Persistent fetal vasculature (PFV) is a congenital eye disease caused by incomplete regression of the embryonic hyaloid vascular system. It was formerly called persistent hyperplastic primary vitreous (PHPV). In 1997, Goldberg proposed the term PFV to include residual vascular fibrous tissue around the lens 12), and this term is now widely accepted.
The hyaloid vascular system consists of the hyaloid artery arising from the optic disc and the anterior tunica vasculosa lentis. Mesenchymal cells enter the vitreous cavity through the embryonic fissure around the 5th to 6th week of gestation, reaching their peak at the 10th week. Regression begins peripherally from the 13th to 15th week and is completed in the late fetal period. In PFV, this regression is incomplete, leading to abnormal development of perivascular tissues.
PFV is typically unilateral and non-hereditary, and no specific causative gene has been identified. Classic cases present with leukocoria and microphthalmia, but it may also be diagnosed upon presentation with strabismus or amblyopia.
PFV is reported to be associated with approximately 20% of infantile and childhood cataracts 2)3). In the Pediatric Eye Disease Investigator Group (PEDIG) cataract registry, 64 of 994 cases (6.4%) had PFV-associated cataracts 1); 75% underwent surgery as aphakic (median age at surgery 2 months) and 25% as pseudophakic (median age at surgery 29 months) 1). Posterior segment abnormalities (vitreous, retinal, or optic nerve anomalies) were present in 28% 1), and only 4–6% had a family history 1).
QWhat is the difference between PFV and PHPV?
A
Essentially, they are old and new names for the same disease. PHPV is the older term, focusing on hyperplasia and persistence of the hyaloid artery (primary vitreous). In 1997, Goldberg proposed the term PFV (persistent fetal vasculature) to also include the persistence of fibrovascular tissue around the lens. PFV can represent a broader spectrum of lesions and is now the standard term.
QDoes PFV occur in both eyes?
A
PFV is almost always unilateral and non-hereditary. In the PEDIG study, only 3 cases of bilateral PFV were excluded 1). Bilateral cases require differentiation from familial exudative vitreoretinopathy (FEVR) and Norrie disease, and further examination including genetic testing is recommended.
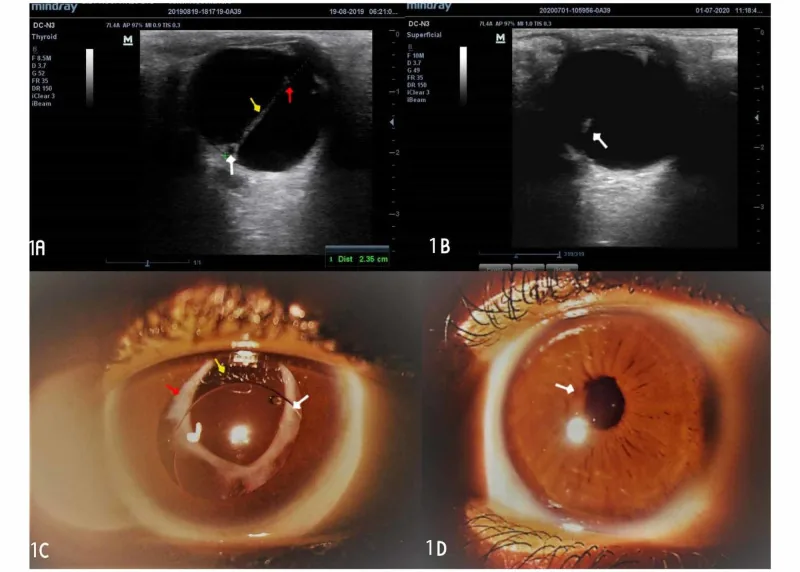
Egbu E The Outcome of Manual Small Incision Cataract Surgery and Anterior Vitrectomy for Persistent Fetal Vasculature in an 18-Year-Old Woman: A One-Year Follow-Up. Cureus. 2020. Figure 1. PMCID: PMC7584328. License: CC BY.
Ocular ultrasound shows a cord-like hyperechoic lesion running through the vitreous, and the anterior segment photograph under mydriasis reveals a white fibrovascular tissue behind the pupil. These findings are characteristic of PFV, showing retrolental fibrovascular membrane and vitreous cord, suitable for the section on main symptoms and clinical findings.
Main findings include microphthalmia in one eye, opacity on the posterior lens surface (Mittendorf dot), abnormal retinal vascular course, retinal dysplasia, elongated ciliary processes, and a stalk extending from the posterior lens surface toward the optic disc. The stalk can cause traction, leading to hypotony via elongation of the ciliary processes. The retina may be involved in the stalk near the optic disc. Severity varies depending on the degree of regression of the hyaloid vascular system.
In the PEDIG study, posterior segment abnormalities were found in 28% (18/64 eyes) of PFV cataracts 1), and 46% of pseudophakic eyes had posterior segment lesions (age-adjusted OR 4.47 compared to 28% in aphakic eyes) 1). Anterior vitrectomy was performed at the time of cataract surgery in 96% of aphakic PFV eyes 1).
In normal development of the hyaloid vascular system, mesenchymal cells enter the vitreous cavity through the embryonic fissure at 5–6 weeks of gestation, forming the hyaloid vascular system. It peaks at 10 weeks of gestation, then regression begins from the periphery. Specifically, regression starts at 13–15 weeks of gestation and subsides in the late fetal period.
In PFV, incomplete regression of the hyaloid vessels occurs, leading to abnormal development of perivascular tissues. This is thought to result in lens opacity, retinal dysplasia, and microphthalmia. Furthermore, traction from the residual tissue causes elongation of ciliary processes and retinal folds.
PFV is considered unilateral and non-hereditary, and no specific causative gene has been identified. Only 4–6% have a family history 1), and most cases are sporadic. In bilateral cases, genetic differentiation from FEVR (NDP, LRP5, FZD4 mutations) and Norrie disease (NDP mutation) is important.
No clear association with low birth weight or prematurity has been shown, but severe persistence of the hyaloid vasculature may rarely present findings similar to retinopathy of prematurity.
Ultrasound (B-scan): Visualizes strands from the posterior lens capsule. Useful for evaluating microphthalmos and the vitreous cavity. Particularly important when the media are opaque and the posterior pole cannot be directly visualized.
CT: Detects intraocular calcification. Retinoblastoma is associated with calcification, while PFV is not, making this the most useful test for differentiating the two diseases.
MRI: Excellent for evaluating strands, posterior segment abnormalities, and optic nerve invasion.
ERG/VEP (Electroretinogram/Visual Evoked Potential): Assesses retinal function. Used preoperatively to evaluate visual function and determine the appropriateness of surgical intervention.
The most important task is to differentiate from diseases that cause leukocoria. In particular, differentiation from retinoblastoma is directly linked to prognosis.
Differentiation from Retinoblastoma
Disease that must be ruled out as a priority
PFV is usually associated with microphthalmos, but retinoblastoma is not. CT detection of intraocular calcification is useful; calcification is characteristic of retinoblastoma and not seen in PFV.
Differentiation from FEVR and Norrie Disease
Important in bilateral cases
In cases of bilateral total retinal detachment or retrolental fibroplasia, differentiation from FEVR or Norrie disease is necessary. Family history and genetic testing are helpful. Use of next-generation sequencing (NGS) panel testing is useful.
Disease
Laterality
Microphthalmos
Hereditary
CT Calcification
Characteristic Findings
PFV
Almost always unilateral
Present
Non-hereditary
None
Retrolental fibrovascular stalk, fibrovascular membrane to optic disc
QWhat is the most important disease to rule out when leukocoria is observed?
A
Retinoblastoma. It is the most common intraocular malignant tumor in children and is directly linked to life prognosis, so prompt exclusion is necessary. PFV is often associated with microphthalmia, while retinoblastoma usually does not present with microphthalmia. CT examination to check for intraocular calcification is the most important differential step. If calcification is confirmed, retinoblastoma should be strongly suspected, and referral to a specialized facility is required.
Opacities of the transparent media are managed similarly to cataracts. If the opacity is localized to the posterior lens and the fundus is normal, lensectomy and fibrovascular membrane removal are performed, following the approach for congenital cataracts. If the retrolental stalk is eccentric and does not involve the visual axis, surgery is not necessarily required. When the fundus is involved, surgery is generally not indicated. For retinal detachment or traction, good ERG/VEP responses provide a basis for surgical intervention. If anterior proliferation causes pupillary distortion or occlusion, pupilloplasty is performed.
After lens removal, refractive correction and amblyopia treatment are performed. The surgical technique follows that for congenital cataracts. In the PEDIG study, 96% of aphakic PFV eyes underwent anterior vitrectomy at the time of cataract surgery 1). The incidence of visual axis opacification was 18% when anterior vitrectomy was performed at the initial surgery, compared to 60% when it was not performed 1).
Postoperatively, amblyopia treatment combining refractive correction (contact lenses or glasses) and occlusion of the healthy eye (eye patch) is performed. In unilateral PFV, compliance with amblyopia treatment determines visual prognosis. Treatment must be actively carried out during the critical period of visual development (from birth to around 10 years of age).
Overall visual outcomes: among 42 eyes, 4 eyes (10%, 95% CI 3–23%) achieved age-normal visual acuity, and 48% (95% CI 32–64%) achieved visual acuity of 20/200 or better 1). The rate of achieving 20/200 or better in pseudophakic PFV eyes (23%) was significantly worse than in non-PFV pseudophakic eyes (68%) (age-adjusted OR=0.14, P=0.005) 1). Aphakic PFV eyes had comparable outcomes to non-PFV aphakic eyes (age-adjusted OR=1.90, P=0.14) 1).
By type, the median visual acuity in anterior-type was 20/100 (54% with 20/200 or better), whereas in posterior-type it was worse at 20/800 (36% with 20/200 or better), a difference of 4 logMAR lines (P=0.09) 1).
Other reports include a 20-year single-center study by Bata et al. (58 aphakic PFV eyes) with 33% achieving 20/200 or better (mean follow-up 6.7 years) 4), a report by Anteby et al. (30 aphakic PFV eyes) with 16.7% achieving 20/200 or better (mean follow-up 8.5 years) 5), and a study by de Saint Sauveur et al. of 36 severe mixed-type PFV cases where measurable visual acuity was present in only 19%, and 61% had no light perception 8).
Other major complications include visual axis opacification (45% in pseudophakic PFV eyes, 15% in aphakic eyes), with a cumulative incidence of visual axis clearing surgery reaching 40% in pseudophakic PFV eyes 1). Additionally, 13% (95% CI 2–22%) of aphakic PFV eyes require secondary IOL implantation within 5 years 1).
There is no effective treatment for retinal dysplasia. In posterior-type PFV, visual development is often not expected. For significant microphthalmos, early prosthetic eye fitting is considered for cosmetic reasons. Prosthetic eye fitting also contributes to orbital development.
QWhat visual acuity can be expected after PFV surgery?
A
In anterior-type (localized posterior lens), the median visual acuity at 5 years postoperatively is 20/100, with 54% achieving 20/200 or better 1). However, only 10% of all eyes achieve age-normal visual acuity. In posterior-type, the median visual acuity is poor at 20/800 1). Visual prognosis is greatly influenced by disease type, presence of posterior segment involvement, age at surgery, and compliance with amblyopia treatment.
QWhat is the most important complication to watch for after PFV surgery?
A
Glaucoma-related adverse events are the most common, reaching a 5-year cumulative incidence of 24% in aphakic PFV eyes 1). Visual axis opacification is also an important complication, occurring in 45% of pseudophakic eyes 1). Performing anterior vitrectomy at the initial surgery is important for preventing visual axis opacification (18% with vs. 60% without) 1). Long-term regular intraocular pressure management, visual axis evaluation, and refractive correction are necessary even after surgery.
At 5–6 weeks of gestation, mesenchymal cells enter the vitreous cavity from the optic fissure, forming the hyaloid vascular system consisting of the hyaloid artery and the tunica vasculosa lentis. This vascular system plays an important role in supplying oxygen and nutrients to the developing lens and anterior segment of the eye.
The peak of development is at 10 weeks of gestation, after which regression begins from the periphery. Regression becomes prominent from 13–15 weeks and is almost complete by the late fetal period. At normal birth, the hyaloid vascular system is barely present, although remnants such as Mittendorf’s dot (a small white spot on the posterior lens surface) may remain.
In PFV, regression failure of the hyaloid vessels occurs, leading to abnormal development of fibrovascular tissue around the vessels. The residual perivascular mesenchymal tissue proliferates and fibroses, presenting various clinical findings.
Specific consequences include the following:
Lens opacity (posterior subcapsular cataract, posterior lenticonus): adhesion of residual fibrous tissue to the posterior lens surface
Microphthalmos: impaired overall ocular growth due to abnormal development of perivascular tissue
Retinal dysplasia: retinal malformation due to traction and ischemia in the posterior type
Elongation of ciliary processes and hypotony: traction by fibrous bands
Retinal fold: deformation due to traction by posterior pathological tissue
The reason for unilaterality and non-heredity is thought to be that the regression of hyaloid vessels during the embryonic period is controlled by local angiogenesis and regression signals, and impairment of this control mechanism is assumed to occur in only one eye. However, the specific molecular mechanisms remain unknown.
Although specific causative genes for PFV have not been identified, animal models have reported that mutations in Wnt signaling pathway-related genes such as FZD4, LRP5, and NDP show PFV-like phenotypes (persistent hyaloid vasculature). These are also causative genes for FEVR and Norrie disease, suggesting a genetic continuum between PFV and related disorders. Clinical application of next-generation sequencing (NGS) panel testing for differential diagnosis of PFV is also advancing.
Approaches using 25-gauge and 27-gauge microincision vitreous surgery (MIVS) for posterior PFV are being attempted. Small-incision surgery in neonates and infants is said to have advantages in minimizing invasiveness and reducing postoperative inflammation 11).
Comparison of long-term outcomes between primary IOL implantation in infancy versus secondary IOL implantation after aphakic management is an important issue in PFV research. Extended follow-up data from the PEDIG study are expected to establish IOL implantation criteria specific to PFV 6)7).
Noninvasive evaluation of PFV using wide-field fundus cameras and anterior segment OCT is advancing. In particular, anterior segment OCT is useful for morphological assessment of posterior lenticonus and posterior subcapsular cataract, as well as for preoperative planning.
Haider KM, Repka MX, Sutherland DR, Hatt SR, Fallaha N, Kraker RT, et al. Outcomes and Complications 5 Years After Surgery for Pediatric Cataract Associated With Persistent Fetal Vasculature. American journal of ophthalmology. 2024;260:30-36. doi:10.1016/j.ajo.2023.11.002. PMID:37939986; PMCID:PMC11005992.
Wilson ME, Trivedi RH, Morrison DG, Lambert SR, Buckley EG, Plager DA, et al. The Infant Aphakia Treatment Study: evaluation of cataract morphology in eyes with monocular cataracts. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2011;15(5):421-6. doi:10.1016/j.jaapos.2011.05.016. PMID:22108352; PMCID:PMC3345197.
Solebo AL, Russell-Eggitt I, Cumberland P, Rahi JS. Congenital cataract associated with persistent fetal vasculature: findings from IoLunder2. Eye (London, England). 2016;30(9):1204-9. doi:10.1038/eye.2016.159. PMID:27472205; PMCID:PMC5023809.
Bata BM, Chiu HH, Mireskandari K, Ali A, Lam WC, Wan MJ. Long-term visual and anatomic outcomes following early surgery for persistent fetal vasculature: a single-center, 20-year review. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2019;23(6):327.e1-327.e5. doi:10.1016/j.jaapos.2019.07.009. PMID:31629823.
Anteby I, Cohen E, Karshai I, BenEzra D. Unilateral persistent hyperplastic primary vitreous: course and outcome. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2002;6(2):92-9. doi:10.1067/mpa.2002.121324. PMID:11997805.
Repka MX, Dean TW, Lazar EL, Yen KG, Lenhart PD, Freedman SF, et al. Cataract Surgery in Children from Birth to Less than 13 Years of Age: Baseline Characteristics of the Cohort. Ophthalmology. 2016;123(12):2462-2473. doi:10.1016/j.ophtha.2016.09.003. PMID:27769584; PMCID:PMC5121052.
Repka MX, Dean TW, Kraker RT, Li Z, Yen KG, de Alba Campomanes AG, Young MP, Rahmani B, et al. Visual Acuity and Ophthalmic Outcomes 5 Years After Cataract Surgery Among Children Younger Than 13 Years. JAMA ophthalmology. 2022;140(3):269-276. doi:10.1001/jamaophthalmol.2021.6176. PMID:35142808; PMCID:PMC8832311.
de Saint Sauveur G, Chapron T, Abdelmassih Y, Chehaibou I, Lecler A, Dureau P, et al. Management and Outcomes of Posterior Persistent Fetal Vasculature. Ophthalmology. 2023;130(8):844-853. doi:10.1016/j.ophtha.2023.03.027. PMID:37044159.
Khandwala N, Besirli C, Bohnsack BL.. Outcomes and surgical management of persistent fetal vasculature. BMJ Open Ophthalmol. 2021;6(1):e000656. doi:10.1136/bmjophth-2020-000656. PMID:34013048; PMCID:PMC8094357.
Hunt A, Rowe N, Lam A, Martin F.. Outcomes in persistent hyperplastic primary vitreous. Br J Ophthalmol. 2005;89(7):859-863. doi:10.1136/bjo.2004.053595. PMID:15965167; PMCID:PMC1772745.
Bata BM, Khalili S, Ali A, Wan MJ, Mireskandari K. Late surgery for unilateral persistent fetal vasculature: long-term visual and anatomic outcomes. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2022;26(6):296.e1-296.e5. doi:10.1016/j.jaapos.2022.09.005. PMID:36265751.
Goldberg MF. Persistent fetal vasculature (PFV): an integrated interpretation of signs and symptoms associated with persistent hyperplastic primary vitreous (PHPV). LIV Edward Jackson Memorial Lecture. American journal of ophthalmology. 1997;124(5):587-626. doi:10.1016/s0002-9394(14)70899-2. PMID:9372715.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.