Giant Retinal Tear (GRT) is a rhegmatogenous retinal detachment (RRD) associated with a full-thickness retinal tear extending 90 degrees (3 clock hours) or more. The tear usually occurs at the posterior border of the vitreous base posterior to the ora serrata. When the tear exceeds two quadrants (180 degrees), the posterior retinal flap tends to invert and fold over the optic disc or macula.
GRT accounts for approximately 1.5% of all rhegmatogenous retinal detachments 1), with a male predominance (72%). 1) Associated conditions include Marfan syndrome and Stickler syndrome1), and it also occurs frequently in highly myopic eyes with lattice degeneration.
By etiology, 60–80% are idiopathic, and traumatic cases account for 16.1%. 4) Bilateral involvement occurs in up to 20%, and the incidence of RD in the fellow eye reaches 30–35%. 3)
Equatorial Type
Most common GRT type: Tear located at the equator.
Posterior flap mobility: Moderate. Unfolding is relatively easy.
Posterior Equatorial Extension Type
Flap inversion is common: The tear edge extends posteriorly.
Folding risk: Inversion over the macula or optic disc is likely.
Pars Plana Type
Rarest type: Tear located near the pars plana.
Anterior approach: Surgical technique may be specialized in some cases.
QWhat is the difference between GRT and GRD (giant retinal dialysis)?
A
GRT (Giant Retinal Tear) is a full-thickness retinal tear occurring at the posterior border of the vitreous base, caused by vitreous traction. In contrast, GRD (Giant Retinal Dialysis) is a condition where the retina is detached at the ora serrata itself, often traumatic, and differs in that vitreous remains attached posterior to the tear margin. Distinguishing them is important because treatment approaches also differ.
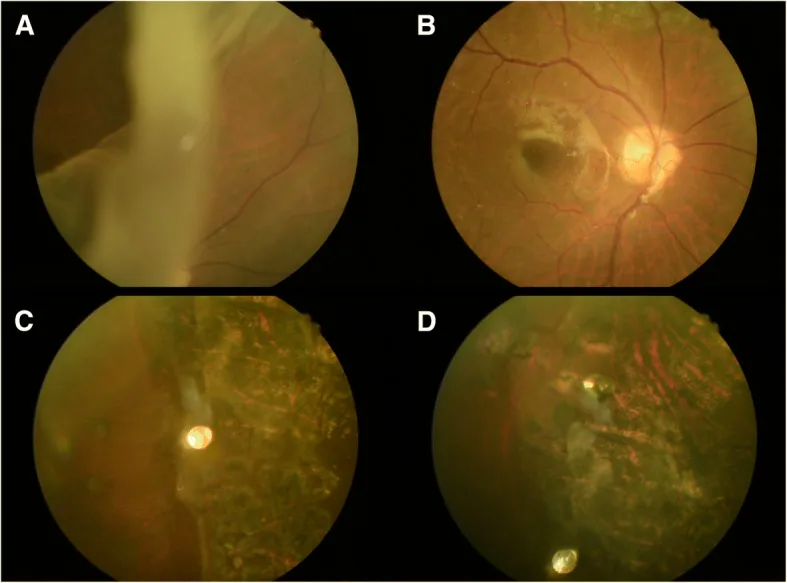
Yo-Chen Chang; Li-Yi Chiu; Tzu-En Kao; Wen-Hsin Cheng; Ting-An Chen; Wen-Chuan Wu. Management of Giant Retinal Tear with microincision vitrectomy and metallic retinal tacks fixation-a case report. BMC Ophthalmol. 2018 Oct 22; 18:272. Figure 1. PMCID: PMC6198422. License: CC BY.
a. Fundus examination revealed a 120 degree giant tear with large inverted flap of the 53-year-old man’s right eye. b, c and d. No recurrent retinal detachment was noted during follow up period and the retina was well fixated by retinal tacks and laser scar
Tobacco dusting (Shafer sign): Present in all cases. Pigment particles scattered in the anterior vitreous, strong evidence of retinal tear.
Inversion of the posterior flap: In giant retinal tears, the posterior retinal flap folds over the optic disc or macula, exposing the retinal pigment epithelium (RPE).
Characteristics of pediatric GRT: Posterior vitreous detachment (PVD) is absent, and the vitreous gel is more viscous, presenting findings different from those in adults. 2)
Abuse-related GRT: A case has been reported in a 4-week-old neonate with two GRTs (1–5 o’clock and 7–11 o’clock). 4)
Tear extent >150 degrees: A GRT extent exceeding 150 degrees is a poor prognostic factor. 1)
High myopia: Often associated with lattice degeneration, making the posterior border of the vitreous base fragile.
Young age (≤35 years): Higher risk of surgical failure. 1)
Male sex: Approximately 1.3 times higher risk than females; 72% of cases are male. 1)
Stickler syndrome: A hereditary disorder with abnormal collagen synthesis, associated with a high lifetime risk of bilateral GRT and RRD. 3)
Trauma (blunt trauma): Shearing forces from blunt trauma can tear the posterior border of the vitreous base. 4)
Child abuse: Multiple GRT cases have been reported in a 4-week-old infant. 4)
QIf a GRT occurs in one eye, is the other eye also likely to develop it?
A
The incidence of RD in the fellow eye is as high as 30–35%. 3) However, meta-analyses have shown that prophylactic laser or cryotherapy can reduce the risk of RD by up to 86%. 3) In Stickler syndrome, 360-degree prophylactic laser is particularly recommended. For details, see the section “Latest Research and Future Prospects”.
B-scan ultrasonography: A double linear echo sign (the folded retina appears as a double line) is characteristic of GRT. Useful when fundus view is poor due to opaque vitreous.
Differential diagnosis (GRT vs. GRD): GRT is a posterior tear due to vitreous traction, while GRD is a traumatic dialysis of the ora serrata; the approaches differ.
Fundus examination of the fellow eye: Essential to check for lattice degeneration, peripheral tears, and predisposing factors.
Pediatric and infant cases: Actively investigate for history of trauma or possible child abuse. 4)
QHow is pediatric GRT different from adult GRT?
A
In children, the proportion of traumatic GRT is higher (up to 32%) compared to adults, and because posterior vitreous detachment (PVD) is absent, separation of the vitreous from the retina is difficult. 2) The presence of viscous vitreous gel makes vitrectomy surgery more complex than in adults. In infants, the possibility of injury from abuse should be considered. 4)
Pars plana vitrectomy is the first-line treatment for GRT. 1)Vitrectomy was chosen in 34 of 36 studies 1), and MIVS (microincision vitrectomy surgery; 23G to 27G) is now widely used as the standard technique. 1)
Key intraoperative points are as follows:
Introduction of perfluorocarbon liquid (PFCL): A heavy liquid used to press the inverted retinal flap from behind, unfold and stabilize it. This is a fundamental step in GRT surgery.
Endophotocoagulation: Apply 8 to 10 rows of photocoagulation along the edge of the retinal tear to seal the retina around the tear.
PFCL-tamponade exchange: Replace PFCL with silicone oil or gas tamponade to complete the surgery (direct PFCL-oil exchange technique may also be used).
Indications for lensectomy: Some cases require lensectomy to ensure anterior visualization or facilitate intraoperative maneuvers.
It has been reported that 77% of postoperative proliferative vitreoretinopathy occurs within one month after surgery1), making early follow-up particularly important.
QHow often does redetachment occur after GRT surgery?
A
Redetachment due to proliferative vitreoretinopathy has been reported to occur in up to 45% of cases. 77% of postoperative proliferative vitreoretinopathy occurs within one month after surgery.1) The anatomical success rate of primary surgery (SSAS) is 80–90% in most studies, but since PVR is the greatest cause of failure, strict follow-up during the first postoperative month is essential.
Tear formation at the posterior border of the vitreous base: Local traction penetrates the full thickness of the retina, forming a large tear of 90 degrees or more.
Release of RPE cells: The tear exposes the RPE to the vitreous cavity, releasing cells. This initiates proliferative vitreoretinopathy.
Progression of proliferative vitreoretinopathy: Released RPE cells and glial cells proliferate and contract, forming proliferative membranes on the retinal surface. This is the main cause of redetachment.
Mechanism of traumatic GRT: Rapid deformation of the eyeball due to blunt trauma generates shear forces, tearing the retina at the posterior border of the vitreous base. 4)
Sherief ST et al. (2022) reported a case of multiple GRTs (at 1–5 o’clock and 7–11 o’clock) in a 4-week-old neonate. It is presumed that rapid mechanical shear forces from trauma (abuse) caused extensive tears in the thin retina of the infant. 4)
7. Latest Research and Future Perspectives (Investigational Reports)
The effectiveness of prophylactic laser and cryocoagulation in the fellow eye of patients with unilateral GRT has been quantified for the first time in a systematic review and meta-analysis.
Vasilakopoulou MP et al. (2025) showed that prophylactic treatment of the fellow eye reduces the risk of RD by 86% (OR 0.14; 95% CI 0.05–0.40). 3) For laser alone, OR was 0.12; for laser plus cryocoagulation, OR was 0.17; the difference between the two modalities was not statistically significant (p=0.57).
In patients with Stickler syndrome, 360-degree prophylactic laser is particularly recommended. 3) However, an important limitation of this meta-analysis is that no RCTs (randomized controlled trials) were available, and the results are based solely on observational studies. 3)
Quiroz-Reyes et al. (2024) conducted a scoping review of 36 studies involving 751 eyes and reported a vitrectomy technique usage rate of 89%, SSAS of 91.2%, and FAS of 96.7%. 1) The possibility of reducing postoperative epiretinal membrane (ERM) by ILM peeling was also suggested, but the lack of RCTs was pointed out as the major limitation. 1)
Reports on surgical approaches for pediatric GRT are also increasing, and modifications of vitrectomy for pediatric eyes lacking posterior vitreous detachment are being discussed. 2) In the future, prospective multicenter studies and RCTs are needed to build evidence.
Quiroz-Reyes MA, Babar ZU, Hussain R, Loh ZC, Quiroz-Gonzalez EA, Quiroz-Gonzalez MA, et al. Management, risk factors and treatment outcomes of rhegmatogenous retinal detachment associated with giant retinal tears: scoping review. International journal of retina and vitreous. 2024;10(1):35. doi:10.1186/s40942-024-00552-6. PMID:38654369; PMCID:PMC11036595.
Bhende PS, Kashyap H, Nadig RR. Surgical management of a case of giant retinal tear with closed funnel retinal detachment in a pediatric patient. Indian J Ophthalmol. 2024. doi:10.4103/IJO.IJO_1598_23.
Vasilakopoulou MP, Androudi S, Tsinopoulos I, Stavrakas P.. Prophylactic Laser and Cryotherapy in the Fellow Eye of Patients With Giant Retinal Tears: A Systematic Review and Meta-Analysis. Cureus. 2025;17(12):e99849. doi:10.7759/cureus.99849. PMID:41445997; PMCID:PMC12723434.
Sherief ST, Dhoot AS, Schwartz S, VandenHoven C, Lam WC, Mireskandari K. Multiple giant retinal tears due to inflicted injury in a neonate. American journal of ophthalmology case reports. 2022;26:101453. doi:10.1016/j.ajoc.2022.101453. PMID:35257035; PMCID:PMC8897640.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.