Ciliary body malignant melanoma is a malignant tumor arising from melanocytes of the ciliary body. Among uveal melanomas originating from melanocytes of the uvea (iris, ciliary body, choroid), ciliary body origin accounts for about 7% 2).
When a ciliary body tumor is discovered, it should first be considered as possible malignant melanoma. Ciliary body malignant melanoma is observed as a dark brown elevation of the ciliary body through the pupil, but since the tumor arises from the ciliary body stroma, what is directly observed is the color of the pigment epithelium. Therefore, whether the tumor is pigmented or not is determined by transillumination.
The incidence of uveal melanoma overall in Japan is about 1/20 of that in Western countries, with 0.025 per 100,000 population. It most commonly arises from the choroid, less frequently from the ciliary body. It occurs in middle-aged and elderly individuals, with a slight male predominance.
Metastasis is exclusively hematogenous (since the uvea lacks lymphatics) and shows a strong tropism for the liver. The median overall survival after metastasis was previously less than 6 months, but is improving with the advent of tebentafusp.
QHow is ciliary body melanoma discovered?
A
The ciliary body is difficult to visualize on fundus examination; it is often discovered through anterior segment observation after pupil dilation (gonioscopy, slit lamp) or triggered by symptoms such as visual loss, sentinel vessels, or secondary glaucoma. It is difficult to detect during health checkups, so prompt ophthalmologic consultation upon symptom onset is important.
Subjective symptoms of ciliary body melanoma exhibit the following characteristics due to the peculiarities of its anatomical location3).
Painless vision loss (blurring): The most common complaint.
Astigmatism due to lens displacement: Caused by anterior displacement of the lens-iris diaphragm by the tumor.
Painless visual field defect when the visual axis is invaded: Occurs when the tumor extends into the vitreous cavity.
Painful vision loss due to acute intraocular pressure elevation: Caused by secondary angle-closure glaucoma. Secondary intraocular pressure elevation is observed in up to 17% of cases at diagnosis3).
Examination of the anterior segment after pupillary dilation reveals a dark brown elevated lesion in the ciliary body region. The following findings provide diagnostic clues.
Ciliary Body Melanoma
Size at detection: Due to its anatomically hidden location, it is often relatively large at the time of detection.
Sentinel vessels: Dilated and tortuous episcleral vessels directly over the tumor are frequently present. This is an important diagnostic clue.
Anterior segment changes: Anterior displacement of the lens-iris diaphragm and secondary angle-closure glaucoma are common.
Extraocular extension: There is a risk of extraocular extension via emissary canals.
Comparison with Choroidal Melanoma
Location: The ciliary body is anterior, making it difficult to observe on fundus examination. The choroid can be seen on fundus examination.
Symptom characteristics: In ciliary body melanoma, lens displacement, astigmatism, and secondary glaucoma tend to be prominent. In choroidal melanoma, photopsia, floaters, and visual field defects are more common.
Difficulty of diagnosis: Examination of the anterior segment, UBM, and transillumination are essential for the ciliary body. Fundus photography and ultrasound are used for the choroid.
Other important clinical findings include iris root abnormalities (compression or deformation by the tumor) and lens displacement or deformation (abnormal anterior segment morphology). As the tumor grows, it may be complicated by vitreous hemorrhage or cataract.
Ciliary body malignant melanoma arises from neoplastic proliferation of melanocytes in the ciliary body. Malignant transformation from uveal nevus can also occur.
Major risk factors are listed below.
Light iris color, fair skin, tendency to sunburn: More common in Caucasians and Nordic populations.
Congenital ocular melanocytosis or melanocytoma: Rare risk factors.
Family history of uveal melanoma: Rare but reported.
The correspondence between gene mutations and metastasis risk is shown below1).
Mutated gene
Mutation frequency
Metastasis risk / Characteristics
GNAQ/GNA11
83–89%
Mutually exclusive initiating mutations. No direct association with metastasis risk.
BAP1
45%
Highest metastasis risk (peak at 3.5 years), class 2
SF3B1
23%
Moderate risk. Characterized by late metastasis (peak at 7 years)
EIF1AX
17%
Lowest metastasis risk
GNAQ/GNA11 mutations are considered early events in tumor formation, and mutations alone are not significantly associated with tumor size or metastasis risk. Secondary driver mutations in BAP1, SF3B1, and EIF1AX occur almost completely mutually exclusive of each other and have important implications for metastasis risk stratification 7).
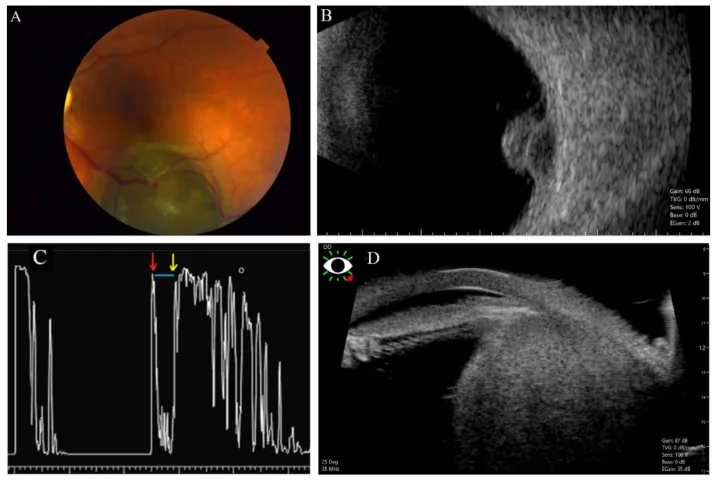
Solnik M, Paduszyńska N, Czarnecka AM, et al. Imaging of Uveal Melanoma-Current Standard and Methods in Development. Cancers (Basel). 2022;14(13):3147. Figure 3. PMID: 35804919; PMCID: PMC9265106; DOI: 10.3390/cancers14133147. License: CC BY.
(A) Fundus photograph showing a mushroom-shaped choroidal melanoma, (B) B-mode ultrasound image with acoustic hollowing, (C) A-mode ultrasound waveform showing low internal reflectivity of the tumor (red arrow: retinal surface, yellow arrow: scleral surface, blue line: low-reflectivity area within the tumor), (D) Ciliary body melanoma imaged by ultrasound biomicroscopy (UBM). Corresponds to the ciliary body melanoma image by UBM (ultrasound biomicroscopy) discussed in the section “4. Diagnosis and Examination Methods”.
Transillumination Examination (Important for Differential Diagnosis)
In a dark room, an endoscopic light source is applied externally to the sclera, and whether light transmits through is observed through the pupil. This transillumination test is the most important basic examination for determining the nature of ciliary body tumors.
Malignant melanoma (pigmented): No translucency (light does not pass through)
This is the most important imaging test for evaluating the size, shape, and internal echoes of ciliary body tumors. High-frequency ultrasound can visualize detailed morphology of the ciliary body. It is excellent for assessing tumor margins, internal reflectivity, and invasion into adjacent structures (iris, angle, lens).
It shows high signal on T1-weighted images and low signal on T2-weighted images, but other ciliary body tumors often show similar findings, and contrast enhancement is often weak. Diagnosis by MRI alone is difficult and should be evaluated in combination with other findings.
Management: Regular monitoring with UBM; if growth is observed, consider resection and pathological examination.
Ciliary body epithelial cyst
Transillumination: Present (due to cyst fluid).
Features: May become free-floating in the vitreous.
Differential diagnosis: UBM confirms the characteristics of the cyst wall and fluid.
Ciliary body adenoma/adenocarcinoma
Origin: Arises from the epithelium of the ciliary body (non-pigmented or pigmented epithelium).
Frequency: Rare tumors; histopathological examination is necessary to differentiate from other ciliary body tumors.
QI was told there is a lump in the ciliary body. Is it definitely cancer?
A
Ciliary body tumors include benign ones. Benign tumors such as leiomyoma, melanocytoma, and epithelial cysts also occur, so it is not necessarily malignant melanoma. Detailed evaluation is performed with transillumination, UBM, MRI, etc., and depending on growth tendency and symptoms, observation, surgery, or radiation therapy is selected.
When the tumor is relatively small and located anteriorly, local resection (transscleral tumor excision) that removes only part of the sclera and the tumor may be selected. This can serve both as a definitive diagnosis and treatment.
Radiation therapy is the main option for eye preservation.
Heavy ion therapy (e.g., HIMAC): Particle therapy that concentrates radiation dose on the tumor using the Bragg peak effect. Indications are expanding recently.
CyberKnife: One option for stereotactic radiotherapy.
Brachytherapy (Ru-106): Ruthenium-106 plaque is sutured onto the sclera.
Proton therapy: An eye-preserving treatment with low radiation dose to surrounding normal tissues.
Even in suspected cases, radiation therapy such as heavy ion therapy may be considered.
For large tumors where eye preservation is difficult, enucleation is selected. Definitive diagnosis is made from the enucleated specimen.
Biopsy depending on the situation
Transscleral, transcorneal, or transpupillary biopsy may also be considered. Considering intratumoral heterogeneity, sampling from morphologically different areas is recommended 7).
Tebentafusp for metastatic uveal melanoma is indicated for HLA-A*02:01-positive patients 5). In a phase III trial, it was the first drug to significantly improve overall survival in metastatic uveal melanoma.
Based on the 2023 updated UK Uveal Melanoma Guidelines, the following surveillance is recommended 1).
Basic program: every 6 months for 5 years, then annually for 10 years.
SF3B1 mutation carriers: consider extended surveillance up to 15 years.
Same after enucleation: continue metastasis surveillance even after local treatment is completed.
The prognosis tends to be poor, similar to choroidal melanoma. Liver metastasis determines the prognosis, and metastasis may become apparent several years to more than 10 years after enucleation.
QIs there a treatment that can preserve the eye?
A
For small to medium-sized tumors, eye-preserving therapies such as transscleral tumor resection, heavy particle therapy, brachytherapy (Ru-106), and proton beam therapy can be selected. For large tumors, enucleation may be necessary, but it has been shown that the choice of local treatment does not affect the metastasis rate or overall survival. While prioritizing life prognosis, the possibility of preservation should be discussed at a specialized facility.
The pathogenesis of uveal melanoma involves unique molecular pathways distinct from those of cutaneous melanoma.
Mutations at the Q209 position of GNAQ/GNA11 are most frequently detected. These mutations impair GTPase activity, leading to a constitutively active GTP-bound state. GNAQ/GNA11 mutations result in sustained activation of multiple signaling pathways, including the MAPK pathway (Ras/RAF/MEK/ERK) 6).
Secondary driver mutations (BAP1, SF3B1, EIF1AX) occur almost completely mutually exclusive of each other and have important implications for stratifying metastasis risk 7).
Because the ciliary body is located anterior to the choroid, it is prone to invasion into the iris and angle. This contributes to secondary angle-closure glaucoma. Additionally, anterior tumor extension can cause lens displacement and cataract.
Extraocular extension occurs via emissary canals, leading to orbital and systemic spread.
Since the uvea lacks lymphatic vessels, all metastases occur hematogenously 2). The strong tropism for the liver is explained by the seed and soil theory. In metastatic lesions, GNAQ (57%) and GNA11 (36%) are detected mutually exclusively.
Intratumoral VEGF concentration is significantly higher than in healthy eyes. A case of rapid growth of ciliary body melanoma after intravitreal bevacizumab injection has been reported (basal diameter 2.51→18.0 mm, height 6.23→11.0 mm over 7 weeks) 4), and intravitreal administration of anti-VEGF drugs may be contraindicated.
Intratumoral heterogeneity exists both morphologically and genetically, affecting the prognostic accuracy of biopsy 7). While monosomy 3 is common across tumor sites, 6q deletion may be limited to pigmented areas in some cases.
7. Latest Research and Future Perspectives (Investigational Reports)
Tebentafusp is a T-cell receptor bispecific fusion protein designed for HLA-A02:01-positive patients 5). It recognizes the tumor-associated antigen gp100 on the HLA-A02:01 complex and activates T cells to exert antitumor effects. It is the first drug to significantly improve overall survival in metastatic uveal melanoma in a phase III trial, and 3-year overall survival data are being accumulated 11).
In a case report by Krohn et al. (2025), a favorable course was recorded after 26 months of tebentafusp (weekly IV: 20→30→68 mg escalation) with stable liver metastases and no new lesions 8). The right eye central choroidal thickness decreased by 49% from 241 μm to 123 μm, and fundus depigmentation, poliosis of eyebrows and eyelashes, and skin depigmentation spots were observed.
gp100 is also expressed on normal choroidal melanocytes and is thought to be related to the mechanism of choroidal thinning 8). Regular ophthalmic monitoring is necessary during treatment.
Combination of a Gαq inhibitor (YM-254890) and a MEK inhibitor (trametinib/binimetinib) has shown synergistic antitumor effects in vitro and in vivo 6). While MAPK signaling recovers within 24 hours with Gαq inhibition alone, the combination with a MEK inhibitor suppresses the recovery of MAPK signaling 6).
A phase II trial of selumetinib showed PFS improvement, but a phase III trial of selumetinib plus dacarbazine (SUMIT trial) did not demonstrate PFS improvement 6).
In uveal melanoma, the efficacy of immune checkpoint inhibitors is limited compared to cutaneous melanoma. This is thought to be related to the eye being an immune-privileged organ and the immunosuppressive microenvironment.
Local approaches for metastatic lesions under investigation include liver resection, radiofrequency ablation, hepatic artery embolization, percutaneous hepatic perfusion (PHP) with melphalan, and yttrium-90 microsphere brachytherapy (SIRT).
An autophagy-related 9-gene signature (9-ARG) has been shown to be useful for predicting prognosis in uveal melanoma (validated in 80 TCGA cases + 150 GEO cases)9). In the high-risk group, the IL6-JAK-STAT3 pathway, angiogenesis, and reactive oxygen species pathways are enriched, and the immunosuppressive phenotype is associated with poor prognosis9).
Kujala et al. (2013) reported staging based on anatomical progression of ciliary body and choroidal melanoma using the CIOM T classification, providing a basis for stratifying the relationship between tumor location and prognosis10).
Carter TJ, Rivero Rodriguez S, Fernandez-Trigo N, et al. Uveal melanoma UK national guidelines: 2023 update. Eye (Lond). 2023.
Rantala ES, Hernberg MM, Piperno-Neumann S, Grossniklaus HE, Kivelä TT.. Metastatic uveal melanoma: The final frontier. Prog Retin Eye Res. 2022;90:101041. doi:10.1016/j.preteyeres.2022.101041. PMID:34999237.
Tigari B, Saini M, Manchanda S, Vankdoth S. Large ciliary body melanoma. BMJ case reports. 2021;14(11). doi:10.1136/bcr-2021-246386. PMID:34764100; PMCID:PMC8587378.
Ma J, Roelofs KA, Russell L, Weis E, Chen SH. Rapid growth of primary uveal melanoma following intravitreal bevacizumab injection: a case report and review of the literature. Digital journal of ophthalmology : DJO. 2021;26(3):27-30. doi:10.5693/djo.02.2020.06.001. PMID:33867879; PMCID:PMC8031910.
Nathan P, Hassel JC, Rutkowski P, et al. Overall Survival Benefit with Tebentafusp in Metastatic Uveal Melanoma. N Engl J Med. 2021;385(13):1196-1206. doi:10.1056/nejmoa2103485.
Sriramareddy SN, Smalley KSM. MEK-ing the most of it: strategies to co-target Gαq and MAPK in uveal melanoma. Clin Cancer Res. 2021;27(5):1217-1219. doi:10.1158/1078-0432.CCR-20-4530. PMID:33355300; PMCID:PMC7925419.
Cristina Fonseca, Rita Pinto-Proença, Sabrina Bergeron, Luís Miguel Pires, Júlia Fernandes, Isabel Marques Carreira, et al. Intratumoral Heterogeneity in Uveal Melanoma. Ocul Oncol Pathol. 2020;7(1):17-25. doi:10.1159/000508517.
Krohn J, Vinnem LIH, Jansson RW, Straume O. Fundus hypopigmentation and choroidal thinning associated with tebentafusp therapy: report of a case and literature review. BMC ophthalmology. 2025;25(1):464. doi:10.1186/s12886-025-04274-7. PMID:40817046; PMCID:PMC12357441.
Chuah S, Chew V. Immune implication of an autophagy-related prognostic signature in uveal melanoma. Bioscience reports. 2021;41(8). doi:10.1042/BSR20211098. PMID:34374416; PMCID:PMC8380919.
Kujala E, Damato B, Coupland SE, Desjardins L, Bechrakis NE, Grange JD, Kivelä T.. Staging of ciliary body and choroidal melanomas based on anatomic extent. J Clin Oncol. 2013;31(22):2825-2831. doi:10.1200/jco.2012.45.2771. PMID:23816968.
Jessica C. Hassel, Sophie Piperno-Neumann, Piotr Rutkowski, Jean-Francois Baurain, Max Schlaak, Marcus O. Butler, Ryan J. Sullivan, Reinhard Dummer, et al. Three-Year Overall Survival with Tebentafusp in Metastatic Uveal Melanoma. N Engl J Med. 2023;389(24):2256-2266. doi:10.1056/nejmoa2304753.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.