Rhegmatogenous retinal detachment (RRD) is a condition in which a tear forms in the retina, allowing liquefied vitreous to enter the subretinal space and separate the neurosensory retina from the retinal pigment epithelium (RPE) layer. The term “rhegmatogenous” is derived from the Greek word for “tear.”
There are three types of retinal detachment. Rhegmatogenous retinal detachment (RRD) is the most common, distinguished from tractional retinal detachment (TRD: mechanical traction by proliferative membranes) and exudative retinal detachment (ERD: accumulation of exudative fluid from choroidal and retinal vessels). This article focuses on rhegmatogenous retinal detachment.
Exudative retinal detachment does not involve a tear, and shifting fluid that moves with changes in body position is characteristic. Treatment primarily targets the underlying disease, which is fundamentally different from rhegmatogenous retinal detachment.
The concept of repair by closing the tear was established by Jules Gonin in the 1920s. Before that, the cure rate was less than 5%, but Gonin’s ignipuncture (thermocoagulation) improved it to 30–60%. Subsequent developments are as follows:
1949: Ernst Custodis reported the use of polyviol buckles
1950s: Charles Schepens popularized silicone rubber materials, indirect ophthalmoscopy, and cryotherapy, establishing the basis of scleral buckling surgery
Harvey Lincoff: Established Lincoff’s rules for retinal break localization
Late 1960s: Robert Machemer developed closed vitrectomy (PPV)
2002 onward: 25G microincision vitrectomy surgery (MIVS) emerged, and recently ultra-small incision with 27G is advancing
Currently, the primary success rate exceeds 90%, and with multiple surgeries reaches 98%.
Incidence: 1 to 1.5 per 10,000 population per year (0.01–0.015%)2)
Bilaterality: Approximately 10%
Familial occurrence: Approximately 20%
Age distribution: Bimodal. Peak in the 20s (shallow detachment due to atrophic holes within lattice degeneration) and peak in the 50s (bullous detachment due to flap tears associated with acute posterior vitreous detachment)
Association with myopia: Myopia accounts for 40–80% of cases
Increasing incidence: German registry data show an increase in annual incidence from 15.6 to 24.8 per 100,000 population, attributed to aging, increasing myopia prevalence, and rising number of cataract surgeries 2)
Risk after cataract surgery: 20–40% of RRD cases have a history of cataract surgery. Postoperative RRD risk is approximately 0.21% (about 1 in 500), with a decreasing trend due to improved surgical techniques 2)
Traumatic: Accounts for about 10% of all RRD cases, more common in young men2)
The incidence is 1–1.5 per 10,000 population per year, making it a relatively rare disease. However, in regions or populations with a high prevalence of myopia, the number of cases tends to increase. About 10% of cases occur in both eyes, so regular observation of the fellow eye is important for patients who have undergone surgery in one eye.
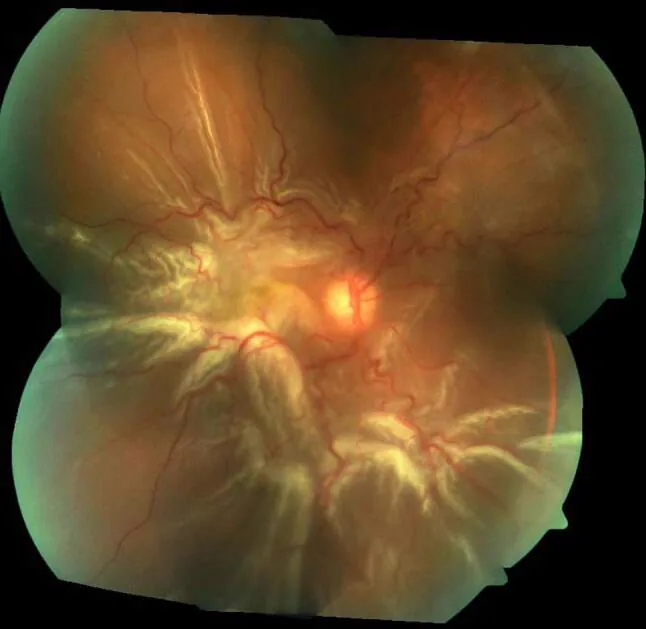
Xiong J, et al. A review of rhegmatogenous retinal detachment: past, present and future. Wien Med Wochenschr. 2025. Figure 3. PMCID: PMC12031774. License: CC BY.
Photopsia: Caused by vitreous traction on the retina. It intensifies in dark environments, occurs even with eyes closed, and is induced by eye movements. Photopsia occurs on the opposite side of the tear, so questioning about the location of occurrence helps estimate the position of the causative tear.
Visual field defect: Occurs on the opposite side of the detachment. Patients may report “a curtain coming down,” “cannot see the edge in the middle,” or “eyelid drooping,” which can be mistaken for progression of glaucoma or ptosis.
Intraocular pressure: Generally decreased. More pronounced decrease when accompanied by choroidal detachment.
Schwartz syndrome: Retinal detachment with elevated intraocular pressure. Caused by outer segments of photoreceptors shed from the detached retina clogging the trabecular meshwork.
Shafer’s sign: Tobacco dust-like pigment (from retinal pigment epithelial cells) floating in the anterior vitreous. An important finding strongly suggesting a retinal tear.
Anterior chamber findings: Normal or only slight increase in cells/flare (useful for differentiation from inflammatory diseases).
Morphology and Predilection Sites of Retinal Breaks
Formed when vitreous traction completely detaches the flap of a tear. The detached flap (operculum) floats in the vitreous cavity.
Progression is relatively slow because traction is relieved. However, liquefied vitreous can easily flow in through the enlarged hole.
Atrophic Hole
Caused by atrophic changes in the retina within lattice degeneration. Not accompanied by an operculum.
Common in young people, women, and high myopia. Progression is often slow because vitreous traction is absent.
The predilection site for retinal tears is the peripheral retina, accounting for two-thirds of all cases. By quadrant: superotemporal 60%, inferotemporal 15%, superonasal 15%, inferonasal 10%.
QShould I see a doctor immediately if I see flashes of light?
A
Photopsia is a sign of retinal traction associated with posterior vitreous detachment and can be a precursor to retinal tear formation. Especially if it occurs simultaneously with floaters or is accompanied by visual field defects, same-day consultation is recommended. Retinal tears are found in 5.4–8% of patients presenting with acute PVD symptoms, and in two-thirds of cases with vitreous hemorrhage. 2)
The development of rhegmatogenous retinal detachment requires two absolute conditions: (1) the presence of a hole in the retina, and (2) liquefaction of the vitreous. For a retinal hole to occur, there must be a thinned degenerative area in the retina, or vitreous traction or strong external force applied to the eye.
Myopia: The greatest risk factor, involved in 40–80% of all RRD cases. Mild myopia (-1 to -3 D) increases risk about 4-fold, and myopia over -3 D increases risk about 10-fold. 2) The main mechanism is thinning of the peripheral retina associated with axial elongation.
Lattice degeneration: Found in about 8% of the general population and about 30% of eyes with retinal detachment. 2) It contributes to 20–30% of all RRD cases. Symptomatic horseshoe tears progress to RRD in at least half of untreated cases, but laser photocoagulation reduces this to less than 5%. The natural progression rate of asymptomatic horseshoe tears to RRD is about 5%. 2)
Posterior vitreous detachment (PVD): Vitreous traction associated with acute PVD is the main mechanism for flap tear formation. It occurs as a physiological change in older adults. In about 88% of patients with vitreous hemorrhage, tears are found in the superior quadrant. 2)
History of cataract surgery: 20–40% of RRD cases have a history of cataract surgery. 2) The risk of postoperative RRD is about 0.21%, and it increases approximately 4-fold after posterior capsulotomy with Nd:YAG laser. 2)
Trauma: Accounts for about 10% of all RRD cases. 2) More common in young males and is a major cause of dialysis and giant retinal tears.
History in the fellow eye: Bilateral involvement occurs in about 10% of cases.
Conditions for laser photocoagulation: gradually increase power from 0.2 seconds, 150 mW, 200 μm to achieve a moderately white coagulation spot. For lattice degeneration, use a three-mirror or wide-angle inverted contact lens to surround the lesion with 2 to 3 rows of coagulation spots without gaps (coagulation size 400–500 μm).
QWill all people with myopia develop retinal detachment?
A
Myopia is the greatest risk factor for RRD, but the incidence rate is 0.01–0.015% of the population, and most people with myopia do not develop it. However, in high myopia (≥ -6 D), the complication rate of lattice degeneration is high, and it is reported that 0.3–0.5% of atrophic holes within lattice degeneration progress to RRD. Regular fundus examinations are particularly important.
Diagnosis involves fundus examination using an indirect ophthalmoscope, a slit-lamp biomicroscope with a pre-corneal lens or a three-mirror lens to identify the detached retina and causative retinal breaks. Slit-lamp examination also allows observation of the vitreous to assess the presence of posterior vitreous detachment and vitreous traction on the break. It is essential to determine whether the detachment extends to the macula, as this affects postoperative visual prognosis.
In outpatient examination, binocular indirect ophthalmoscopy with scleral depression is most useful. Differentiating true breaks from pseudo-holes, evaluating the presence of subretinal fluid around the break, and assessing the extent of detachment are critical for determining the treatment plan.
The following information from the patient history is important for diagnosis and treatment planning: 2)
OCT (Optical Coherence Tomography): Detects subtle macular detachment. Useful for differentiating from retinoschisis and confirming the presence of subretinal fluid. 2) Also used to predict postoperative visual acuity.
B-scan ultrasound: Essential when media opacities such as vitreous hemorrhage are present. Allows evaluation of detachment extent, morphology, and proliferative membranes. 2)
Retinoschisis: Separation between retinal layers. OCT shows a two-leaf structure of inner and outer layers. If there is no perforation in the outer layer, detachment does not occur.
Exudative retinal detachment: No tear. Characterized by positive shifting fluid that moves with position change. Identification of the cause (e.g., Vogt-Koyanagi-Harada disease, choroidal tumor) is important.
Tractional retinal detachment: Tent-shaped with poor mobility. Occurs in conditions such as proliferative diabetic retinopathy.
When the macula detaches, irreversible degeneration of photoreceptors begins. In macula-on RRD, 73% achieve corrected visual acuity of 0.5 or better at 2 months postoperatively. In macula-off RRD, about half of patients have visual acuity of 0.5 or less.
Preoperative positioning may suppress fluid flow into the macula:
Superior bullous detachment → Supine position (Trendelenburg position)
This is an external eye surgery in which a silicone buckle is sutured to the sclera on the outside of the eyeball, compressing and indenting the eye wall inward to close the retinal break.
Cryotherapy: Apply minimal coagulation to the edges of the tear and degenerative areas. Avoid excessive coagulation as it may promote PVR.
Selection and placement of buckle: Local buckle (for single tear) or encircling band (for multiple tears or PVR cases)
Buckle material
Shape
Main use
Silicone sponge
Localized buckling
Single/localized tear
Silicone band
Encircling band
Encircling buckle / 360° buckle
Silicone tire
Wide band
Large tears, lattice degeneration
Drainage of subretinal fluid (if needed): When there is high subretinal fluid accumulation, drainage is performed through a partial scleral incision. A non-drainage technique can also be selected, with lower complication risk.
Gas injection (if needed): Additional internal tamponade with SF₆ or C₃F₈.
Outcomes: Initial anatomical reattachment rate over 90%. In phakic eyes, visual outcomes may be superior to vitrectomy, and 5, 6) in macula-off retinal detachment, SB has been reported to show significantly better outcomes. 6)
Major complications: redetachment, PVR, SINS (buckle-induced infection, necrosis, exposure), 4) refractive change (myopic shift), ocular motility disorder/diplopia.
Method: After vitrectomy, the tear is sealed, and internal tamponade is performed with gas (20% SF₆, 14% C₃F₈) or silicone oil.
Outcomes: The primary anatomical success rate is comparable to scleral buckling. 2)Cataract acceleration is a disadvantage, and careful consideration is needed in young phakic patients.
Intraoperative macular protection in macula-on cases: Intraoperative macular protection is especially important in cases where the macula is not detached.
Prevention of intraoperative intraocular pressure fluctuations using valved cannulas
Avoidance of subretinal fluid inflow through a large open tear
If bullous detachment is present, first reduce SRF via drainage retinotomy
Place perfluorocarbon liquid (PFCL) in the posterior pole to prevent fluid migration under the fovea
Drain SRF sufficiently before complete fluid-air exchange (inadequate drainage may cause macular detachment)
Steamroller technique: A procedure to prevent iatrogenic macular detachment by rolling gas over the macula in bullous detachment near the macula. It is known as a unique intraoperative management method for macula-off RRD.
This is an outpatient procedure in which an expansile gas is injected into the vitreous cavity to close the retinal break using the buoyancy of the gas, followed by cryopexy or photocoagulation to create scarring around the break.
Indications:
RRD with breaks within the superior 120–180° (10 to 2 o’clock position)
Gas injection: inject through the pars plana on the temporal side (4 mm posterior to the limbus in phakic eyes)
Check intraocular pressure and blood flow: confirm central retinal artery perfusion. If pulsation is absent for several minutes, perform re-decompression
Positioning instruction: maintain gas position over the tear for 5–8 days
Results of the PIVOT trial (randomized comparison of PR and PPV):
This is a segmental scleral buckling procedure without drainage, and is reported to be applicable to approximately 90% of rhegmatogenous retinal detachments. Good outcomes have been reported: primary reattachment rate 91%, after reoperation 97.4%, and PVR incidence 0.9%.
In phakic eyes with simple RRD (especially in young patients), scleral buckling may result in better visual outcomes. 2, 5, 6)Vitrectomy is chosen for severe PVR or complex RRD with posterior pole breaks. The choice of surgical procedure is determined by a comprehensive assessment of the characteristics and location of the break, severity of PVR, patient background, and surgeon’s expertise.
The conditions for the development of rhegmatogenous retinal detachment are (1) a retinal break and (2) vitreous liquefaction.
Formation of flap tears: Vitreous traction due to posterior vitreous detachment concentrates on lattice degeneration or areas of strong vitreoretinal adhesion. The presence of lattice degeneration or strong vitreoretinal adhesion leads to break formation. It occurs most frequently in the superotemporal quadrant (60%).
Formation of atrophic holes: These form from retinal thinning and necrosis within lattice degeneration without vitreous traction. Common in young individuals, women, and high myopia. Since they occur before posterior vitreous detachment, the vitreous remains attached, and progression is often slow.
When retinal detachment occurs, photoreceptors and retinal pigment epithelial cells are separated, and oxygen and nutrient supply from the choroid is impaired. Early degeneration and loss of photoreceptor outer segments occur, gradually leading to irreversible degeneration.
The main factors for subretinal fluid extending to the macula are as follows.
Gravity: Fluid from superior tears tends to move toward the macula due to gravity. In inferior detachments, gravity delays macular involvement.
Inertial forces from eye movements: Saccades (rapid eye movements) apply traction to the tear edges, promoting fluid inflow. This is the theoretical basis for the effectiveness of preoperative rest.
Degree of vitreous liquefaction: In middle-aged and older individuals, completely liquefied vitreous tends to flow in easily, leading to rapid progression as bullous retinal detachment. In younger individuals, the vitreous is gel-like, so inflow is slow and often results in shallow detachment.
Mechanism of the non-drainage method (Lincoff-Kreissig method)
PVR is the most common complication after RRD surgery, defined as tractional retinal detachment due to formation of epiretinal and subretinal proliferative membranes.
Mechanism: retinal detachment → breakdown of blood-retinal barrier → RPE cells, glial cells, and macrophages enter the vitreous cavity → cytokine stimulation (e.g., TGF-β) → epithelial-mesenchymal transition and proliferation of cells → contractile membrane formation → re-detachment.
RPE cells transform into fibroblast-like cells, produce collagen, and form membranous or cord-like proliferative tissue. The old PVR severity classification (Retina Society 1983) is as follows.
Grade A: Vitreous opacity, pigment clumps in the vitreous, pigment clumps on the retina
Grade B: Formation of retinal surface folds, tortuosity of retinal vessels, elevation of the tear edge, reduced vitreous mobility
Arndt et al. (2023) reported in a study of 73 non-diabetic RRD and 64 ERD patients that intravitreal glucose concentration in RD eyes (2.28 mmol/L) was significantly higher than in ERM eyes (1.60 mmol/L) (p<0.0001). 1) Intravitreal glucose significantly correlated with macrophage density (p=0.002) and RD extent (r=0.38). It showed an inverse correlation with postoperative macular thickness (MFT) (r=-0.51), and a significant correlation was found between epithelial cell density and PVR-C grade (p=0.002). 1) It has also been hypothesized that collagen cross-linking by advanced glycation end products (AGEs) contributes to vitreous stiffening. 1)
7. Latest Research and Future Perspectives (Research-Stage Reports)
Data from Arndt et al. (2023) suggest that insulin may play a protective role for cones. 1) Based on the hypothesis that the high-glucose environment in RD eyes exacerbates photoreceptor damage, improving visual prognosis through metabolic intervention is a research topic.
German registry data show an increase in annual incidence from 15.6 to 24.8 per 100,000 population, with aging, increasing myopia prevalence, and rising cataract surgery numbers cited as background factors. 2) The risk of RRD after cataract surgery has decreased to 0.21% with improved surgical techniques. 2)
RD in young adults and adults with history of untreated ROP
Long-term observation of eyes with a history of untreated ROP found retinal tears in 18.4% of those aged ≤18 years and 35.1% of those aged 19–30 years. 3) The main mechanism is strong vitreoretinal adhesion before posterior vitreous detachment, and the reoperation rate in retinal detachment cases is as high as 36%. Optimizing surgical strategies according to the underlying disease in children and young adults is a challenge. 3)
This technique combines a wide-angle observation system with chandelier lighting to compensate for the limited visibility of conventional procedures. 7) Meta-analyses show that visual acuity and anatomical success rates are comparable to conventional methods, with reduced surgical time. 9)
Postoperative photoreceptor realignment may affect functional outcomes and is being studied as a factor explaining differences in postoperative visual function between scleral buckling and vitrectomy. 6)
Al-Saleh et al. (2025) performed pneumatic retinopexy using SF₆ gas for traumatic macula-sparing RRD, achieving reattachment within 24 hours and a final visual acuity of 20/40. 14) This suggests that with appropriate case selection, this procedure may be effective for traumatic RRD.
Dean et al. (2023) reported a case of worsening inflammation, keratic precipitates, and vitreous opacity occurring 2–3 weeks after vitrectomy combined with scleral buckling. 15) The condition improved with increased steroids and systemic NSAIDs, indicating that HLA-B27 testing is useful in the differential diagnosis of postoperative persistent inflammation.
Simultaneous surgery for idiopathic macular hole and macula-on RRD
Au Eong et al. (2024) reported a case of concurrent idiopathic macular hole persisting for 30 years (documented by photographs) and acute macula-on RRD, in which PPV combined with ILM peeling and C₃F₈ tamponade achieved simultaneous reattachment and hole closure. 16) Although visual improvement was limited (remained at 6/45) due to long-term photoreceptor damage, this report is notable for demonstrating the feasibility of simultaneous surgery.
Arndt C, Hubault B, Hayate F, et al. Increased intravitreal glucose in rhegmatogenous retinal detachment. Eye (Lond). 2023;37(4):638-643. doi:10.1038/s41433-022-01968-w.
Kim SJ, Bailey ST, Kovach JL, Lim JI, Vemulakonda GA, Ying GS, et al. Posterior Vitreous Detachment, Retinal Breaks, and Lattice Degeneration Preferred Practice Pattern®. Ophthalmology. 2025;132(4):P163-P196. doi:10.1016/j.ophtha.2024.12.023. PMID:39918519.
Hamad AE, Moinuddin O, Blair MP, et al. Late-Onset Retinal Findings and Complications in Untreated Retinopathy of Prematurity. Ophthalmol Retina. 2020;4(6):602-612. doi:10.1016/j.oret.2019.12.015.
Bannu Jayallan, Mohd Hasif Mustafa, Norshamsiah Md Din, Mae-Lynn Catherine Bastion. Rhegmatogenous Retinal Detachment in Anterior Scleritis With Ulcerative Colitis. Cureus. 2024. doi:10.7759/cureus.61819.
Ferro Desideri L, Bonfiglio V, Russo A, et al. Scleral buckling: a review of clinical aspects and current concepts. J Clin Med. 2022;11(2):314.
Cruz-Pimentel M, Huang CY, Wu L.. Scleral Buckling: A Look at the Past, Present and Future in View of Recent Findings on the Importance of Photoreceptor Re-Alignment Following Retinal Re-Attachment. Clin Ophthalmol. 2022;16:1971-1984. doi:10.2147/opth.s359309. PMID:35733617; PMCID:PMC9208732.
Governatori L, Scampoli A, Culiersi C, Bernardinelli P, Picardi SM, Sarati F, Caporossi T. Chandelier-Assisted Scleral Buckling: A Literature Review. Vision (Basel, Switzerland). 2023;7(3). doi:10.3390/vision7030047. PMID:37489326; PMCID:PMC10366817.
Bernardi E, Shah N, Ferro Desideri L, Potic J, Roth J, Anguita R. Cystoid Macular Edema Following Rhegmatogenous Retinal Detachment Repair Surgery: Incidence, Pathogenesis, Risk Factors and Treatment. Clinical ophthalmology (Auckland, N.Z.). 2025;19:629-639. doi:10.2147/OPTH.S489859. PMID:40007877; PMCID:PMC11853832.
Ziafati M, Mirshahi R, Sanadgol N, Mahmoudinezhad G, Chaibakhsh S. Functional Outcome of Chandelier-Assisted Scleral Buckling in Rhegmatogenous Retinal Detachment: A Systematic Review and Meta-Analysis. Journal of current ophthalmology. 2025;37(2):172-182. doi:10.4103/joco.joco_39_25. PMID:41488718; PMCID:PMC12758858.
Wang JC, Tang WM, Eliott D. Management of Large Subretinal Gas Bubble After Pneumatic Retinopexy With Head-Positioning Maneuver. Journal of vitreoretinal diseases. 2022;6(2):167-170. doi:10.1177/24741264211009666. PMID:37008670; PMCID:PMC9976003.
Ahmed I, Wu DM. Drusen Disappearance After Retinal Detachment Repair. J VitreoRetin Dis. 2025;9(1):109-112. doi:10.1177/24741264241276603.
Flaxel CJ, Adelman RA, Bailey ST, Fawzi A, Lim JI, Vemulakonda GA, et al. Idiopathic Epiretinal Membrane and Vitreomacular Traction Preferred Practice Pattern®. Ophthalmology. 2020;127(2):P145-P183. doi:10.1016/j.ophtha.2019.09.022. PMID:31757497.
Al-Saleh A, Al-Otabi A, Al-Shammari Y, Alrabiah M. Successful Management of Macula-Sparing Retinal Detachment Following Blunt Ocular Trauma Using Pneumatic Retinopexy. Cureus. 2025;17(6):e85709. doi:10.7759/cureus.85709. PMID:40495823; PMCID:PMC12151135.
Dean J, McTavish S, Feng Y, et al. Persistent inflammation associated with HLA-B27 after pars plana vitrectomy with scleral buckle placement. J VitreoRetinal Dis. 2023;7(6):557-561. doi:10.1177/24741264231176143. PMID:37974913; PMCID:PMC10649459.
Au Eong JTW, Lim JHM, George SM, Au Eong KG. Successful anatomical closure of a photographically documented 30-year-old idiopathic full-thickness macular hole following surgery for concurrent repair of an acute macula-on rhematogenous retinal detachment. Journal of surgical case reports. 2024;2024(4):rjae231. doi:10.1093/jscr/rjae231. PMID:38633563; PMCID:PMC11021346.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.