Choroidal effusion is a condition in which serous fluid abnormally accumulates in the suprachoroidal space (the space external to the choroid) from the choroidal capillaries. When the ciliary body and choroid separate from the sclera and fluid accumulates in this space, causing elevation toward the vitreous cavity, it is called choroidal detachment. If a relatively large blood vessel ruptures, it becomes hemorrhagic choroidal detachment, which can lead to expulsive hemorrhage.
Choroidal effusion, ciliochoroidal effusion, and serous choroidal detachment are used almost synonymously. Choroidal detachment is a broader concept that also includes hemorrhagic types. The overall classification of choroidal detachment includes three groups: idiopathic choroidal detachment, secondary choroidal detachment, and uveal effusion syndrome. Postoperative choroidal detachment belongs to the secondary type. Causes of secondary choroidal detachment include various conditions such as hypotony, choroidal circulatory disturbance, choroidal inflammation, and malignant tumors.
Glaucoma surgery is the most common cause of choroidal detachment. According to the Japanese Glaucoma Guidelines (5th edition), the frequencies of early postoperative complications after trabeculectomy include shallow anterior chamber (0.9–13%), choroidal detachment (5–14%), hyphema (2.7–11%), and wound leak from the conjunctival incision (3.4–14%) 1). In the TVT (Tube versus Trabeculectomy) study, postoperative choroidal effusion was observed in 19% of trabeculectomy cases and 16% of glaucoma drainage implant cases 4). Hemorrhagic choroidal detachment has been reported in 1.2–2.7% of tube shunt surgeries and 0.6–1.4% of trabeculectomies. Choroidal effusion has also been reported in 0–15% of cases after XEN45 gel stent implantation 2).
Intraoperative choroidal effusion also occurs during cataract surgery. In sutureless micro-incision cataract surgery, the incidence is about 0.05% due to the short duration of intraocular pressure reduction. Risk factors include advanced age, hypertension/arteriosclerosis, high intraocular pressure/glaucoma, high myopia, microphthalmos, and Sturge-Weber syndrome.
The frequency of hypotony maculopathy, which can cause postoperative visual impairment, is reported to be 0.9–5%, and the frequency of bleb-related infection is 0.97–5% 1).
QWhat happens if choroidal effusion occurs after glaucoma surgery?
A
Small peripheral choroidal effusions are often asymptomatic and resolve spontaneously. However, large effusions can cause decreased vision and shallow anterior chamber. Most cases improve with conservative treatment using mydriatics and steroids, but severe cases with flat anterior chamber or kissing choroidals require surgical drainage. See “Standard Treatment” section for details.
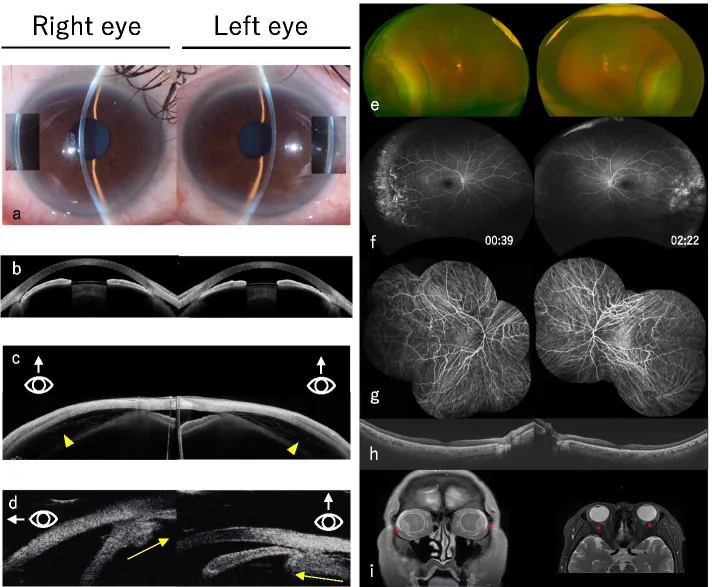
Takahashi S, et al. Multimodal imaging of indapamide-induced bilateral choroidal effusion: a case report. BMC Ophthalmol. 2021. Figure 1. PMCID: PMC8567550. License: CC BY.
Acute phase images showing angle narrowing on slit lamp (a), extremely shallow anterior chamber on anterior segment OCT (b), choroidal effusion (c), anterior displacement of the lens and ciliary body edema on UBM (d), bilateral choroidal effusion on color fundus photography (e), and vascular leakage on fluorescein angiography (f). These correspond to choroidal detachment discussed in section “2. Main Symptoms and Clinical Findings”.
Serous choroidal effusion: Most commonly occurs 2–5 days after surgery. Small peripheral effusions are often asymptomatic. Large effusions present with the following symptoms:
Decreased vision: Due to refractive changes caused by choroidal elevation
Peripheral visual field constriction: Elevated choroid compresses the retina
Myopic shift: Due to anterior displacement of the lens-iris diaphragm
Hemorrhagic choroidal detachment: Suspect if sudden severe eye pain, nausea, and vision loss occur within a few days after surgery1). Presents with sudden intense throbbing pain and immediate vision loss. Pain due to stretching of ciliary nerves may be accompanied by nausea and vomiting.
Intraoperative onset (during cataract surgery): A sudden rise in vitreous pressure with shallow anterior chamber is a sign. Risk of posterior capsule rupture as the posterior capsule elevates; if the anterior chamber becomes extremely shallow, continuing surgery becomes difficult. If the fundus is visible, choroidal folds may be observed.
Clinical Findings (Findings Confirmed by Physician Examination)
Comparison of clinical findings between serous and hemorrhagic types is shown below.
Finding
Serous
Hemorrhagic
Intraocular pressure
Usually low
Usually high
Transillumination (Hagen sign)
Positive
Negative
B-mode ultrasound
Echofree
Hyperechoic
Fundus findings: On ophthalmoscopy, choroidal detachment appears as a smooth, brownish, convex lens-like elevation. In early or mild cases, it is seen as elevation of the pars plana and peripheral choroid, allowing easy visualization of the ora serrata without scleral indentation. Large choroidal detachments present as up to four multiloculated balloon-like elevations separated by vortex vein attachments.
Anterior chamber findings: The anterior chamber may be of normal depth, shallow, or absent. Anterior displacement of the lens due to choroidal detachment causes a shallow anterior chamber.
Findings when complicated by hypotony maculopathy: Persistent hypotony leads to shortening of the axial length, choroidal folds, macular folds, tortuosity of retinal vessels, and optic disc edema 1). If prolonged, it may result in permanent visual impairment.
Secondary glaucoma: Secondary choroidal detachment can cause an acute glaucoma attack. This condition involves angle closure due to anterior displacement of the lens-iris diaphragm, leading to a sudden rise in intraocular pressure.
Postoperative hypotony is the most common cause. According to Starling’s equation, a decrease in intraocular pressure (decrease in interstitial pressure) results in a relative increase in capillary pressure, leading to fluid accumulation in the suprachoroidal space. Increased choroidal capillary permeability due to inflammation also contributes 6).
Fluid accumulation in the suprachoroidal space creates the following vicious cycle:
Postoperative hypotony → fluid accumulation in the suprachoroidal space
Decreased ciliary body function → reduced aqueous humor production → further hypotony
Increased protein concentration in aqueous humor → promotes scarring of the bleb
Onset during cataract surgery is thought to occur due to arteriosclerosis from aging and a sudden drop in intraocular pressure during surgery, leading to a rapid exudation of serous fluid from the short posterior ciliary arteries.
Rapid accumulation of blood in the suprachoroidal space due to rupture of a branch of the posterior ciliary artery. Risk is high with sudden ocular decompression, especially when surgery is initiated from a state of high intraocular pressure. Use of antimetabolites (mitomycin C, 5-FU) also promotes hypotony and contributes 1).
Choroidal detachment is observed as a hard, convex lens-shaped elevation with a smooth surface and a brownish color. A characteristic feature is that the ora serrata can be easily observed without compression. In large choroidal detachments, multilobular elevations separated by vortex vein attachments are seen.
It allows observation of the separation between the ciliary body and sclera, and is used to visualize anterior rotation of the ciliary body. It is useful for detailed evaluation of the anterior segment.
Expulsive hemorrhage: It occurs acutely during surgery and leads to loss of the anterior chamber. The presence or absence of choroidal folds is useful for differentiating from choroidal effusion. Expulsive hemorrhage is often accompanied by sudden extrusion of intraocular contents and has a poor prognosis.
Irrigation misdirection syndrome (IMS): It is an increase in vitreous pressure that occurs during cataract surgery, but is distinguished from choroidal effusion by the absence of choroidal folds in the fundus.
Malignant glaucoma (aqueous misdirection): Suspect when there is a shallow anterior chamber but no corresponding hypotony, choroidal detachment, or suprachoroidal hemorrhage. It is a condition in which aqueous humor flows into the vitreous cavity, causing the anterior chamber to shallow. Treatment options include mydriatics, aqueous suppressants, and vitrectomy.
Posterior scleritis: B-mode ultrasound shows thickening of the posterior sclera and choroid, and a T-sign due to retrobulbar tissue edema is characteristic. It is more common in middle-aged women, often unilateral, with eye pain and vision loss, and frequently associated with anterior scleritis or uveitis.
The basic principle of prevention is to minimize intraoperative and postoperative hypotony1).
Trabeculectomy: Place multiple sutures on the scleral flap and manage intraocular pressure postoperatively with laser suture lysis (LSL). Placing many sutures intraoperatively to reduce overfiltration is a common management method1).
Many choroidal effusions resolve with conservative treatment. Some cases improve spontaneously due to scarring of the subconjunctival and periscleral flap tissues1).
Mydriatics (atropine sulfate hydrate): Rotate the lens-iris diaphragm posteriorly to deepen the anterior chamber.
Pressure patch: Accurate compression of the scleral flap may improve overfiltration1).
Severe cases: Oral prednisolone (1 mg/kg, tapered) is used in combination 5)
When the anterior chamber is lost: Air or viscoelastic material is injected into the anterior chamber to reform it
Management during cataract surgery: If the anterior chamber can be formed by injecting Healon V® (high-viscosity sodium hyaluronate) into the anterior chamber, surgery can be continued. In micro-incision cataract surgery, the wound naturally closes as intraocular pressure rises, so waiting 20–30 minutes may deepen the anterior chamber and allow surgery to continue. If Healon V® is pushed back through the wound, surgery should be discontinued; if the anterior chamber cannot be formed, surgery is resumed the next day or later.
If intraoperative choroidal effusion occurs in one eye, the risk is similarly high in the fellow eye; therefore, surgery on the fellow eye should preferably be performed under general anesthesia, or referral to a facility where general anesthesia is available should be considered.
Persistent choroidal effusion unresponsive to conservative treatment
Technique: A full-thickness scleral incision is made 3.5–4.5 mm posterior to the limbus to drain fluid from the suprachoroidal space. During drainage, the anterior chamber is reformed by injecting irrigation fluid or viscoelastic material 5).
Drainage of hemorrhagic choroidal detachment: Bleeding may be absorbed spontaneously, but if drainage is performed, it is advisable to wait 7–10 days until the blood has liquefied 1).
For hypotony associated with overfiltration, the following interventions are considered stepwise 1):
Transconjunctival scleral flap suture: A method of suturing the scleral flap directly through the conjunctiva with nylon thread, which has shown long-term effectiveness in treating hypotony maculopathy1)
Autologous blood injection: There are reports of improvement in hypotony maculopathy by injecting autologous blood into and around the filtering bleb. However, it may cause a sudden increase in intraocular pressure1)
Open scleral flap suture: If the above methods do not improve the condition, the conjunctiva is reopened and the scleral flap is sutured under direct visualization1)
Scleral window procedure: Drainage of fluid accumulated in the suprachoroidal space when marked choroidal detachment is present1)
QDoes choroidal effusion resolve on its own?
A
Many serous choroidal effusions resolve with postoperative wound healing and scarring of the subconjunctival tissue. Most cases improve with conservative treatment using mydriatics and steroid eye drops. However, large or persistent choroidal effusions may require surgical drainage. Hemorrhagic choroidal detachment is more severe than serous and requires more aggressive intervention.
QWhat is kissing choroidal?
A
Kissing choroidal (appositional choroidal detachment) is a condition in which opposing choroidal detachments become so elevated that they touch each other from the optic nerve to the lens. It is accompanied by anterior chamber loss and carries a high risk of retinal blood flow impairment and corneal endothelial damage, making it an absolute indication for surgical drainage.
Histologically, the choroid is divided into four layers from the outside: the suprachoroid, vascular layer, choriocapillaris, and Bruch’s membrane. The choroid is firmly attached to the sclera at the sites where the optic nerve and posterior ciliary arteries enter the eye and where the vortex veins exit the eye. The attachment between the suprachoroid and sclera is looser anteriorly and tighter posteriorly. These attachment sites determine the multilobular morphology of choroidal detachment.
The space between the sclera and choroid is called the suprachoroidal space, and the suprachoroid, a thin pigmented connective tissue membrane, exists in this space. Because the anterior attachment between the suprachoroid and sclera is loose, early choroidal detachment is observed as elevation of the pars plana and peripheral choroid.
In normal choroidal capillaries, the balance of hydrostatic pressure is maintained. When this balance is disrupted by various causes, albumin in the blood leaks out of the capillaries, and exudate accumulates in the suprachoroidal space 6).
When intraocular pressure is low, the interstitial pressure (≈ intraocular pressure) decreases, causing capillary pressure to become relatively high, and fluid accumulates in the suprachoroidal space. Once choroidal effusion forms, serum containing proteins accumulates in the suprachoroidal space, and the reabsorption of the uvea is limited by the balance of colloid osmotic pressure. In choroidal circulatory disorders, leakage from choroidal capillaries increases; in choroidal inflammation, capillary permeability increases, and the liquid components of blood leak out of the vessels.
Branches of the posterior ciliary arteries (short posterior ciliary arteries) rupture due to sudden ocular decompression, and blood rapidly accumulates in the suprachoroidal space. A sudden drop in intraocular pressure from a state of high intraocular pressure is the greatest risk. In elderly patients with arteriosclerosis, the vascular walls are more fragile, and the threshold for rupture is lowered. If it occurs during surgery, it can lead to expulsive hemorrhage, a serious complication that causes extrusion of intraocular contents.
If choroidal detachment persists for a long time, the barrier mechanism of the retinal pigment epithelium (RPE) decompensates, resulting in the accumulation of subretinal fluid and non-rhegmatogenous retinal detachment. If the accompanying non-rhegmatogenous retinal detachment is long-standing and the retinal pigment epithelium under the fovea is damaged, even if anatomical improvement is achieved by surgery, visual improvement is difficult.
In nanophthalmos, abnormal thickening of the sclera compresses the vortex veins, obstructing drainage from the vortex veins and causing accumulation of subretinal fluid. It has been reported that scleral thickening is due to abnormal arrangement of collagen fibers.
In uveal effusion syndrome, abnormal sclera impairs the transscleral outflow of protein-rich fluid from the choroidal extravascular space 6). Protein-rich exudate accumulates in the suprachoroidal space, and fluid retention persists due to colloid osmotic pressure differences. This condition recurs with remissions and exacerbations, and prolonged choroidal detachment gradually causes chorioretinal atrophy and decreased function of the retinal pigment epithelium, leading to visual impairment.
In 1983, Gass reported that partial sclerectomy and scleral window surgery are effective for uveal effusion syndrome, and in 1990 reported that about 56% of cases showed improvement of two or more lines of visual acuity. However, if non-rhegmatogenous retinal detachment has been long-standing, visual recovery is limited even if anatomical improvement is achieved by surgery.
In addition, mucopolysaccharide metabolic disorders such as Hunter syndrome can also cause scleral thickening and secondary choroidal detachment.
Minimally invasive glaucoma surgery tends to have a lower risk of choroidal effusion compared to traditional filtration surgery. However, although the small lumen (approximately 45 μm) of the XEN45 gel stent theoretically can avoid early postoperative hypotony, choroidal effusion is still reported 2).
Cassottana et al. (2023) reported a case of bilateral choroidal effusion after XEN45 implantation in an 84-year-old man. The right eye improved within one month with mydriatics and steroids, but the left eye was resistant to conservative treatment and required transscleral drainage after two months. Advanced age, preoperative use of multiple medications, and intraocular pressure below 10 mmHg within the first postoperative week were identified as major risk factors 2).
Intraocular pressure below 10 mmHg within 24 to 48 hours after surgery is considered a poor prognostic factor 2).
Choroidal effusion in one eye may be a risk factor for the same surgery in the contralateral eye 2). In cataract surgery as well, if intraoperative choroidal effusion occurs in one eye, the risk is similarly high in the contralateral eye, so surgery under general anesthesia or transfer to a facility capable of general anesthesia may be considered.
Shaheen et al. (2023) reported a case of acute serous and hemorrhagic choroidal effusion caused by topical dorzolamide. A 78-year-old man developed choroidal effusion in the left eye two days after starting dorzolamide-timolol combination drops, which completely resolved within four days after discontinuing dorzolamide and using prednisolone 1% and atropine 1% eye drops. He had a similar episode ten years earlier, confirming the reproducibility of an idiosyncratic reaction 3).
In pseudophakic eyes, the absence of a lens barrier may increase drug penetration into the vitreous, potentially raising the risk of onset 3). Some cases have not developed choroidal effusion with oral carbonic anhydrase inhibitors (acetazolamide, methazolamide), suggesting that the pathophysiology may differ between topical and systemic administration 3).
For uveal effusion syndrome, the efficacy of partial sclerectomy and scleral window surgery has been reported. Gass reported visual improvement of two or more lines in approximately 56% of cases. However, if the accompanying non-rhegmatogenous retinal detachment is prolonged and the subfoveal retinal pigment epithelium is damaged, visual improvement may be difficult even if anatomical improvement is achieved by surgery.
Advances in imaging diagnosis: Standardization of early detection and quantitative evaluation of postoperative choroidal effusion using OCTA and wide-angle OCT is expected. It is becoming possible to evaluate micro-effusions that are difficult to detect with conventional B-mode ultrasound.
Management guidelines by surgical procedure: With the spread of minimally invasive glaucoma surgery, establishment of incidence rates and management guidelines specific to each procedure for choroidal effusion is required.
Contralateral eye risk assessment: Exploring biomarkers for risk prediction in the contralateral eye after unilateral onset is a future research challenge.
Elucidation of drug-induced mechanisms: It has been suggested that the pathophysiology may differ between topical and systemic administration of carbonic anhydrase inhibitors, and cases have been reported where choroidal effusion did not occur with oral acetazolamide3). Improved safety in drug selection is expected.
QCan choroidal effusion occur even with minimally invasive glaucoma surgery?
A
Minimally invasive glaucoma surgery has a lower risk compared to traditional filtration surgery, but choroidal effusion has been reported in 0–15% of cases even with procedures such as the XEN gel stent. The risk is higher in elderly patients, those using many glaucoma medications before surgery, and when intraocular pressure drops below 10 mmHg early after surgery. See the “Causes and Risk Factors” section for details.
Cassottana P, Toma C, Maltese C, Villa V, Ricciarelli R, Traverso CE, et al. A Case of Bilateral Choroidal Effusion after XEN Gel Stent Implantation. Gels (Basel, Switzerland). 2023;9(4). doi:10.3390/gels9040276. PMID:37102888; PMCID:PMC10138104.
Shaheen A, Schultis S, Magraner M, Correa ZM, Yannuzzi NA, Greenfield DS. Acute serous and hemorrhagic choroidal effusion associated with topical dorzolamide therapy. American journal of ophthalmology case reports. 2023;31:101866. doi:10.1016/j.ajoc.2023.101866. PMID:37323588; PMCID:PMC10265454.
Gedde SJ, Herndon LW, Brandt JD, et al. Postoperative complications in the Tube Versus Trabeculectomy (TVT) study during five years of follow-up. Am J Ophthalmol. 2012;153(5):804-814.e1. doi:10.1016/j.ajo.2011.10.024. PMID: 22244522.
Schrieber C, Liu Y. Choroidal effusions after glaucoma surgery. Curr Opin Ophthalmol. 2015;26(2):134-142. doi:10.1097/ICU.0000000000000131. PMID: 25643198.