Exudative retinal detachment (ERD) is a type of non-rhegmatogenous retinal detachment. Retinal detachment without a tear is called non-rhegmatogenous retinal detachment, which is broadly divided into exudative and tractional types. Exudative retinal detachment is a condition in which fluid accumulates in the subretinal space without a retinal tear or traction, and occurs in various diseases such as inflammatory diseases, degenerative diseases, infections, and tumors.
The basic pathology is the accumulation of exudate under the retina due to dysfunction of retinal vessels, retinal pigment epithelium (RPE), or choroid. Disruption of the blood-retinal barrier (BRB) leads to leakage of fluid from choroidal vessels, retinal vessels, and RPE, which accumulates under the retina. It is sometimes used almost synonymously with “serous retinal detachment,” but this article covers exudative retinal detachment in a broad sense, including neoplastic, inflammatory, and drug-induced types.
Causes are diverse, including uveitis such as Vogt-Koyanagi-Harada disease (VKH) and posterior scleritis, retinal pigment epithelial diseases such as CSC and multiple posterior pigment epitheliopathy (MPPE), subretinal neovascularization such as age-related macular degeneration, vascular diseases such as Coats disease, neoplastic diseases such as choroidal hemangioma and retinoblastoma, uveal effusion, and diabetic macular edema. Since treatment fundamentally differs depending on the disease, accurate diagnosis is very important.
QHow is rhegmatogenous retinal detachment different from exudative retinal detachment?
A
Rhegmatogenous retinal detachment occurs when a hole (tear) forms in the retina, allowing vitreous fluid to enter. Exudative retinal detachment has no tear and results from fluid accumulation under the retina due to vascular or RPE damage. The former is treated by surgical closure of the tear, while the latter focuses on treating the underlying cause. “Shifting fluid,” where the detachment moves with position changes, is characteristic of exudative detachment.
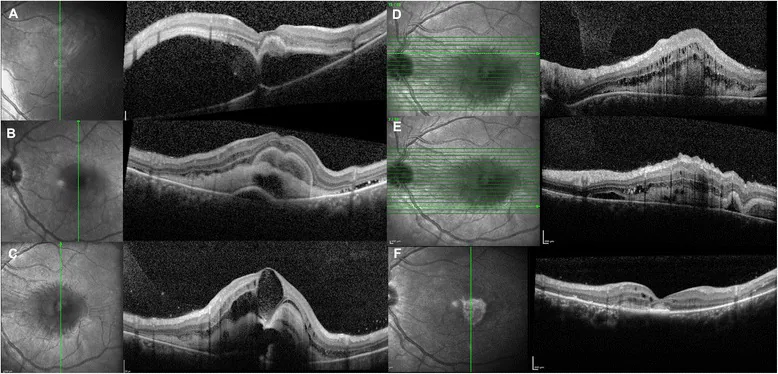
Maggio E, et al. Multimodal imaging findings in a case of severe Central Serous Chorioretinopathy in an uncomplicated pregnancy. BMC Ophthalmol. 2015. Figure 1. PMCID: PMC4688919. License: CC BY.
Optical coherence tomography (OCT) shows marked serous elevation of the neurosensory retina in the macula with subretinal hyperreflective material (a), and resolution of subretinal fluid with accumulation of subretinal exudates during follow-up (b-c). This corresponds to serous retinal detachment discussed in the section “2. Main symptoms and clinical findings”.
Typical exudative retinal detachment shows a dome-shaped elevation of the retina with a smooth surface, and subretinal fluid shifts with positional changes (shifting fluid). Folds or irregular elevations as seen in rhegmatogenous detachment usually do not occur.
Inflammatory (VKH)
Bilateral serous detachment: Multiple dome-shaped elevations occur in both eyes.
Choroidal thickening: Marked choroidal thickening (approximately 600 μm) is seen on OCT. 2)
Characteristic OCT findings: Vesicular retinal detachment with septal structures, narrowing of choroidal luminal structures.
Optic dischyperemia and edema: Inflammatory changes also involve the optic nerve head.
Drug-induced (MEKAR)
Acute-onset bilateral SRD: Develops rapidly after MEK inhibitor administration. 4)
Symptoms are often mild: Some cases have mild vision loss with few subjective symptoms.
Reversible: Often resolves within 3 days after drug discontinuation. 4)
Pregnancy-related
Bilateral serous RD: May be associated with preeclampsia/HELLP syndrome. 6)
Macula-dominant detachment: Fluid accumulates in the macula, causing metamorphopsia and vision loss.
Resolution after delivery: Often resolves spontaneously after delivery, with vision recovery. 6)
Traumatic/Iatrogenic
ERD after RPE tear: Exudative detachment occurs secondary to a traumatic RPE tear. 1)
Drug-induced (MEKAR): RPE dysfunction via the MAPK pathway caused by MEK inhibitors (e.g., binimetinib). Incidence reported as 0.6–27% in melanoma treatment and 0.9% in colorectal cancer treatment. 4)
Tilted disc syndrome (TDS): Local circulatory disturbance due to scleral thickening and choroidal thinning leads to macular serous detachment. 3)
Traumatic RPE tear: RPE tear after trauma such as contusion may lead to secondary exudative detachment. 1)
Iatrogenic (after ROP laser): Exudative detachment may occur after laser photocoagulation for retinopathy of prematurity. Gestational age >40 weeks and low birth weight are reported as risk factors. 5)
Neoplastic: Choroidal malignant melanoma and metastatic choroidal tumors can cause ERD.
Coats disease: A vascular disease generally affecting male children, not associated with heredity or systemic disease. Adult onset also occurs. Fundus examination reveals tortuous abnormal vascular networks in the periphery, and fluorescein angiography shows profuse leakage from these areas. It presents with yellowish subretinal exudates and exudative retinal detachment. In children, differentiation from retinoblastoma is essential; distinguish from retinoblastoma which shows a solid mass on ultrasound and calcification on head CT.
Uveal effusion: Characterized by highly mobile serous retinal detachment that easily shifts with head position and peripheral choroidal detachment. Often associated with microphthalmia, high hyperopia, vortex vein abnormalities, and scleral thickening. Scleral decompression surgery is a treatment option.
Immune checkpoint inhibitor (ICI)-associated ERD: VKH-like inflammatory uveitis and serous retinal detachment have been reported in patients using ICIs such as PD-1/PD-L1 inhibitors and CTLA-4 inhibitors. 12) Whether to continue ICI requires consultation with oncology.
QCan anticancer drugs cause retinal detachment?
A
Some antitumor drugs, including MEK inhibitors (e.g., binimetinib), can impair RPE function via the MAPK pathway and cause exudative retinal detachment (MEKAR). 4) Most cases are asymptomatic to mild and resolve within days after drug discontinuation. Whether to continue treatment should be discussed with the attending physician.
A multimodal approach combining multiple modalities is important for identifying the underlying disease and assessing the condition. In ophthalmoscopy, carefully observe not only the location and extent of retinal detachment but also accompanying findings such as retinal hemorrhage, exudates, pigment epithelial detachment, subretinal neovascularization, and the presence of elevated lesions. Also examine the entire eye for inflammatory findings in the anterior segment and intermediate media. Systemic examinations are also important, such as cerebrospinal fluid examination and hearing test for VKH, and imaging for neoplastic diseases.
Evaluation of choroidal circulatory insufficiency and hypoperfusion areas
Ultrasonography
Differentiation of posterior scleritis and choroidal tumors
OCT (Optical Coherence Tomography): Noninvasively evaluates the presence, amount, and distribution of subretinal fluid. Measurement of choroidal thickness is also useful for assessing activity in VKH. In the acute phase of VKH, OCT shows marked choroidal thickening of approximately 600 μm. 2)
Fluorescein angiography (FA): In VKH, multiple punctate hyperfluorescent spots and leakage from the optic disc are characteristic findings. 2) In CSC, leakage points are seen on FA, and in IA, increased permeability of choroidal vessels is observed. In CSC, differentiation from idiopathic CNV and optic disc pit in young patients, and from polypoidal choroidal vasculopathy (PCV) and pachychoroid neovasculopathy in elderly patients is important; IA and OCTA are used to check for polypoidal lesions and CNV. 9)
ICGA (Indocyanine Green Angiography): In VKH, multiple hypoperfusion areas are visualized. 2) It is excellent for evaluating choroidal circulatory disorders.
Ultrasonography (B-mode): In posterior scleritis, scleral thickening and T-sign (Tenon’s capsule fluid accumulation) can be confirmed. It is also important for differentiation from neoplastic lesions. In pediatric Coats disease, differentiation from retinoblastoma is essential; ultrasonography shows a solid mass, and head CT shows calcification, distinguishing it from retinoblastoma.
QCan OCT alone make a diagnosis?
A
OCT is essential for detecting and monitoring subretinal fluid, but multimodal imaging combining FA, ICGA, and ultrasound is often necessary to identify the underlying cause. 2) For example, in VKH, multiple hypofluorescent areas on ICGA, together with FA findings, provide diagnostic evidence.
QHow do you differentiate Coats disease from retinoblastoma?
A
Coats disease is characterized by yellowish subretinal exudates and peripheral abnormal vascular networks, with intense fluorescein leakage on fluorescein angiography. Retinoblastoma typically shows a solid mass on ultrasound and characteristic calcifications on head CT. This distinction is especially important in children with leukocoria, as the treatment strategies for these two diseases are fundamentally different, making accurate differentiation essential.
The basis of treatment is identifying and treating the underlying cause. Direct drainage of subretinal fluid is usually unnecessary; once the cause is resolved, the fluid often resolves spontaneously.
For VKH, a combination of sub-Tenon triamcinolone injection (20 mg), oral prednisolone (1 mg/kg/day), and an immunosuppressant (methotrexate; MTX) has been reported to resolve serous retinal detachment within two weeks. 2)
Peng et al. (2025) reported a case of unilateral choroidal detachment associated with VKH, in which sub-Tenon TA 20 mg plus prednisolone 1 mg/kg/day and MTX led to resolution of subretinal fluid and choroidal detachment within two weeks. 2)
Discontinuation of the causative drug is the first-line treatment. Rapid resolution within three days of discontinuation has been reported, and in most cases no specific ophthalmic treatment is required. 4)
Sakumura et al. (2022) reported a case of bilateral serous retinal detachment due to binimetinib (a MEK inhibitor). OCT showed multiple subretinal fluid pockets in both eyes, but complete resolution occurred three days after binimetinib discontinuation. 4)
Blood pressure management and delivery are the most important therapeutic interventions. After delivery, serous detachment resolves spontaneously, and vision usually recovers. 6)
Phang et al. (2022) reported a case of a pregnant woman with preeclampsia complicated by HELLP syndrome who developed bilateral serous retinal detachment. After emergency cesarean section and antihypertensive therapy, the subretinal fluid resolved and vision returned to pre-onset levels. 6)
Subthreshold micropulse laser is considered effective.
Minowa et al. (2021) reported that subthreshold laser treatment was performed on 5 eyes with serous retinal detachment associated with tilted disc syndrome, and subretinal fluid disappeared in 4 of 5 eyes (80%). 3)
For exudative retinal detachment secondary to traumatic RPE tear, conservative treatment (e.g., prednisolone eye drops) is administered.
Panigrahi et al. (2023) reported a case of RPE tear and exudative retinal detachment after trauma. Spontaneous resolution occurred 2 weeks after prednisolone eye drop administration, and visual acuity recovered. OCT one week later showed depigmented cells filling the RPE tear site. 1)
Zou et al. (2022) reported a case of exudative retinal detachment in one eye after laser treatment for retinopathy of prematurity. Subretinal fluid resolved after 8 weeks with increased prednisolone eye drops (4 times/day to 8 times/day). 5)
The main pathology is an autoimmune reaction in which CD4-positive T cells target melanocytes (melanin-producing cells of the RPE and uvea). A strong genetic association with HLA-DRB1*0405 is known, and VKH is more common in East Asia. 2) Inflammation disrupts the tight junctions of the RPE (oBRB breakdown), allowing serous fluid from the choroid to flow into the subretinal space. OCT characteristically shows multiple bullous retinal detachments with septal structures and marked choroidal thickening in the acute phase. 2)
MEK inhibitors suppress the MAPK pathway, altering aquaporin expression density in the RPE and impairing RPE fluid transport function (oBRB breakdown). 4) This mechanism is reversible, and function recovers quickly after drug discontinuation.
In preeclampsia, placental factors (such as anti-VEGF antibody-like substances) cause systemic vasospasm. Choroidal arterial spasm leads to choroidal ischemia, impairing RPE pump function and causing oBRB breakdown. 6)
Scleral thickening and choroidal thinning lead to localized choroidal circulatory abnormalities. This abnormal circulation is thought to reduce RPE fluid transport capacity, causing chronic serous detachment. 3)
Physical trauma such as contusion causes RPE rupture, acutely disrupting the local oBRB. Within one week after RPE tear, depigmented cells begin to fill and repair the tear, sometimes leading to spontaneous resolution. 1)
QWhat is the structure of the blood-retinal barrier (BRB)?
A
The BRB is a barrier mechanism that controls substance exchange between the blood and retinal tissue. It has a two-layer structure: the inner BRB (iBRB) formed by tight junctions of retinal vascular endothelial cells, and the outer BRB (oBRB) formed by tight junctions of the RPE. Breakdown of the oBRB is a common pathology in many exudative retinal detachments.
7. Latest Research and Future Perspectives (Investigational Stages)
For chronic serous retinal detachment associated with tilted disc syndrome (TDS), the efficacy of subthreshold laser has been reported at the case level. 3) It is suggested that it may promote fluid absorption without leaving photocoagulation scars and while preserving RPE function, but verification through controlled trials is still insufficient.
Regarding the correlation between ocular adverse events of MEK inhibitors (MEKAR) and antitumor effects, sufficient data do not exist at present. 4) How to balance drug continuation and preservation of visual function is an important future research topic.
Pathophysiological Elucidation by Multimodal Imaging
The combination of OCT angiography (OCTA) and ICGA allows more detailed evaluation of blood flow changes in the choriocapillaris. 2) This is expected to improve the understanding of the pathophysiology of diseases causing exudative retinal detachment and the accuracy of treatment effect assessment.
Pachychoroid Spectrum Disease and Reclassification of CSC
In recent years, CSC has been reclassified as a type of pachychoroid spectrum disease characterized by choroidal thickening and pachyvessels (dilated large choroidal vessels). 9) The concept of pachychoroid is also important for understanding related diseases such as polypoidal choroidal vasculopathy (PCV) and pachychoroid neovasculopathy (PNV), and is influencing the diagnostic and differential classification system of exudative retinal detachment.
With the expansion of indications for immune checkpoint inhibitors (ICIs), ocular adverse events including VKH-like inflammatory uveitis and serous retinal detachment are increasing. 12) Appropriate management through collaboration between ophthalmologists and oncologists has become an important issue.
For steroid-resistant or steroid-dependent VKH, the use of TNF-α inhibitors such as infliximab and adalimumab, as well as biologics like rituximab, has been reported. 8) Although not yet established as a standard treatment, research continues on these as options for refractory cases.
Panigrahi PK, et al. Spontaneous resolution of posttraumatic RPE tear and associated exudative retinal detachment. J Curr Ophthalmol. 2023;35:408-410.
Chuzhi Peng, Yonghong Jiao, Chunli Chen. Unilateral choroidal detachment in an elderly patient with Vogt-Koyanagi-Harada disease: a case report and literature review. Front. Immunol. 2025;16. doi:10.3389/fimmu.2025.1514306.
Minowa Y, Ohkoshi K, Ozawa Y. Subthreshold Laser Treatment for Serous Retinal Detachment Associated with Tilted Disc Syndrome. Case reports in ophthalmology. 2021;12(3):978-986. doi:10.1159/000520570. PMID:35111034; PMCID:PMC8787533.
Sakumura M, et al. Bilateral serous retinal detachment with MEK inhibitor (binimetinib). Intern Med. 2022;61:1707-1712.
Phang DSK, Ariffin N, Abd Aziz H, Vendargon FM, Sonny Teo KS. Bilateral Serous Retinal Detachment in Pregnancy. Cureus. 2022;14(10):e30019. doi:10.7759/cureus.30019. PMID:36348857; PMCID:PMC9637277.
Tayal A, Bansal S. Vogt-Koyanagi-Harada disease: a narrative review. Ther Adv Ophthalmol. 2024;16:25158414241244681.
Cheung CMG, Lee WK, Koizumi H, et al. Pachychoroid disease. Eye (Lond). 2019;33(1):14-33. doi:10.1038/s41433-018-0158-4.
Daruich A, Matet A, Moulin A, Kowalczuk L, Nicolas M, Sellam A, et al. Mechanisms of macular edema: Beyond the surface. Progress in retinal and eye research. 2018;63:20-68. doi:10.1016/j.preteyeres.2017.10.006. PMID:29126927.
Campbell M, Humphries P. The blood-retina barrier: tight junctions and barrier modulation. Advances in experimental medicine and biology. 2012;763:70-84. PMID:23397619.
Dalvin LA, Shields CL, Orloff M, Sato T, Shields JA. CHECKPOINT INHIBITOR IMMUNE THERAPY: Systemic Indications and Ophthalmic Side Effects. Retina (Philadelphia, Pa.). 2018;38(6):1063-1078. doi:10.1097/IAE.0000000000002181. PMID:29689030.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.