Color fundus photographs provide high-resolution images similar to those observed during fundus examination. They reproduce the natural color of the fundus without processing, and some devices are equipped with various imaging modes and filters to highlight specific lesions.
By two-dimensionally recording color information such as hemorrhages (red) and hard exudates (yellow-white), as well as morphological changes such as macular holes, optic disc cupping, and vascular abnormalities, objective and longitudinal evaluation is possible.
OCT provides detailed morphological information of posterior pole lesions but does not provide color information. A unique strength of color fundus photography is the ability to infer lesion components from color information.
The fundus contains red from blood hemoglobin, brown from RPE and choroidal melanin pigment, yellow from macular pigment (xanthophyll), yellow-white from hard exudates, and white from cotton-wool spots and necrotic retina.
Diabetic retinopathy (DR): Useful for recording severity, presence of optic disc/retinal neovascularization (NVE), and treatment effects. Wide-angle imaging is especially effective for capturing the overall picture of DR. 1)
Retinal vein occlusion (RVO): Useful for recording severity of retinal findings, NVE, and extent of intraretinal hemorrhage. 2)
Retinal Artery Occlusion (RAO): Useful for recording severity of retinal findings, vessel diameter, intraretinal emboli, and presence of neovascularization3)
QWhat is the difference between fundus photography and OCT?
A
Fundus photography records color information and morphological changes two-dimensionally, allowing visual identification of hemorrhages, exudates, vascular abnormalities, and pigment changes. OCT provides detailed morphological information through tomographic images but does not capture color information. Both are complementary examinations.
2. Normal Findings and Anatomical Structures to Observe
To differentiate left and right eyes in fundus photography, use the positional relationship between the optic disc and the macula. The optic disc is always on the nasal side, and the macula is always on the temporal side. If the optic disc is visible in the right half of the image, it is the right eye; if in the left half, it is the left eye.
The optic disc (optic nerve head) is located on the nasal side, appears yellowish-orange to pink, and has clear margins. The temporal margin is particularly distinct, while the nasal margin is slightly indistinct.
Components of the Optic Disc
Scleral ring: Surrounds the outer edge of the optic disc. Formed at the point where the sclera ends and nerve fibers enter the eye.
Neuroretinal rim: The tissue between the edge of the cup and the edge of the disc. It consists mainly of nerve fibers and glial cells and is usually pink.
Optic disc cupping: A pale, horizontally oval depression in the center. Normal cup-to-disc ratio is less than 0.5.
ISNT Rule
Definition: A mnemonic for the normal distribution of neuroretinal rim thickness.
The central retinal artery and vein emerge from the optic disc and divide into four branches: superotemporal, inferotemporal, superonasal, and inferonasal. In about one-third of the population, a cilioretinal artery is present, supplying blood to the perimacular area.
Arteries are narrower and brighter in color than veins.
Beyond one disc diameter, they are called arterioles and venules.
Macula: Located about two disc diameters temporal and slightly inferior to the optic disc. Diameter approximately 5.5 mm. Appears darker than the surrounding area due to taller RPE cells and higher pigment density.
Fovea: Center of the macula, diameter 1.5 mm. Lutein and zeaxanthin contribute to its yellowish color.
Uniform brightness, good contrast, and clear visualization of fundus structures are necessary conditions for a normal assessment.
The main artifacts are as follows.
Light entering around the periphery: caused by misalignment of the optical axis, forward/backward camera displacement, or obstruction of the light path by eyelashes.
Spots on the image: white spots due to dirt on the objective lens, internal mirrors, or lenses.
Black central spot: tends to appear when photographing highly myopic eyes.
QHow to distinguish between left and right eyes?
A
If the optic disc is in the right half of the image, it is the right eye; if in the left half, it is the left eye. This is based on the anatomical principle that the optic nerve is always on the nasal side and the macula is always on the temporal side.
3. Classification of Abnormal Findings and Causative Diseases
Disc pallor: suggests ischemia due to vascular loss, or fibrosis, demyelination, or gliosis. Main causes: anterior ischemic optic neuropathy (AION), optic atrophy, optic nerve hypoplasia.
Disc hyperemia: occurs from disc edema or inflammation. Papilledema due to increased intracranial pressure is distinguished from “optic disc edema.”
Pigmentation: optic disc melanocytoma (eccentric black lesion), infiltration of choroidal melanoma.
Disc edema: characterized by blurred margins and hyperemia. The Frisen scale is widely used for severity grading.
Pseudopapilledema: a condition where the disc appears elevated without swelling of the nerve fiber layer. Differentiation from true disc edema is important.
Peripapillary atrophy (PPA): consists of two zones: alpha zone (irregular pigmentation/depigmentation) and beta zone (visibility of sclera and large choroidal vessels). A non-specific finding seen in both high myopia and glaucoma.
Myopic crescent: A white depigmented crescent-shaped lesion on the temporal side of the optic disc. Caused by scleral stretching and RPE thinning.
Optic disc notching: A localized indentation of the disc contour associated with focal RNFL loss. Related to glaucomatous changes.
Myelinated nerve fibers: White-gray patches with feathery borders that obscure underlying blood vessels.
Optic pit: A gray to white round or oval depression, usually inferotemporal. A congenital anomaly.
Optic disc drusen: Calcified yellowish-white round deposits. The disc appears lumpy-bumpy and elevated.
Arteriovenous crossing phenomenon (AV nicking): Compression and focal narrowing of adjacent veins by sclerotic arteries. Most commonly due to chronic hypertension.
Microaneurysm: Small red dot-like lesions. Commonly seen in diabetic retinopathy.
Intravascular plaque: Cholesterol (Hollenhorst plaque), talc, or calcium deposits at bifurcations.
Vascular discontinuity: Due to vessel invasion by a tumor or non-perfusion (e.g., BRAO or cavernous hemangioma).
Crystalline retinopathy: Numerous small yellow crystalline deposits. Causes include talc retinopathy, Bietti crystalline dystrophy, cystinosis, tamoxifen retinopathy, etc.
Epiretinal membrane (ERM): A transparent to white to yellow fibrovascular membrane covering the macula. Membrane contraction causes loss of the foveal depression and wrinkling of the retinal surface.
QHow to determine the depth of hemorrhage on fundus photographs?
A
The positional relationship with retinal vessels is key. If the hemorrhage covers the vessels, it is preretinal (vitreous or under the ILM); if it lies between vessels, it is intraretinal; if vessels run over the hemorrhage, it is subretinal. The shape of the hemorrhage (flame-shaped, dot, boat-shaped) also helps differentiate depth.
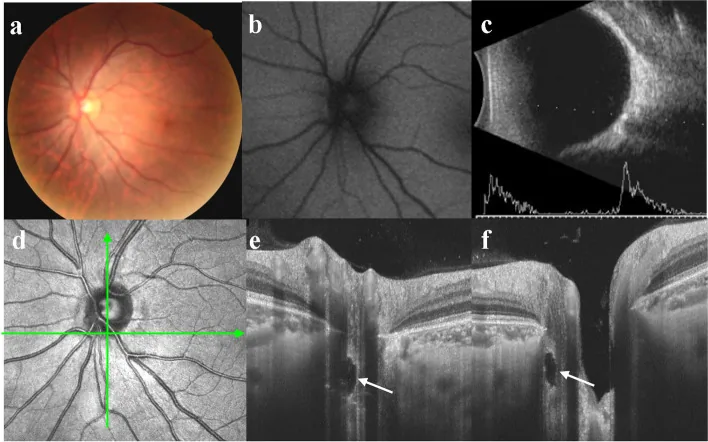
Xiaohong Guo; Yingjie Wu; Yuhong Wu; Hui Liu; Shuai Ming; Hongpei Cui; Ke Fan; Shuyin Li; Bo Lei. Detection of superficial and buried optic disc drusen with swept-source optical coherence tomography. BMC Ophthalmol. 2022 May 13; 22:219. Figure 3. PMCID: PMC9107153. License: CC BY.
Multimodal imaging of a typical buried ODD a There was no noticeable pseudoedema in the optic disc. b No autofluorescence was detected. c B-scan ultrasonography showed strong echo spots with acoustic shadowing. d Horizontal scan line corresponded to e, vertical scan line corresponded to f. e/f An ODD was located near the rim of the optic disc (white arrow), and there was no highly reflective mass around the optic papilla
Correctly understanding the characteristics of each imaging device and mode is a prerequisite for proper interpretation.
A comparison of the characteristics of imaging methods is shown below.
Conventional fundus camera: Captures approximately 60-degree images with a white light flash. Image format can be selected from TIFF (uncompressed) or JPEG (compressed).
Ultra-widefield fundus camera (e.g., Optos): Scanning type using laser light sources. Red, green (and blue) wavelength light sources move rapidly through the center of the pupil, and the obtained point information is imaged in pseudo-color. Wide-angle images of approximately 130–135 degrees can be captured without mydriasis in a short time. Particularly effective for grasping the overall picture of DR 1).
Handheld fundus camera (e.g., OPTOMED M5, iExaminer): Field of view 25–40 degrees, non-mydriatic. Suitable for posterior pole imaging at remote locations.
Red-free photography: Black-and-white photograph extracting green and blue components. Excellent for depicting hemorrhages, microaneurysms, and RNFLD. Useful when RNFLD cannot be observed in wide-angle color fundus photographs due to high brightness.
Wavelength-specific layer-selective imaging: Blue light → superficial layer (RNFL), green light → vascular lesions, red light → deep layer to choroid evaluation.
Fluorescein angiography (FA): Imaging after intravenous injection of sodium fluorescein. Mainly excellent for detecting retinal abnormalities (vascular wall abnormalities, neovascularization, RPE abnormalities). Lesions are evaluated by hyperfluorescence (leakage, window defect, tissue staining, pooling) and hypofluorescence (blockage, filling delay).
Indocyanine green angiography (ICG): Excellent for detecting choroidal lesions
QWhat is red-free photography?
A
It is a fundus photograph that extracts only the green and blue components and converts them to black and white. By removing the blood (red), the contrast of hemorrhages, microaneurysms, and retinal nerve fiber layer defects (RNFLD) is enhanced. In some electronic medical record filing systems, it can be converted with a single button.
5. Principles of Lesion Interpretation Based on Color Information
Abnormal pre-existing vessels: Engorgement and tortuosity of the main retinal vein (central retinal vein occlusion), retinal microaneurysms and IRMA (diabetic retinopathy), telangiectasia (Coats disease), redness due to optic disc vascular dilation (optic neuritis)
Acquired melanin pigmentation: Residual melanin pigment in areas of RPE/choroidal degeneration and atrophy, old RPE detachment, choroidal malignant melanoma
RPE detachment: Round or oval elevation, or radial crack pattern from the optic disc
In addition to conventional fundus cameras (white light, approximately 60 degrees), scanning ultra-widefield fundus imaging devices using laser light sources have become widespread. They can capture wide-angle images of approximately 130–135 degrees without pupil dilation and in a short time.
In diseases where peripheral lesions are important, such as DR, retinal vein occlusion, and retinal detachment, the ability to grasp the overall picture has dramatically improved. The Optos series is widely used as a representative device. RetCam is used for pediatric fundus imaging (e.g., evaluation of retinopathy of prematurity).
The American Academy of Ophthalmology’s DR clinical guidelines (2024) state that wide-field imaging is particularly useful for assessing the overall DR burden 1).
Multicolor imaging using a scanning laser ophthalmoscope (SLO) can acquire information from different layers depending on the wavelength. Blue light reflects the superficial layer (RNFL), green light reflects vascular lesions, and red light reflects the deep layer to the choroid.
Lim JI, Kim SJ, Bailey ST, et al. Diabetic Retinopathy Preferred Practice Pattern. Ophthalmology. 2025 Apr;132(4):P75-P162. doi:10.1016/j.ophtha.2024.12.020. PMID:39918521.
American Academy of Ophthalmology. Retinal Vein Occlusions Preferred Practice Pattern. Ophthalmology. 2024.
Kovach JL, Bailey ST, Kim SJ, Lim JI, Vemulakonda GA, Ying GS, et al. Retinal and Ophthalmic Artery Occlusions Preferred Practice Pattern®. Ophthalmology. 2025;132(4):P270-P302. doi:10.1016/j.ophtha.2024.12.024. PMID:39918522.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.