Leukocoria means “white pupil” and is derived from the Greek words leukos (white) and kore (pupil). It refers to a condition in which a white light reflection is observed instead of the normal red reflex when illuminating the fundus through the pupil.
When there is opacity or an abnormal structure anywhere along the optical path from the cornea to the posterior pole, the red reflex from the choroidal vessels is blocked, resulting in a white pupillary reflex. The causative diseases include tumors, congenital anomalies, vascular diseases, inflammatory diseases, and opacities of the ocular media.
The most important disease to differentiate in leukocoria is retinoblastoma. Retinoblastoma is the most common intraocular malignant tumor in children, with an estimated incidence of 1 in 17,000 live births 2). Leukocoria and strabismus are the main initial signs 2), and early detection is directly linked to life prognosis and visual prognosis.
QWhat is the most important disease to rule out in leukocoria?
A
Retinoblastoma. It is the most common intraocular malignant tumor in children and is directly linked to life prognosis, so when leukocoria is observed, it must be ruled out as a top priority. For details, see the section “Diagnosis and Examination Methods”.
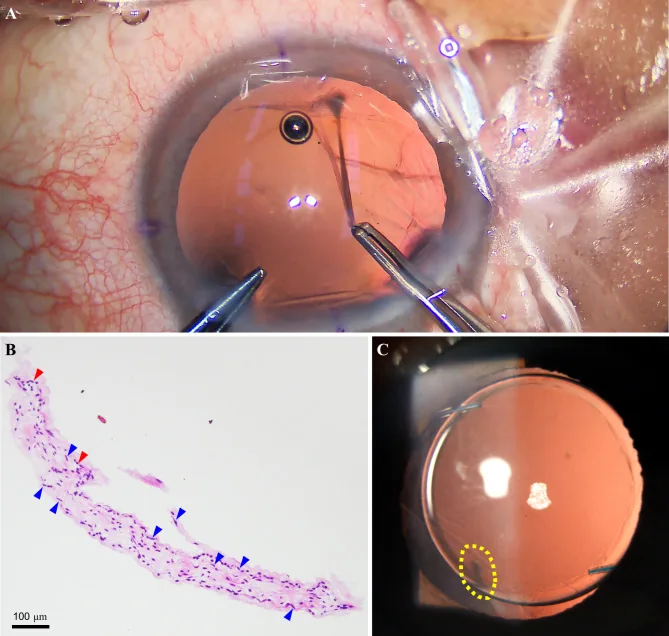
Yu Y, et al. Non-typical persistent hyperplastic primary vitreous: a rare case report and review of the literature. BMC Ophthalmol. 2023. Figure 2. PMCID: PMC10262480. License: CC BY.
Intraoperative and postoperative findings of the left eye: A is a fibrovascular cord-like band attached around the posterior lens capsule, B is a histological image including fibrous cells (yellow arrow) and capillaries (red arrow), and C is the normal anterior segment after surgery. This corresponds to the fibrovascular cord discussed in the section “2. Main Symptoms and Clinical Findings.”
The normal red reflex is replaced by a white or gray-white reflex. Asymmetry of the reflex between the two eyes (positive Bruckner reflex) is also an important finding.
Findings specific to the underlying disease are observed.
Retinoblastoma: Vascularized white elevated lesion. May contain calcification. Vitreous seeding may be present.
Coats disease: Retinal telangiectasia (light bulb telangiectasias). Commonly occurs in the inferior and temporal quadrants, with yellow lipid exudation 6)
QShould I see a doctor if only one eye appears white in flash photography?
A
Asymmetry of the red reflex is an indication for an eye examination. The American Academy of Pediatrics (AAP) recommends red reflex testing for all newborns, infants, and children. A white reflex or asymmetry of the reflex requires prompt referral to an ophthalmologist.
Retinoblastoma: When there is a germline mutation in the RB1 gene, it develops as an autosomal dominant trait. Hereditary types account for 35–45% of all cases, but only about 10% have a family history; most are de novo mutations 4).
Coats disease: Non-hereditary and sporadic; more than 75% are unilateral 6).
ROP: Low birth weight, low gestational age, and oxygen administration are major risk factors 4).
According to the 2008 American Academy of Pediatrics (AAP) recommendation, all newborns, infants, and children should undergo red reflex testing before discharge and during routine checkups.
Technique: Set the direct ophthalmoscope lens power to “0”, and in a dark room, shine light into both eyes simultaneously from about 45 cm away.
Normal finding: Symmetrical red reflex is obtained from both eyes.
Abnormal findings: Dark spots within the red reflex, marked reduction of the reflex, white reflex, or asymmetry of the reflex (Bruckner reflex).
All of the above abnormalities are indications for referral to an ophthalmologist. The transillumination method is useful for diagnosing cataracts and is also important for determining the surgical indication for infantile cataracts.
Ultrasound (B-scan): Particularly useful when the posterior pole cannot be directly visualized due to opacities of the ocular media. In retinoblastoma, it detects solid tumors and internal calcifications. Coats disease shows no calcification and presents with serous retinal detachment without choroidal mass 6)
MRI: Superior to CT and ultrasound for differentiating retinoblastoma from Coats disease6). Retinoblastoma shows signal intensity similar to brain parenchyma on T1-weighted images and mild hypointensity on T2-weighted images, with contrast enhancement. In Coats disease, subretinal fluid shows T1 hyperintensity and T2 hypointensity, without contrast enhancement 6). Approximately 3% of bilateral retinoblastoma cases develop trilateral retinoblastoma, so screening with head MRI is recommended.
Optical Coherence Tomography (OCT): In MRNFL, hyperreflective nerve fiber layers are observed, and it is also useful for evaluating macular structure 1)3)
QHow should ultrasound and MRI be used differently?
A
Ultrasound is excellent for detecting calcifications and is suitable as an initial screening tool that can be performed quickly in an outpatient setting. MRI is best for differentiating retinoblastoma from Coats disease and persistent fetal vasculature, and can also evaluate optic nerve invasion and choroidal invasion.
Treatment for leukocoria varies greatly depending on the underlying cause. Treatment for each major cause is described below.
Retinoblastoma
Systemic chemotherapy: The standard regimen is a combination of three drugs: vincristine 1.5 mg/m², etoposide 150 mg/m², and carboplatin 560 mg/m²2).
Local therapy: Transpupillary thermotherapy (TTT), laser photocoagulation, and cryotherapy are used in combination with chemotherapy2).
Enucleation: For advanced cases (e.g., Murphree classification Group E), enucleation is performed2). Biopsy of intraocular tumors is generally not performed due to the risk of extraocular tumor cell dissemination.
Coats Disease
Early stage (Stage 1-2): Laser photocoagulation is used to occlude dilated blood vessels6).
Intermediate stage (with significant exudation): Cryotherapy is used to destroy abnormal blood vessels6).
MRNFL itself: This is a benign congenital anomaly and does not require treatment3).
Associated amblyopia: Refractive correction (glasses or contact lenses) and patching (occlusion of the healthy eye) are the basics. Early intervention during the critical period of visual development (up to about 10 years of age) is important1)3).
Concomitant strabismus: If exotropia or other strabismus has a large angle, extraocular muscle surgery is performed3).
QIs treatment necessary for leukocoria due to myelinated nerve fibers?
A
Myelinated retinal nerve fibers (MRNFL) themselves are a benign congenital anomaly and do not require treatment. However, because they are frequently associated with high myopia and amblyopia, early amblyopia treatment with refractive correction and patching affects visual prognosis. For details, see the section “Standard treatment”.
Light from the ophthalmoscope passes through the cornea, anterior chamber, lens, and vitreous to reach the retina. The abundant blood vessels in the choroid beneath the retina reflect light, observed as a red reflex. If there is opacity, tumor, or abnormal structure anywhere in this optical pathway, the red reflex is blocked, resulting in leukocoria.
Biallelic inactivation of the tumor suppressor gene RB1 (located on chromosome 13q14) leads to uncontrolled proliferation of retinal cells2)4).
Heritable form: The patient has a germline mutation in one allele (first hit), and a somatic mutation (second hit) occurs after birth, leading to disease. Often bilateral4)
Sporadic form: Both alleles are inactivated by somatic mutations. Often unilateral
A white retinal tumor directly blocks the red reflex, presenting as leukocoria.
It is a non-hereditary, sporadic disease, and two pathogenic pathways have been proposed6).
Endothelial degeneration pathway: Endothelial cells of retinal blood vessels degenerate, leading to breakdown of the blood-retinal barrier. Plasma leaks through the vessel wall, causing thickening of the vessel wall (sausage-like vessels).
Aneurysm formation pathway: Abnormal interactions between endothelial cells and pericytes lead to the formation of aneurysms. Lipid exudation causes retinal thickening, leading to cyst formation and exudative retinal detachment.
Normally, myelination of nerve fibers occurs only posterior to the lamina cribrosa, and nerve fibers within the retina are unmyelinated. In MRNFL, immaturity or defect of the lamina cribrosa allows oligodendrocyte-like cells to invade the retina and form myelin sheaths around axons of retinal ganglion cells3). Myelin sheaths impede light transmission, so extensive MRNFL is recognized as leukocoria.
7. Latest research and future perspectives (reports under investigation)
Badalova et al. (2025) reported in a retrospective cohort study using the Dutch National Retinoblastoma Registry (1991–2019) that all 28 cases of familial retinoblastoma who were fully screened from birth were diagnosed before 1 year of age (median age at diagnosis 18 days, range 3–352 days). 57.1% were diagnosed within the first month of life, and 82.1% within 6 months. In the incomplete screening group (10 cases), the median age at diagnosis was 420 days. Based on these results, the protocol was revised to shorten screening for the low-risk group (estimated risk <3%) to up to 2 years of age7).
Association of congenital brain malformations and retinoblastoma
Lomi et al. (2025) reported a case of bilateral retinoblastoma in an infant with Dandy-Walker syndrome (DWS). Both DWS and retinoblastoma have been suggested to be associated with chromosome 13q abnormalities, but the coexistence of both diseases is extremely rare. In an MRI study of 168 children with retinoblastoma by Rodjan et al., only one case had a Dandy-Walker variant. This suggests the importance of screening for intraocular malignancy in children with congenital brain malformations2).
It has been discussed that in vitro fertilization (IVF) may increase the risk of developing retinoblastoma through epigenetic abnormalities. A Dutch study suggested an increased incidence of retinoblastoma after IVF, but multiple large-scale epidemiological studies have not found a significant association, and the conclusion remains inconclusive 4).
The triad of myelinated retinal nerve fibers (MRNFL), myopia, and amblyopia is called Straatsma syndrome. Factors associated with visual prognosis include the type of MRNFL (type 1: only superior arcade, type 2: both superior and inferior arcades, type 3: not continuous with the optic disc), the degree of anisometropia, and the structure of the macular ellipsoid zone on OCT. Type 2 had the poorest prognosis and also showed poor response to amblyopia treatment 1).
Altamirano F, Gonzalez E, Oke I.. Leukocoria in a 4-year-old boy. Digit J Ophthalmol. 2024;30(2):42-44. doi:10.5693/djo.02.2024.03.005. PMID:38962670; PMCID:PMC11218840.
Lomi N, Das D, Chawla B, Parampalli Ravindra A. Retinoblastoma in Dandy-Walker Syndrome. Cureus. 2025;17(8):e89663. doi:10.7759/cureus.89663. PMID:40926918; PMCID:PMC12415497.
Alghofaili RS, Almesfer SA.. Bilateral Retinoblastoma Presenting in an in vitro Fertilization Infant with Retinopathy of Prematurity. Case Rep Ophthalmol. 2021;12(1):306-310. doi:10.1159/000513181. PMID:34054475; PMCID:PMC8138227.
Bafna RK, Mahalingam K, Bansal B. Hyperoleon masquerading as leukocoria. BMJ case reports. 2021;14(9). doi:10.1136/bcr-2021-246135. PMID:34544725; PMCID:PMC8454427.
Laasri K, El Houss S, Halfi IM, Kettani NE, Fikri M, Jiddane M, et al. Coats’ syndrome: A rare cause of infant leukocoria to keep in mind. Radiology case reports. 2024;19(1):7-11. doi:10.1016/j.radcr.2023.09.046. PMID:37881471; PMCID:PMC10594555.
Badalova NA, van Hoefen Wijsard M, Dommering CJ, et al. At What Age Could Screening for Familial Retinoblastoma Be Stopped? Ophthalmology. 2025;132:1152-1160.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.