Iris cyst is a general term for cystic lesions that occur within the iris. Based on differences in pathogenesis and tissue origin, they are mainly classified into two types: iris stromal cyst and iris pigment epithelial cyst2. Both are relatively rare, and in cases with a history of trauma or surgery, iris stromal cyst should be considered. They may also be discovered incidentally during or after cataract surgery1.
Iris stromal cyst (iris epithelial cyst) arises from ectodermal implantation during embryonic development (congenital) or from surgery/trauma within the iris stroma. The cyst wall is composed of thin stratified epithelium similar to conjunctiva, often containing mucous cells. When enlarged, it can contact the corneal endothelium and cause irreversible corneal opacity that is difficult to treat.
Iris pigment epithelial cyst results from separation between the two layers of pigment epithelium on the posterior iris surface. Most are acquired and commonly occur at the iris root (border with the ciliary body). Enlargement can cause lens dislocation or cataract, but most follow a slow course.
QIs it okay to leave an iris cyst untreated?
A
It depends on the type. For iris pigment epithelial cysts that are small and asymptomatic, observation is the rule, and most progress slowly. On the other hand, iris stromal cysts can cause corneal opacity and mucogenic glaucoma when enlarged, so early surgical intervention or aspiration is recommended. Slit-lamp examination, anterior segment OCT, and UBM are necessary to determine the type.
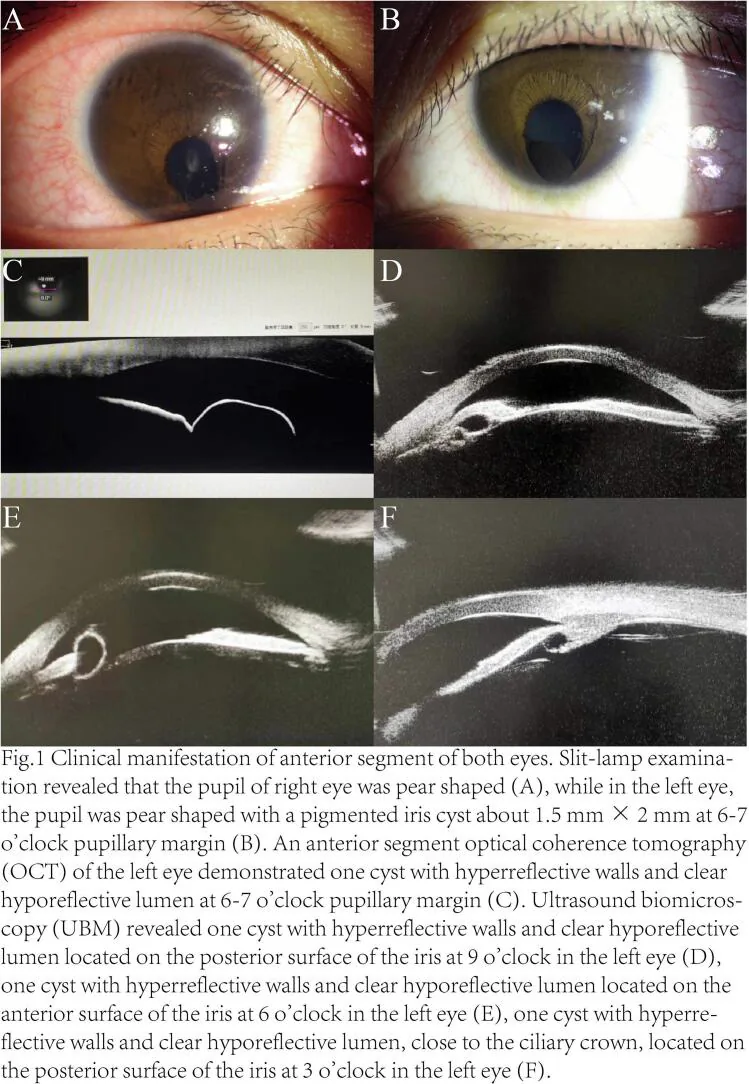
Song XZ, et al. Congenital bilateral coloboma of iris and choroid accompanied by unilateral multiple primary pigmented iris cysts: A case report. Int J Surg Case Rep. 2024. Figure 1. PMCID: PMC11615603. License: CC BY.
A pigmented iris cyst measuring 1.5 × 2 mm at the pupillary border from 6 to 7 o’clock in the left eye is seen on slit-lamp (B). AS-OCT (C) shows a hyperreflective wall and hyporeflective lumen, and UBM (D–F) reveals multiple cysts with hyporeflective cavities near the posterior and anterior iris surface and ciliary body crown. This corresponds to an iris pigment epithelial cyst discussed in the section “2. Main symptoms and clinical findings.”
An iris stromal cyst appears as a transparent to translucent elevation in the anterior segment. As it enlarges, the following changes occur.
Irreversible corneal opacity due to contact with the corneal endothelium
Pupillary dilation disorder and visual field defect
Mucous secretion from the cyst wall mixing into the aqueous humor (mucogenic glaucoma)
Decreased vision and headache due to elevated intraocular pressure
Mucogenic glaucoma is a serious complication of stromal cysts. Mucus obstructs the trabecular meshwork, causing a rapid rise in intraocular pressure. Complete excision of the cyst wall without residue is essential for prevention.
An iris pigment epithelial cyst is observed as a black cyst on the posterior surface of the iris. Direct visualization with a slit lamp is often difficult, and it is delineated by anterior segment OCT. When enlarged, the following problems occur.
A non-pigmented cyst located at the iris root, i.e., the border with the ciliary body, is called a ciliary epithelial cyst. It may occur secondary to a ciliary body tumor. Detailed evaluation with UBM is necessary for diagnosis.
Iris Stromal Cyst
Appearance: Transparent to translucent elevation in the anterior segment of the eye
Pathogenesis: Ectodermal choristoma (congenital) or epithelial inclusion after trauma/surgery
Main complications: Corneal opacity, mucogenic glaucoma
Treatment strategy: Early surgery or needle aspiration. Complete excision of the cyst wall is required
Iris pigment epithelial cyst
Appearance: Black cyst on the posterior surface of the iris (confirmed by anterior segment OCT)
Pathogenesis: Dissection due to aqueous humor penetration between the two layers of the pigment epithelium
Congenital iris stromal cysts occur when ectodermal epithelium becomes entrapped within the iris stroma during embryonic development. Acquired cysts are caused by epithelial inclusion following trauma or intraocular surgery.
These cysts occur when aqueous humor penetrates and dissects between the two layers of the iris pigment epithelium. They may also develop secondary to ciliary body tumors. Although specific risk factors are not clearly defined, the following are considered associated:
Age-related changes
Ciliary body neoplastic lesions (e.g., ciliary body adenoma, adenocarcinoma)
This is the first examination to confirm cystic lesions in the anterior segment.
Stromal cysts appear as transparent to translucent elevations in the anterior segment.
Pigment epithelial cysts are located behind the iris and may be difficult to visualize directly.
Non-invasively evaluates the depth, size, and wall structure of cysts.
Particularly useful for imaging iris pigment epithelial cysts.
Also helps determine the nature of the cyst lumen (fluid-filled vs. solid).
An examination using high-frequency ultrasound that allows detailed evaluation of posterior cysts and their positional relationship with the ciliary body.
Excellent for evaluating areas difficult to image with anterior segment OCT (ciliary body, angle region) 2.
Essential for evaluating ciliary body epithelial cysts and cysts secondary to ciliary body tumors.
UBM studies have shown that 84.4% of iris pigment epithelial cysts involve the iris pigment epithelium, and approximately 74% remain stable over one year of follow-up 3.
Light is applied from the scleral side to check the translucency of ciliary body cysts.
Useful for differentiating from ciliary body tumors.
Solid tumors have low translucency, while cystic lesions show high translucency.
Malignant tumors (such as iris malignant melanoma) are often solid, and solid components are confirmed inside by anterior segment OCT or UBM. Cystic lesions (iris cysts) have a liquid lumen and high translucency. Additionally, if accompanied by rapid enlargement, congestion, increased intraocular pressure, or ciliary injection, malignancy should be considered and prompt detailed examination is necessary. If the diagnosis is uncertain, referral to a specialized tumor center is recommended.
Iris stromal cysts can enlarge and cause irreversible complications if left untreated, so early intervention is the principle.
Needle aspiration is a temporary measure performed when the cyst shows a tendency to enlarge. It temporarily reduces the cyst and prevents contact with the cornea. However, because the cyst wall remains, there is a risk of recurrence 2. Recently, combined aspiration and absolute alcohol-induced sclerosis has been reported to achieve cyst regression in 14 of 16 cases (93%), and is attracting attention as a minimally invasive option 4.
Surgical excision (complete removal) is the curative treatment. Complete removal of the cyst wall prevents the development of mucogenic glaucoma. Intervention before corneal opacity occurs is important for visual prognosis. Incomplete resection leads to recurrence, so the surgeon aims to remove the entire cyst wall without leaving any remnants 2.
Observation is the basic policy. Small, asymptomatic cysts are monitored regularly with anterior segment OCT or UBM. Most progress slowly and remain stable without intervention 1,5. In pediatric studies, most primary pigment epithelial cysts do not require treatment, and only iris stromal cysts require needle aspiration, cryotherapy, or surgical excision 5.
Partial cyst wall resection during cataract surgery is considered in the following cases:
The cyst shows a tendency to enlarge
Complications such as lens dislocation or cataract have occurred
When securing a surgical field is necessary
The cyst is reduced by partial resection of the cyst wall simultaneously with cataract surgery. Complete resection is often technically difficult, so partial resection is used.
With appropriate treatment, the prognosis is good.
Iris stromal cysts rarely recur if completely excised.
Incomplete excision carries a risk of recurrence, requiring long-term follow-up.
Iris pigment epithelial cysts usually follow a slow course and rarely cause severe visual impairment.
Congenital iris stromal cysts arise from ectopic ectodermal epithelium that becomes entrapped within the iris stroma during embryonic eye development.
The ectopic epithelium forms the cyst wall and becomes stratified squamous epithelium with secretory function.
In acquired cases, corneal or conjunctival epithelium is carried into the eye (epithelial inclusion) during trauma or surgery.
The entrapped epithelium proliferates within the iris stroma and forms a cyst.
The stratified epithelium composing the cyst wall continuously secretes mucus.
When this mucus mixes with the aqueous humor, it can obstruct the trabecular meshwork, causing increased intraocular pressure (mucogenic glaucoma).
Persistent elevated intraocular pressure leads to optic nerve damage (glaucomatous visual field loss).
On the posterior surface of the iris, there are two layers of pigment epithelium: the inner layer (derived from the neural layer) and the outer layer (pigment epithelial layer).
Aqueous humor penetrates and accumulates between these two layers, causing separation and cyst formation.
When secondary to ciliary body tumors, it is thought that fluid produced by the tumor accumulates between the two layers, leading to cyst formation.
Enlargement of pigment epithelial cysts is usually slow, but when the cyst becomes large, it can compress and displace the lens anteriorly.
Lens displacement can cause irregular astigmatism and decreased vision.
Furthermore, persistent compression of the lens may lead to cataract formation.
The mucus (mucin) secreted by iris stromal cysts is more viscous than aqueous humor.
When mucus enters the aqueous humor, it physically obstructs the trabecular meshwork.
This obstruction of aqueous outflow causes a rapid rise in intraocular pressure, leading to glaucoma.
For this reason, if the cyst wall remains, mucus secretion continues postoperatively, and intraocular pressure elevation recurs.
Complete excision is essential for a cure.
Nd:YAG laser cyst wall destruction has been reported as a minimally invasive alternative to surgery. This procedure creates a perforation in the cyst wall with a laser to drain the cyst contents into the anterior chamber. Efficacy has been shown at the case report level, but data on recurrence rates and long-term prognosis are limited. Indications are carefully determined considering cyst size, location, distance from the corneal endothelium, and other factors.
Trends in new classification using anterior segment OCT and UBM
Advances in high-resolution anterior segment OCT and UBM have enabled more detailed morphological evaluation of iris cysts. A new classification that objectively assesses cyst wall structure, lumen characteristics, and relationship with surrounding tissues is being considered. This is expected to standardize treatment indications and improve prognostic accuracy.
Atropine eye drops used for treating myopia in children may influence the formation or enlargement of iris pigment epithelial cysts. It is hypothesized that the mydriatic and cycloplegic effects of atropine are involved in fluid accumulation between pigment epithelial layers, but the detailed mechanism and clinical significance require further research.
Georgalas I, Petrou P, Papaconstantinou D, Brouzas D, Koutsandrea C, Kanakis M. Iris cysts: A comprehensive review on diagnosis and treatment. Surv Ophthalmol. 2018;63(3):347-364. PMID: 28882598. PubMed
Liu D, Lutchman CR, Persad K, Simpson ER. Evaluation of the characteristics of primary iridociliary cysts using ultrasound biomicroscopy at a tertiary care centre. Can J Ophthalmol. 2023;58(3):243-249. PMID: 35157832. PubMed
Shields CL, Arepalli S, Lally EB, Lally SE, Shields JA. Iris stromal cyst management with absolute alcohol-induced sclerosis in 16 patients. JAMA Ophthalmol. 2014;132(6):703-708. PMID: 24723076. PubMed
Shields JA, Shields CL, Lois N, Mercado G. Iris cysts in children: classification, incidence, and management. The 1998 Torrence A Makley Jr Lecture. Br J Ophthalmol. 1999;83(3):334-338. PMID: 10365043. PubMed
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.