Medulloepithelioma is a rare intraocular tumor arising from the nonpigmented ciliary epithelium. The nonpigmented ciliary epithelium is derived from embryonic neural tube epithelium, and medulloepithelioma exhibits a distinctive histology reflecting its multipotent differentiation. It was once described as a tumor related to retinoblastoma.
The most common site of origin is the ciliary body; cases arising from the optic nerve or retina are rare. It occurs predominantly in children, especially between 1 and 10 years of age, and is exceptional in adults. In an analysis of 41 cases by Kaliki et al., the median age at diagnosis was 5 years 1. It is a very rare tumor, making it difficult to determine the exact incidence, and it is extremely uncommon in ophthalmic practice 2.
The most important clinical challenge is differentiating it from retinoblastoma, which also occurs in children of the same age and presents with leukocoria. Definitive diagnosis is often made by histopathological examination after enucleation.
QHow is medulloepithelioma different from retinoblastoma?
A
Both occur in children’s eyes and present with leukocoria. However, medulloepithelioma arises from the nonpigmented ciliary epithelium (neuroepithelium), whereas retinoblastoma arises from undifferentiated retinal cells. On imaging, retinoblastoma is characterized by calcification (CT) and multifocal lesions, while medulloepithelioma often forms a mass in the ciliary body. Ultrasound biomicroscopy (UBM) to confirm a ciliary body mass is useful for differentiation, but definitive diagnosis relies on histopathology.
Medulloepithelioma is often asymptomatic in the early stages and may be discovered incidentally by parents or during infant health checkups due to abnormal red reflex. The main discovery triggers are listed below.
Leukocoria: The most important sign. The pupil appears white, often noticed by parents during photography.
Cataract: Caused by the tumor compressing the lens.
Glaucoma: Due to obstruction of aqueous humor outflow by the tumor.
Proptosis: Seen when extraocular extension has progressed.
In an analysis of 41 cases by Kaliki et al., secondary glaucoma was found in 44%, iris neovascularization in 51%, cataract in 46%, and lens subluxation in 27%, with leukocoria, secondary glaucoma, and lens abnormalities reported as a characteristic clinical triad 13.
After pupillary dilation, anterior segment examination and gonioscopy reveal a white to yellowish-white mass in the ciliary body region. The surface of the mass is irregular and may contain cystic structures.
Histological Features of Benign Type
Nonteratoid type: Forms neuroepithelial-like tubular structures.
Teratoid type: Contains heterotopic tissues such as cartilage and striated muscle in addition to neuroepithelial-like structures.
Common: Mild nuclear atypia, few infiltrative findings and mitotic figures.
Histological Features of Malignant Type
Infiltrative findings: Clear infiltration into surrounding tissues.
Mitotic figures: Numerous mitotic figures.
Risk of extraocular extension: Infiltration into the sclera and orbit, and metastasis may occur.
As the tumor enlarges and extends outside the eye, proptosis and ocular motility disturbances appear. Secondary glaucoma may cause elevated intraocular pressure and corneal edema.
Medulloepithelioma is thought to arise from an embryonal developmental abnormality of the nonpigmented ciliary epithelium. The formation of neuroepithelial tubules during normal development is presumed to be involved in tumorigenesis, but the specific mechanisms remain largely unknown.
No specific environmental risk factors have been established. There is also a lack of clear data on sex, regional, or racial differences.
As a genetic background, association with DICER1 gene mutations has been reported in some cases. DICER1 mutations are causative genes for a cancer predisposition syndrome (DICER1 syndrome) that causes multi-organ tumors such as pleuropulmonary blastoma, renal tumors, and thyroid tumors, and it has been reported that ciliary medulloepithelioma can appear as a manifestation of familial tumor predisposition syndrome associated with pleuropulmonary blastoma 45. Furthermore, in sporadic cases, somatic DICER1 mutations have been identified in tumor tissue, suggesting that abnormalities in the DICER1 pathway may be involved in tumorigenesis 6. However, most medulloepitheliomas are sporadic, and familial cases are limited to a small number.
In the teratoid type, since various heterotopic tissues such as cartilage and striated muscle are included, it is thought that pluripotent cells are involved in tumor formation. This is consistent with the fact that the nonpigmented ciliary epithelium retains multipotent differentiation capacity during the embryonic period.
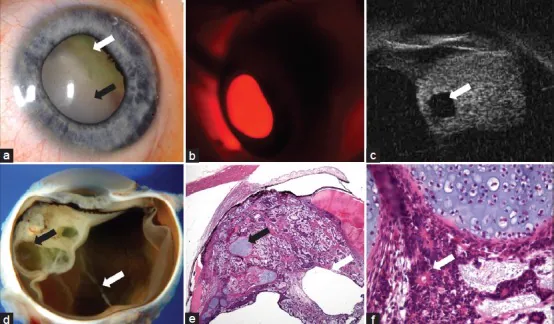
Stathopoulos C, Gaillard MC, Schneider J, et al. Successful treatment of ciliary body medulloepithelioma with intraocular melphalan chemotherapy: a case report. BMC Ophthalmol. 2020;20:243. Figure 2. PMID: 32552699; PMCID: PMC7302148. DOI: 10.1186/s12886-020-01512-y. License: CC BY 4.0.
Six-panel images of medulloepithelioma arising from the ciliary body of the left eye in a 22-month-old girl: (a) Yellow-white ciliary mass and subluxated lens observed on slit-lamp photography, (b) Limbus shadow on transillumination, (c) Ultrasound biomicroscopy (UBM) image showing a solid ciliary mass with cystic spaces, (d) Gross section of the enucleated eye showing the mass and cysts, (e)(f) Histopathological images showing cords of neuroepithelial cells, hyaline cartilage, cystic structures, and Flexner-Wintersteiner rosettes. This corresponds to the depiction of ciliary cystic masses by ultrasound biomicroscopy (UBM) discussed in the section “4. Diagnosis and Examination Methods.”
Ultrasound biomicroscopy (UBM) is the most useful examination for confirming and evaluating the morphology of ciliary body masses. It can depict solid or mixed cystic-solid masses adjacent to the ciliary body, and can assess the extent of the mass, its relationship with the ciliary body, and the presence of anterior segment invasion. In the analysis by Kaliki et al., intratumoral cysts were confirmed in 61% of cases, and the depiction of cystic structures on UBM is a finding strongly suggestive of this disease 1.
MRI is used to evaluate tumor extent and extraocular invasion. When orbital or optic nerve invasion is suspected, it provides essential information for treatment planning.
CT scan is useful for evaluating the presence of calcification and helps in differentiation from retinoblastoma (retinoblastoma frequently shows calcification).
Fundus examination and anterior segment examination are performed using slit-lamp microscopy and indirect ophthalmoscopy under mydriasis. Direct observation of the ciliary mass and assessment of associated retinal complications (such as serous retinal detachment) are performed.
Definitive diagnosis is often made by histopathological examination after enucleation. Because biopsy of the ciliary body is technically difficult and carries a risk of tumor seeding, when medulloepithelioma is strongly suspected based on clinical and imaging findings, enucleation is generally performed first.
Histopathologically, it is diagnosed as an epithelial tumor forming tubular, papillary, or sheet-like structures resembling embryonic neuroepithelium. In the teratoid type, the presence of heterotopic tissues such as cartilage, striated muscle, and brain-like components is characteristic.
Characterized by leukocoria, calcification on CT, and multifocality. Arises from the retina. Medulloepithelioma primarily presents as a ciliary body mass.
Ciliary Body Melanocytoma
Benign and heavily pigmented. Common in middle-aged and elderly individuals; appears as a hyperechoic mass on UBM.
Ciliary Body Malignant Melanoma
Occurs in middle-aged and elderly individuals. Pigmented mass, sometimes accompanied by sentinel vessels.
Congenital. Forms a fibrovascular membrane in the vitreous, presenting with leukocoria.
QA white area is seen in a child's eye. What could it be?
A
Leukocoria in children is an urgent finding requiring prompt evaluation by an ophthalmologist. Main differential diagnoses include retinoblastoma, medulloepithelioma, persistent hyperplastic primary vitreous (PHPV), congenital cataract, Coats disease (exudative retinopathy), and ocular toxocariasis. Among these, retinoblastoma and medulloepithelioma are malignant tumors, and delayed diagnosis can affect prognosis; therefore, immediate referral to a specialist is crucial.
For small tumors strongly suspected to be benign, local resection by cyclectomy is an option. However, surgical access to the ciliary body is technically challenging, and the number of facilities and surgeons capable of performing it is limited. Also, there is a risk of tumor recurrence after resection, so careful patient selection and strict postoperative follow-up are necessary.
If extraocular extension has progressed and the tumor involves the orbit, orbital exenteration is required. Because it is highly invasive and causes postoperative cosmetic problems, the indication is carefully considered.
Good prognosis after enucleation if no metastasis. Low local recurrence rate.
Malignant type
Risk of extraocular invasion and distant metastasis. Poor prognosis if metastasis occurs.
Extraocular invasion cases
Need to monitor for local recurrence and metastasis even after orbital exenteration.
Distant metastasis is relatively rare, but careful follow-up is required for malignant types and cases with extraocular invasion. If metastasis occurs, treatments such as chemotherapy and radiation therapy are considered, but no standard regimen has been established.
Medulloepithelioma originates from the nonpigmented ciliary epithelium. The nonpigmented ciliary epithelium is formed from neuroepithelium derived from the neural tube during embryonic development. Therefore, the histology of medulloepithelioma shows tubular, papillary, and sheet-like structures resembling embryonic neural tube epithelium.
Nonteratoid type forms only neuroepithelial-like tubular and papillary structures. It is the type closest to the morphology of normal neural tube epithelium. Cells are columnar to cuboidal and may show pseudostratified arrangement.
Teratoid type contains diverse tissues such as cartilage, striated muscle, and brain-like components in addition to neuroepithelial-like structures. This reflects the high pluripotency of the tumor-initiating cells, resulting in histology resembling teratoma. Benign teratoid type shows few nuclear atypia and mitotic figures, and remains well-circumscribed.
Histological differences between benign and malignant types
In malignant types, the following findings are observed in addition to neuroepithelial-like structures:
Severe nuclear atypia and multinucleated cells
Numerous mitotic figures
Invasion into surrounding tissues (sclera, orbital fat, iris, ciliary muscle)
Formation of necrotic foci
These findings serve as the basis for determining malignancy and predicting prognosis. Intermediate types with ambiguous boundaries between benign and malignant have also been reported, and pathological diagnosis requires experience.
In malignant types, the main route is considered to be tumor cell invasion into the orbit through the emissary canals. Hematogenous metastasis is thought to occur via the rich vascular network of the ciliary body, but the detailed mechanisms are still under investigation.
7. Latest research and future perspectives (research-stage reports)
The DICER1 gene encodes an RNase III enzyme involved in the biosynthesis of small RNAs. Germline mutations in DICER1 cause DICER1 syndrome, which is associated with multiple tumors such as pleuropulmonary blastoma, renal tumors, and thyroid tumors. Recently, DICER1 mutations have been reported in some medulloepitheliomas, drawing attention to the association between ocular tumors and DICER1 syndrome.
Identification of DICER1 mutations may be important for selecting candidates for genetic counseling and considering the indication for family genetic screening. Recent clinicopathological analyses of ciliary body medulloepithelioma have again pointed out the importance of systematic evaluation incorporating molecular genetic testing 7.
Refinement of criteria for distinguishing benign and malignant tumors
Medulloepithelioma is a rare disease, making large-scale clinical studies difficult. Accumulation of large case series by specialized ocular oncology centers, such as those by Shields et al., has contributed to refining the pathological criteria for distinguishing benign and malignant tumors. Standardization of quantitative evaluation criteria for mitotic count and invasion findings remains a future challenge.
Expanding indications for local resection (ciliary body resection) for small, benign-type medulloepithelioma are being considered. While it may be possible to avoid enucleation and preserve visual function, risk management of postoperative recurrence and establishment of long-term follow-up protocols are required.
Clinical Differences Between Teratoid and Non-Teratoid Types
Whether there are differences in malignancy frequency, extraocular invasion risk, and prognosis between teratoid and non-teratoid types has not been fully elucidated. Comparative studies through large-scale multicenter research are expected.
Tadepalli SH, Shields CL, Shields JA, Honavar SG. Intraocular medulloepithelioma - A review of clinical features, DICER 1 mutation, and management. Indian J Ophthalmol. 2019;67(6):755-762. doi:10.4103/ijo.IJO_845_19. PMID: 31124483; PMCID: PMC6552580. ↩↩2
Peshtani A, Kaliki S, Eagle RC, Shields CL. Medulloepithelioma: A triad of clinical features. Oman J Ophthalmol. 2014;7(2):93-95. doi:10.4103/0974-620X.137171. PMID: 25136238; PMCID: PMC4134557. ↩
Kramer GD, Arepalli S, Shields CL, Shields JA. Ciliary body medulloepithelioma association with pleuropulmonary blastoma in a familial tumor predisposition syndrome. J Pediatr Ophthalmol Strabismus. 2014;51:e48-e50. doi:10.3928/01913913-20140709-03. PMID: 25032694. ↩
Priest JR, Williams GM, Manera R, Jenkinson H, Bründler MA, Davis S, Murray TG, Galliani CA, Dehner LP. Ciliary body medulloepithelioma: four cases associated with pleuropulmonary blastoma—a report from the International Pleuropulmonary Blastoma Registry. Br J Ophthalmol. 2011;95(7):1001-1005. doi:10.1136/bjo.2010.189779. PMID: 21156700. ↩
Durieux E, Descotes F, Nguyen AM, Grange JD, Devouassoux-Shisheboran M. Somatic DICER1 gene mutation in sporadic intraocular medulloepithelioma without pleuropulmonary blastoma syndrome. Hum Pathol. 2015;46(5):783-787. doi:10.1016/j.humpath.2015.01.020. PMID: 25791583. ↩
August AH, Cernichiaro-Espinosa LA, Moctezuma-Davila M, Wibbelsman TD, Wilson MW, Chévez-Barrios P, Shields CL, Lally SE, Eberhart CG, Orr BA, Simpson E, Eagle RC, Milman T. Ciliary Body Medulloepithelioma: Clinical and Pathologic Challenges with a Focus on Molecular Genetics. Semin Ophthalmol. 2025;40(6):518-528. doi:10.1080/08820538.2025.2457066. PMID: 39869033. ↩
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.