case of a woman in her 70s who developed hypotony maculopathy with intraocular pressure of 2 mmHg three years after non-penetrating glaucoma surgery (deep sclerectomy). Complete recovery was achieved after eight weeks of dexamethasone eye drops five times daily and cyclopentolate twice daily, but recurrence occurred two months after stopping steroids. When steroid eye drops were resumed and continued at a maintenance dose, stable intraocular pressure (14–17 mmHg) and good visual acuity were maintained for 14 months 14). This is an interesting report applying the characteristics of steroid responders to treatment.
New Technique of Transconjunctival Scleral Flap Suturing
Maheshwari et al. (2022) reported a minimally invasive technique of suturing the scleral flap transconjunctivally without incising the conjunctiva3). In a 70-year-old male glaucoma case who developed severe hypotony (1 mmHg) and 360-degree choroidal detachment after combined cataract and glaucoma surgery, this technique resolved the choroidal detachment and improved both intraocular pressure and visual acuity. This technique is introduced as a promising method that is minimally invasive and can be performed on an outpatient basis.
Atypical Cause: After Intravitreal Anti-VEGF Injection
Lima-Fontes et al. (2022) reported a case of a 52-year-old man with pseudoxanthoma elasticum who developed hypotony maculopathy after intravitreal ranibizumab injection (after the 78th injection). The cause was scleral dehiscence at the injection site with a 30-gauge needle. High myopia, pseudoxanthoma elasticum, repeated injections, and absence of vitreous due to prior vitrectomy were considered factors of scleral fragility. Recovery was achieved with scleral suturing and atropine and dexamethasone eye drops 11).
Markopoulos et al. (2023) reported a 78-year-old man who developed peripapillary retinoschisis (PPRS) associated with low intraocular pressure (6 mmHg) after trabeculectomy. PPRS completely resolved after 4 weeks of treatment with dexamethasone 0.1% eye drops twice daily and nepafenac eye drops three times daily, and intraocular pressure recovered to 16 mmHg. It is speculated that the mechanism of PPRS development involves changes in capillary hydrostatic pressure gradient due to low intraocular pressure, promoting fluid movement into the extracellular space15).
For refractory hypotony maculopathy, methods combining vitrectomy with internal limiting membrane (ILM) peeling and flattening of chorioretinal folds using perfluorocarbon liquid (PFCL) have been reported. These are all at the case report level and have not been established as standard treatment.
Mari Sakamoto, Yoshiko Matsumoto, Sotaro Mori, Kaori Ueda, Yukako Inoue, Takuji Kurimoto, et al. Excessive scleral shrinkage, rather than choroidal thickening, is a major contributor to the development of hypotony maculopathy after trabeculectomy. PLoS ONE. 2018;13(1):e0191862. doi:10.1371/journal.pone.0191862.
Maheshwari D, Shyam P, Pawar N, Ramakrishnan R. Transconjunctival flap sutures: A novel technique to combat hypotony. Indian J Ophthalmol. 2022;70(6):2223-2225.
Wise JB. Treatment of chronic postfiltration hypotony by intrableb injection of autologous blood. Archives of ophthalmology (Chicago, Ill. : 1960). 1993;111(6):827-30. doi:10.1001/archopht.1993.01090060115034. PMID:8512485.
Nuyts RM, Greve EL, Geijssen HC, Langerhorst CT. Treatment of hypotonous maculopathy after trabeculectomy with mitomycin C. American journal of ophthalmology. 1994;118(3):322-31. doi:10.1016/s0002-9394(14)72956-3. PMID:8085589.
Okada K, Tsukamoto H, Masumoto M, Jian K, Okada M, Mochizuki H, et al. Autologous blood injection for marked overfiltration early after trabeculectomy with mitomycin C. Acta ophthalmologica Scandinavica. 2001;79(3):305-8. doi:10.1034/j.1600-0420.2001.790320.x. PMID:11401645.
Lilia A Fannin, Joyce C Schiffman, Donald L Budenz. Risk factors for hypotony maculopathy. Ophthalmology. 2003;110(6):1185-1191. doi:10.1016/s0161-6420(03)00227-6.
Lee YJ, Woo SJ. Hypotony maculopathy and photoreceptor folds with disruptions after vitrectomy for epiretinal membrane removal: two case reports. Journal of medical case reports. 2021;15(1):255. doi:10.1186/s13256-021-02824-3. PMID:33957968; PMCID:PMC8103759.
Lima-Fontes M, Godinho G, Cunha AM, et al. Hypotony Maculopathy Related to Anti-VEGF Intravitreal Injection. Int Med Case Rep J. 2022;15:517-520.
Eha J, Hoffmann EM, Pfeiffer N. Long-term results after transconjunctival resuturing of the scleral flap in hypotony following trabeculectomy. American journal of ophthalmology. 2013;155(5):864-9. doi:10.1016/j.ajo.2012.12.004. PMID:23394904.
Satpute K, Bukke AN, Verma S, Dada T. Conjunctival advancement for management of hypotony maculopathy after trabeculectomy. BMJ case reports. 2022;15(11). doi:10.1136/bcr-2022-251718. PMID:36328363; PMCID:PMC9639019.
Barbosa RC, Bastos R, Tenedório P. Recurrent macular neurosensory detachment in hypotony maculopathy managed with topical corticosteroids. BMJ case reports. 2022;15(6). doi:10.1136/bcr-2022-248773. PMID:35705300; PMCID:PMC9204401.
Markopoulos I, Tzakos M, Tzimis V, Halkiadakis I. Peripapillary Retinoschisis as a Manifestation of Ocular Hypotony. Case reports in ophthalmology. 2023;14(1):13-17. doi:10.1159/000528636. PMID:36619359; PMCID:PMC9818672.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.