Eales disease was first reported in 1880 by the British ophthalmologist Henry Eales as recurrent vitreous hemorrhage in healthy young men. It is an idiopathic occlusive retinal vasculitis characterized by peripheral retinal phlebitis, vascular occlusion, and neovascularization.
The incidence varies greatly by region. It is rare in North America, but relatively common in areas with high tuberculosis infection rates such as India, the Middle East, and Asia 1). It predominantly affects men in their 20s to 30s, with a male-to-female ratio of about 20:1. Up to 87% of cases are bilateral 1).
It is a diagnosis of exclusion, confirmed after ruling out other retinal vasculitis, systemic diseases, and diabetes.
QHow rare is Eales disease?
A
It is very rare in North America, but relatively common in tuberculosis-endemic regions such as India and the Middle East 1). The male-to-female ratio is about 20:1, with a strong male predominance, and up to 87% of cases are bilateral.
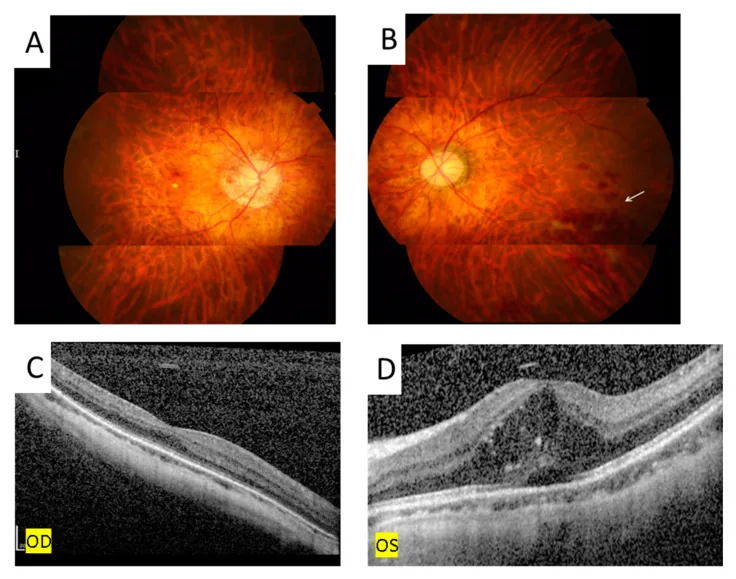
Ping-Ping Meng; Chun-Ju Lin; Ning-Yi Hsia; Chun-Ting Lai; Henry Bair; Jane-Ming Lin; Wen-Lu Chen; Yi-Yu Tsai. Use of Ultra-Widefield Fluorescein Angiography to Guide the Treatment to Idiopathic Retinal Vasculitis, Aneurysms, and Neuroretinitis—Case Report and Literature Review. Medicina (Kaunas). 2022 Oct 16; 58(10):1467. Figure 5. PMCID: PMC9611749. License: CC BY.
Fundus photography showed retinal hemorrhage ((B), arrow) and OCT disclosed subretinal and intraretinal fluid with hyperreflective material over the left eye (D). There is no retinal hemorrhage (A) nor macular edema (C) over the right eye.
In the early stage, the disease is often asymptomatic, and there are no subjective symptoms during the peripheral phlebitis phase. As the disease progresses, the following symptoms appear.
Floaters: Acute onset of floating sensation due to vitreous hemorrhage. It may be accompanied by sudden photopsia1).
Blurred vision: There is a report of persistent blurred vision and floaters for 2 months as the main complaint4).
The Saxena classification subdivides the disease into 7 stages from Ia to IVb. Ia/Ib: peripheral phlebitis; IIa: ischemia/non-perfusion; IIb: neovascularization; IIIa/IIIb: degree of vitreous hemorrhage; IVa/IVb: extent of TRD.
Macular edema is observed in 58.2% of cases4) and is an important complication directly linked to visual prognosis.
Fluorescein angiography (FA) can evaluate venous leakage in active inflammation, wall staining in the chronic sclerotic phase, and the extent of non-perfusion areas.
The cause is unknown and considered idiopathic, but a hypersensitivity reaction to tuberculous protein is the most likely etiological theory.
Association with tuberculosis: The MPB64 gene of Mycobacterium tuberculosis is detected by PCR in 50–70% of epiretinal membranes. However, bacterial culture is negative, suggesting that an immunological hypersensitivity reaction to non-viable bacteria or DNA fragments is involved in the pathogenesis3).
Role of VEGF: High concentrations of VEGF, IL-6, IL-8, and MCP-1 are detected in the vitreous, promoting pathological angiogenesis3).
Immunological predisposition: Associations with HLA-B5, DR1, DR4, low glutathione, and C3 complement changes have been reported4).
Coagulation abnormalities: Heterozygous factor V Leiden mutation increases thrombotic risk approximately 7-fold and may contribute to vascular occlusion4).
Cocaine involvement: There are case reports of Eales disease triggered by cocaine abuse as an immunological trigger4).
QWhat is the relationship between Eales disease and tuberculosis?
A
PCR for Mycobacterium is reported positive in 50–70% of cases of epiretinal membrane, but the bacteria are not detected by culture 3). The pathogenesis is thought to be an immunological hypersensitivity reaction to non-viable bacteria or DNA fragments, rather than direct infection by live bacteria. Therefore, combination therapy with anti-tuberculosis drugs is recommended in patients with a positive Mantoux test.
Fluorescein angiography (FA): Most important test. Evaluates venous leakage (active inflammation), wall staining (sclerosis), and extent of non-perfusion areas. Essential for determining treatment indication and laser photocoagulation area.
It is a diagnosis of exclusion, made after ruling out systemic diseases such as diabetes, sarcoidosis, and SLE through blood tests and imaging1). Fluorescein angiography (FA) is the most important test, confirming peripheral periphlebitis, non-perfusion areas, and neovascularization.
Oral steroids are the first-line treatment. A regimen starting with prednisone 40 mg/day and gradually tapering is used 1). There is also a report of achieving a final visual acuity of 20/20 with dexamethasone 1 mg/kg/day tapered over 4 months 4). A large study by Biswas et al. (500 patients, 898 eyes) showed that steroid administration during the acute inflammatory phase significantly improved visual acuity2)4).
For patients with a positive Mantoux test, antitubercular drugs are added. A regimen of RIPE (rifampicin, isoniazid, pyrazinamide, ethambutol) for 4 months, followed by isoniazid alone for 5 months, for a total of 9 months, is used 2)3). The international consensus (COTS guidelines) serves as a reference for the ATT initiation algorithm when tuberculosis infection is suspected 2).
Treatment of the Ischemic and Proliferative Phases
Retinal photocoagulation (PRP): The mainstay treatment for the ischemic phase. Sectoral photocoagulation has been reported to induce regression of neovascularization in over 89% of cases. In one case, neovascularization regressed after three sessions of panretinal photocoagulation1). A synergistic effect of steroids and photocoagulation is expected 1).
Intravitreal anti-VEGF injection: Bevacizumab can promote regression of neovascularization and absorption of vitreous hemorrhage. However, there is a risk of promoting tractional retinal detachment (TRD) formation 3). In cases unresponsive to ranibizumab, aflibercept (which binds VEGF-A, VEGF-B, and PlGF) has been used, with case reports maintaining 20/25 to 20/20 vision over long periods (43 months, 28 months) 3).
Vitrectomy (PPV): Indicated for vitreous hemorrhage persisting for more than 3 months, or for TRD threatening the macula. There are reports of maintaining 20/20 vision even after 33 years of follow-up 2).
QWhat is the visual prognosis for Eales disease?
A
With early and appropriate treatment, a good visual prognosis can be expected. There are reports of maintaining 20/20 vision for 33 years after vitrectomy2). On the other hand, delayed treatment can lead to tractional retinal detachment, neovascular glaucoma, cataract, and optic atrophy4).
The pathology of Eales disease is understood as a stepwise progression starting from peripheral periphlebitis 1)2).
Stage 1 (Inflammation): Inflammatory cell infiltration and periphlebitis occur along the peripheral retinal veins. PCR for Mycobacterium tuberculosis is positive in 50–70% of epiretinal membranes, but cultures do not detect the bacteria 3). It is thought that non-viable organisms or DNA fragments activate the host immune system, causing reactive inflammation 1).
Stage 2 (Ischemia): Inflammation-induced vascular wall damage leads to thrombus formation and vascular occlusion. Capillary non-perfusion areas expand, and ischemia progresses.
Stage 3 (Neovascularization): Large amounts of VEGF are secreted from the ischemic retina3). In addition to VEGF, high concentrations of IL-6, IL-8, and MCP-1 are detected in the vitreous, forming a sustained loop of pathological neovascularization and inflammation 3). Sea-fan-shaped neovascularization appears at the border of ischemia, and repeated bleeding from fragile new vessels occurs.
Eales disease and tuberculosis-related retinal vasculitis (TRV) are clinically almost indistinguishable, and it has been suggested that they may be on a spectrum 2).
Cocaine promotes thrombus formation through vasoconstriction and endothelial damage, and may act as an immunological trigger 4). Heterozygosity for the factor V Leiden mutation increases thrombotic risk approximately 7-fold and is a genetic risk factor for vascular occlusion 4).
7. Latest Research and Future Perspectives (Investigational Reports)
International consensus guidelines (COTS) are organizing the management algorithm for TRV (tuberculosis-related retinal vasculitis) 2). Eales disease and TRV have been treated as separate diseases, but their boundary is being reconsidered, and the continuity of clinical features and etiology is being discussed 2).
Cases have been reported where aflibercept was used for Eales disease refractory to ranibizumab, maintaining 20/25 after 43 months and 20/20 with repeated administration every 3 months for 28 months 3). This is the first case report of aflibercept use for Eales disease, and by simultaneously binding VEGF-A, VEGF-B, and PlGF, it may be effective in cases resistant to existing anti-VEGF drugs 3).
New risk factors such as cocaine abuse and factor V Leiden mutation have been identified in individual cases 4), and further elucidation of immunological and genetic predispositions is expected in the future.
Horvath D, Aljameey U, Douglas E.. Double Trouble: Eales Disease in a Background of Paradoxical Embolism. Cureus. 2023;15(9):e44708. doi:10.7759/cureus.44708. PMID:37809206; PMCID:PMC10552784.
Kiryakoza LC, Sengillo JD, Fernandez MP, Pathengay A, Albini TA, Flynn HW Jr. Retinal Vasculitis in the Setting of Mycobacterium tuberculosis Exposure: Clinical Course and Management of Three Cases. Case reports in ophthalmology. 2025;16(1):18-26. doi:10.1159/000542075. PMID:39981526; PMCID:PMC11842010.
Hsia NY, Lin CJ, Lai CT, Bair H, Chang CH, Lin JM, et al. Intravitreal Aflibercept as a Rescue Therapy for Retinal Neovascularization and Macular Edema due to Eales Disease. Case reports in ophthalmological medicine. 2021;2021:8887362. doi:10.1155/2021/8887362. PMID:33628552; PMCID:PMC7892226.
Iannetti L, Scarinci F, Alisi L, Beccia A, Cacciamani A, Saturno MC, Gharbiya M.. Cocaine Abuse as an Immunological Trigger in a Case Diagnosed with Eales Disease. Medicina (Kaunas). 2023;59(1):169. doi:10.3390/medicina59010169. PMID:36676793; PMCID:PMC9865688.
Saxena S, Kumar D. A new staging system for idiopathic retinal periphlebitis. Eur J Ophthalmol. 2004;14(3):236-239. doi:10.1177/112067210401400308. PMID:15206649.
Goel N, Kumar V, Seth A, Ghosh B. Pattern of macular involvement in Eales’ disease. J Ophthalmic Inflamm Infect. 2011;1(3):109-116.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.