Glaucoma is a leading cause of irreversible visual impairment worldwide. Elevated intraocular pressure (IOP) is the most important risk factor for glaucoma, and impaired aqueous humor outflow is its main cause4).
Aqueous humor is produced by the ciliary body and drains through the conventional outflow pathway (trabecular meshwork → Schlemm’s canal → collector channels → aqueous veins → episcleral veins) and the unconventional outflow pathway (uveoscleral outflow). The conventional pathway accounts for over 80% of total outflow4). The juxtacanalicular connective tissue (JCT) and Schlemm’s canal are the main sites of outflow resistance1)4).
With the recent rise of MIGS, interest in imaging diagnosis of the aqueous humor outflow pathway has increased. Preoperative evaluation of the outflow pathway may allow identification of optimal treatment targets and contribute to personalized surgical selection.
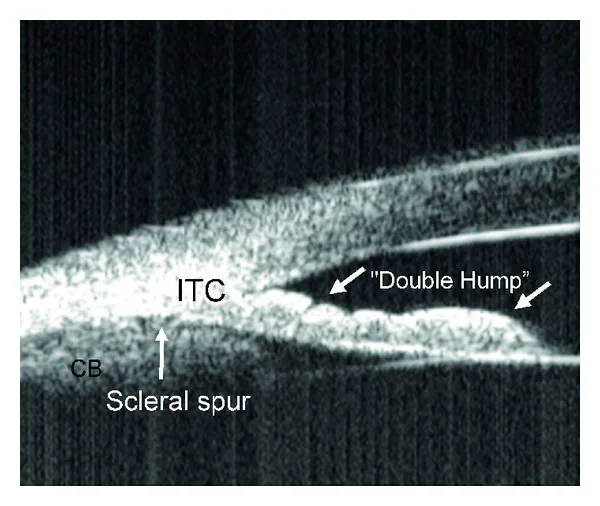
Syril Dorairaj; James C Tsai; Tomas M Grippo. Changing Trends of Imaging in Angle Closure Evaluation. ISRN Ophthalmol. 2012;2012:597124. Figure 3. PMCID: PMC3914273. License: CC BY.
Ultrasound biomicroscopy shows the double-hump sign typical of plateau iris configuration. The cross-section shows the anterior displacement of the peripheral iris and the positional relationship of the ciliary processes.
Gonioscopy is the gold standard for evaluating the anterior chamber angle2). Complementary imaging methods include ultrasound biomicroscopy, AS-OCT, and angle photography.
Ultrasound Biomicroscopy (UBM)
Principle: B-mode ultrasound using high-frequency ultrasound of 50–100 MHz provides cross-sectional images of the anterior segment3). It is a contact examination requiring topical anesthesia.
Advantages: Since it does not use light, angle imaging is possible in dark room mydriatic conditions. It can visualize the posterior surface of the iris and ciliary body, and is useful for diagnosing plateau iris and ciliary body tumors3).
Limitations: It is a contact method requiring examiner proficiency. Resolution is inferior to AS-OCT. Lighting conditions and accommodation affect image quality.
Anterior Segment OCT (AS-OCT)
Principle: Uses low-coherence interferometry to obtain high-resolution cross-sectional images of anterior segment structures3). Non-contact, non-invasive, and can be performed in a short time.
Advantages: Excellent resolution and quantifiability, can scan all four quadrants at once. SS-OCT enables 360-degree evaluation and quantification of angle closure extent.
Quantitative parameters: AOD, trabecular-iris space area (TISA), iris-trabecular contact (ITC) index. For every 0.1 mm decrease in AOD750, the odds of angle closure increase by 3.27 times.
Limitations: Cannot evaluate pigment or neovascularization3). Difficult to differentiate organic angle closure. Identification of the scleral spur is impossible in 15–28% of cases.
AS-OCT tends to detect more angle closure than gonioscopy2). In a study of 342 eyes by Nolan et al., 66.7% were diagnosed as closed by AS-OCT and 44.4% by gonioscopy. This is thought to be because AS-OCT uses infrared light and is not affected by inadvertent compression during gonioscopy that can open the angle. However, AS-OCT should not replace gonioscopy but be used complementarily2).
EyeCam (Clarity Medical Systems) is a contact handheld device that can obtain clear angle images in over 98% of patients. Agreement with gonioscopy is good (κ=0.72–0.76), but the detection rate of angle closure is higher with EyeCam (27%) than with gonioscopy (13.8%). A drawback is that indentation cannot be performed.
The NGS-1 automatic gonioscope provides 360-degree panoramic angle images. It captures multifocal high-resolution photographs, but 22.5% are of low quality and it has been reported to have lower sensitivity than gonioscopy.
QWhich is better, AS-OCT or ultrasound biomicroscopy?
A
The two are complementary and cannot be directly compared. AS-OCT is non-contact, offers superior resolution and quantifiability, and is easy to use in daily practice 3). On the other hand, ultrasound biomicroscopy can visualize the posterior iris and ciliary body, and is essential for diagnosing plateau iris and ciliary body tumors 3). The mean values, reproducibility, sensitivity, and specificity for detecting narrow angles are reported to be similar between the two.
Ultrasound biomicroscopy evaluation: In primary open-angle glaucoma eyes, the SC meridional diameter, coronal diameter, and TM thickness are all significantly smaller compared to normal eyes. In pediatric glaucoma, the SC diameter is significantly smaller in glaucomatous eyes (64.9 μm) than in non-glaucomatous eyes (142 μm).
AS-OCT evaluation: Quantification of SC cross-sectional area (CSA) is possible. The SC area in primary open-angle glaucoma eyes (11,332 μm²) is significantly smaller than in normal eyes (13,991 μm²). SC area correlates significantly with intraocular pressure.
Age-related changes: SC size and detection rate significantly decrease with age. TM thickness increases with age.
Differences between devices: CSA varies depending on the OCT device. CSA measured by SD-OCT is larger than that measured by SS-OCT.
SC Changes with Treatment
Eye drops: 8 hours after instillation of 0.004% travoprost, the mean SC area increases by more than 90%. Pilocarpine also dilates SC. Timolol-dorzolamide combination does not change SC.
After SLT: SC cross-sectional area and volume increase significantly. There is a significant positive correlation between SC area increase and intraocular pressure reduction. In young open-angle glaucoma, identification of SC is a strong predictor of SLT success.
After canaloplasty: SC height increases by 351% and width by 144%.
After trabeculectomy: In PACG eyes, SC diameter and area increase significantly. SC changes correlate with the rate of intraocular pressure reduction.
There are few reports on in vivo imaging evaluation of collector channels (CC). Li et al. used enhanced depth imaging OCT to show that the number of collector channels is significantly higher on the nasal side (5.5±1.4) than on the temporal side (3.3±1.1). SC cross-sectional area was significantly larger in regions with more collector channels (r=0.6).
QCan imaging of Schlemm's canal be used clinically?
A
It is still at the research stage, but the potential for clinical application is expanding. SC area correlates with intraocular pressure, and morphological changes of SC in response to eye drops and surgery have been reported. In particular, identification of SC before SLT may be a predictor of SLT success, which is clinically important. However, the detection rate of SC varies with age (73.8% in those aged 15 years and older vs. 53.6% in those aged 7 years and younger), and attention should be paid to differences in CSA between devices.
Imaging of Intrascleral and Conjunctival Vasculature
Anterior segment OCT angiography (AS-OCTA) enables evaluation of conjunctival vessels and deep intrascleral vessels. In the deep vascular layer (corresponding to episcleral veins and aqueous veins), vascular density, vessel length density, diameter index, and fractal dimension differ among quadrants.
Observation of aqueous veins may be useful for predicting the efficacy of MIGS. It has been reported that the intraocular pressure reduction rate after iStent surgery correlates with the grade of aqueous vein flow.
6. Anatomy of Aqueous Outflow Pathways and Outflow Resistance
The conventional outflow pathway follows the route: anterior chamber → trabecular meshwork → Schlemm’s canal → collector channels → aqueous veins → episcleral veins → systemic circulation. The trabecular meshwork is divided into three parts from the anterior chamber side: uveal trabecular meshwork, corneoscleral trabecular meshwork, and juxtacanalicular connective tissue (JCT) 1).
Most of the aqueous outflow resistance exists between the JCT and the inner wall endothelium of Schlemm’s canal (SCE) 1). Aqueous humor flows through microscopic discontinuities in the SCE basement membrane, via giant vacuoles and pores, into the lumen of Schlemm’s canal 1). Aqueous outflow is not uniform; there are segmental regions of high and low flow 1). Glaucomatous eyes have more low-flow regions 1).
The extracellular matrix of the JCT in glaucomatous eyes is about 20 times stiffer than in normal eyes 1). Loss of trabecular meshwork cells leads to loss of IOP homeostasis response, and cell replenishment restores the response 1).
Alternative Outflow Pathway (Uveoscleral Outflow Pathway)
In the alternative outflow pathway, aqueous humor enters the ciliary body stroma from the intercellular spaces at the anterior ciliary body, travels posteriorly along the uvea, and exits the eye through the sclera. Outflow rate is reported to be 0.2–0.4 μL/min. While the conventional pathway is pressure-dependent, the alternative pathway is pressure-independent 4).
QWhere does aqueous outflow resistance exist?
A
Most of the aqueous outflow resistance is localized in the deepest part of the juxtacanalicular connective tissue (JCT), specifically in a 1–2 μm thick region consisting of the inner wall endothelium of Schlemm’s canal (SCE) and its basement membrane 1). Aqueous humor encounters little resistance in the intertrabecular spaces of the uveal and corneoscleral trabecular meshwork. In glaucomatous eyes, the stiffness of the extracellular matrix in this region is increased to about 20 times normal, which is considered a contributing factor to increased outflow resistance 1).
Deep learning systems have been developed to automatically detect angle closure from AS-OCT images. Fu et al. reported an area under the curve (AUC) of 0.96, sensitivity of 0.9, and specificity of 0.92. This is expected to be applied for screening patients at high risk of angle closure.
AS-OCTA enables imaging of anterior segment microvasculature without contrast agents. Visualization of deep vessels is increasingly allowing evaluation of pathways beyond the collector channels (episcleral veins and aqueous veins). In the future, its utility in assessing outflow pathways before MIGS and predicting postoperative outcomes is expected to be investigated.
Advances in OCT technology have enabled in vivo measurement of Schlemm’s canal, allowing monitoring of morphological changes in SC in response to medications, laser, and surgery. Clinical applications such as predicting SLT success and evaluating canaloplasty are progressing.
Acott TS, Vranka JA, Keller KE, Raghunathan V, Kelley MJ. Normal and glaucomatous outflow regulation. Progress in retinal and eye research. 2021;82:100897. doi:10.1016/j.preteyeres.2020.100897. PMID:32795516; PMCID:PMC7876168.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.