Diffuse Unilateral Subacute Neuroretinitis (DUSN) is a multifocal chorioretinitis caused by a nematode migrating in the subretinal space. It was first reported by Gass et al. in 1978 and was initially called “unilateral wipeout syndrome” 3). It commonly occurs in healthy children and young adults 1), and is typically unilateral, although bilateral cases have been reported 3).
Several causative nematodes are known, classified by the size of the worm and the presumed endemic region.
Worm species
Body length (approximate)
Main endemic regions
Baylisascaris procyonis
1500–2000 μm
Midwestern United States, North America
Toxocara canis
400–1000 μm
Southeastern United States, tropical regions
Ancylostoma caninum
400–1000 μm
Tropical/subtropical
Gnathostoma spinigerum
400–1000 μm
Asia (Thailand, etc.)
Endemic areas are widespread, including the Midwest and Southeast of the United States, Brazil, Caribbean islands, India, and Malaysia. In Malaysia, the prevalence of soil-transmitted helminths (STH) is reported to reach 52–76% 4).
QCan DUSN occur in both eyes?
A
Although typically unilateral, bilateral cases have been reported 3). Delayed treatment in one eye or the patient’s immune status may lead to involvement of the fellow eye. However, simultaneous bilateral onset is rare, and if findings in one eye are asymmetric to the other, a detailed examination considering DUSN is necessary.
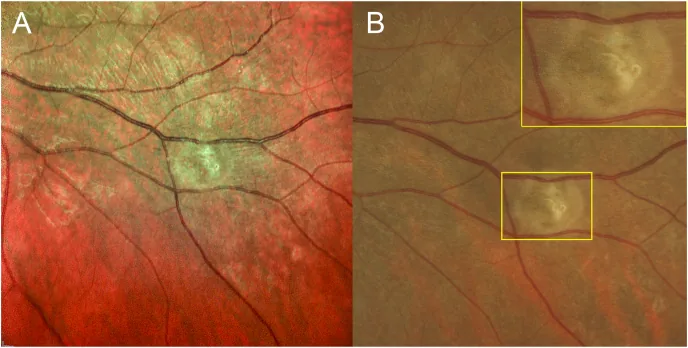
Simrat K Sodhi; John Golding; Efrem D Mandelcorn; Andrea K Boggild; Netan Choudhry. Enface vitreous OCT ‘worm holes’: A novel finding in a patient with diffuse unilateral subacute neuroretinitis (DUSN). Am J Ophthalmol Case Rep. 2021 May 12; 23:101112. Figure 4. PMCID: PMC8170075. License: CC BY.
(A) MultiColor scanning laser imaging and (B) color fundus photograph of the left eye post-laser treatment demonstrating early laser burn with centrally locating nematode corpse. Magnified inset corresponds to area demarcated in yellow. (For interpretation of the references to color in this figure legend, the reader is referred to the Web version of this article.)
The route of infection for DUSN is primarily through contact with host animals or exposure to contaminated environments.
Contact with host animal feces: Feces of raccoons (the definitive host of B. procyonis) can be a source of infection3).
Ingestion of contaminated food: Consumption of undercooked meat or seafood. Cases have been reported with a history of travel to Thailand2) and consumption of street food in Pakistan3).
Outdoor activities: Exposure to soil and animal feces during camping or outdoor work1).
Age: More common in young people under 40 years old. In those aged 20 and older, early consultation within one month is associated with better final visual acuity1).
Travel or residence in endemic areas: A history of living in the aforementioned endemic areas is a risk factor.
QWho is more likely to get DUSN?
A
It commonly occurs in healthy children and young adults, but can also develop without any specific underlying disease 1). Risk factors include travel or residence in endemic areas (Midwest and Southeast United States, Brazil, tropical regions of Asia), contact with wild animals such as raccoons, and consumption of undercooked food.
Definitive diagnosis requires direct visualization of the nematode in the fundus, but this is possible in only about 25–39% of all cases1). Comparison of serial fundus photographs to confirm the worm’s movement pattern is useful1).
Increased autofluorescence around the optic disc and macula1)
Enface swept-source vitreous OCT reveals cavities “wormholes” at the internal limiting membrane (ILM) level along the migration path of the nematode, which were first reported as traces of the nematode moving into the vitreous 3). Infrared live imaging can track the worm in real time using 900 nm near-infrared mode, utilizing the nematode’s photophobic behavior (avoidance of visible light 450–490 nm) 2).
Blood tests: Eosinophilia is a supportive finding 1)4).
Serological tests: Antibody tests for Toxocara and B. procyonis2). If cat scratch disease (CSD) coinfection is suspected, also test for Bartonella henselae antibodies 4).
QHow is the diagnosis made when the nematode cannot be identified?
A
The nematode can be directly visualized in only about 25–39% of cases1). When not visible, diagnosis is made clinically based on a combination of unilateral multifocal white dot lesions, optic neuritis, vitritis, eosinophilia, travel history to endemic areas, and animal contact. It is recommended to attempt detection of the nematode using multimodal imaging such as infrared live imaging and en face OCT.
Treatment for DUSN differs depending on whether the nematode is visible. Combination therapy with laser photocoagulation, oral albendazole, and systemic steroids is associated with the best prognosis1).
This is the first-line treatment when the nematode is visible1).
Standard parameters: spot size 200 μm, power 150–200 mW, duration 0.2 seconds1).
Navigated laser (Navilas 577s): spot 100 μm, power 400 mW, duration 20 ms, delivered in a 4×4 pattern2).
Infrared live imaging assistance: The photophobic nematode is observed under near-infrared mode to determine the irradiation site in real time2). Since the nematode exhibits avoidance behavior when exposed to blue light (450–490 nm), a technique has been developed to use infrared mode until just before irradiation and then switch immediately before delivery3).
The standard dosage and duration of albendazole have not been established1)2), but several regimens have been reported.
Dosing Regimen
Notes
400 mg/day × 30 days
Standard simple regimen2)
400 mg twice/day × 30 days
High-dose regimen2)
200 mg × 2/day × 6 weeks
Divided dose1)
400 mg × 2/day × 6 weeks
High dose, long term1)
400 mg/day × 6 weeks
Single dose, long term4)
In eyes with vitritis, albendazole shows improved intraocular penetration due to disruption of the blood-retinal barrier (BRB), leading to higher therapeutic efficacy1).
Steroids (corticosteroids): For inflammation control, prednisone 40–60 mg/day is tapered over 2–4 weeks (e.g., schedule: 30 mg → 20 mg → 10 mg → 5 mg)2).
Treatment for coexisting infection: For cases complicated by CSD, doxycycline 100 mg twice daily for 6 weeks4). For secondary ocular hypertension, timolol, brimonidine, and acetazolamide are used4).
Laser Photocoagulation
Indication: When the nematode is directly visible in the fundus.
Principle: Irradiate immediately after visualization. Surround the nematode from 1–2 DD behind its location.
Purpose: Suppression of vitreitis, vasculitis, and optic neuritis.
QDoes vision recover after laser treatment?
A
If laser photocoagulation is performed early, visual recovery can be expected. However, in late-stage cases with optic atrophy or extensive RPE degeneration, irreversible visual impairment remains1). Early consultation within one month in patients aged 20 years or older has been shown to be associated with better final visual acuity1), highlighting the importance of early intervention.
6. Pathophysiology and Detailed Mechanism of Onset
Retinal damage in DUSN is caused by a combination of local mechanical and toxic stimuli from the nematode migrating in the subretinal space and the host immune response (inflammatory reaction). This mechanism is described as “toxic autoimmune nematode retinopathy”1).
The nematode initially migrates confined to the subretinal space but may also move into the vitreous cavity. “Wormholes” observed on enface swept-source vitreous OCT have been reported as cavities representing traces of nematode migration within the vitreous3), suggesting that B. procyonis may randomly migrate through all layers of the retina3).
The timeline of the pathology is as follows.
Early stage: Local inflammation occurs along the path of the worm, appearing as gray-white subretinal lesions (cluster-like white spots). Vitreitis and papillitis progress simultaneously.
Intermediate stage: Subretinal tracks form, with accumulating damage to the RPE and outer photoreceptors. Diffuse RPE degeneration spreads.
Late stage: Optic atrophy and narrowing of retinal arterioles occur, with a marked decrease in ERG b-wave amplitude. These changes are irreversible1), and since the worm can survive intraocularly for up to 3 years, delayed diagnosis critically worsens the final prognosis.
QWhat is the mechanism of vision loss in DUSN?
A
Both toxins produced by the worm and the host immune response cause retinal damage1). In the early stage, only reversible photoreceptor dysfunction occurs, but in the late stage, optic atrophy, diffuse RPE degeneration, and retinal arteriolar narrowing progress, leading to irreversible vision loss. Therefore, the longer the worm remains in the eye, the worse the visual prognosis.
7. Latest Research and Future Perspectives (Research-stage Reports)
Hänsli et al. (2024) performed real-time tracking of a nematode using infrared live imaging (900 nm) and administered navigated laser photocoagulation (Navilas 577s) in a 14-year-old boy (best corrected visual acuity 20/100) who developed DUSN after traveling to Thailand2).
By combining nematode visualization in infrared mode immediately before laser irradiation with a 4×4 pattern (100 μm, 400 mW, 20 ms, 41 spots), photocoagulation was accurately completed while suppressing the photophobic nematode’s avoidance behavior2). After treatment, albendazole (400 mg/day × 30 days) and prednisone (30 mg → tapered) were added, and serum Toxocara antibody positivity was confirmed.
Sodhi et al. (2021) performed enface swept-source vitreous OCT in a 37-year-old woman (best corrected visual acuityCF, vitreous cells 1+) with DUSN and recorded for the first time worldwide a cavity (“wormhole”) at the ILM level corresponding to the nematode’s migration path3).
Conventional tomographic OCT confirmed nematodes at the ILM level, but enface vitreous OCT images continuously depicted the migration path itself as a cavity 3). This finding is evidence that the nematode had invaded the vitreous and supports the hypothesis that B. procyonis randomly migrates through the full thickness of the retina.
In the same case, using MultiColor scanning laser imaging (green reflectance 515 nm, blue reflectance 488 nm) revealed the entire image of the nematode, which is difficult to see on white-light fundus photographs 3). These multimodal approaches are expected to contribute to improved diagnostic rates in cases where the nematode is not directly visible 1)2)3).
Nurul-Farhana M, Roslin-Azni AA, Sor-Earn T, Shatriah I, Shelina OM. Diffuse Unilateral Subacute Neuroretinitis: Challenges in Diagnosis and Management. Cureus. 2024;16(4):e58510. doi:10.7759/cureus.58510. PMID:38765355; PMCID:PMC11101984.
Christof Hänsli, Cornelia Staehelin, Alexandra Bograd, Christoph Tappeiner. Infrared live imaging and navigated laser for nematode photocoagulation in a child with diffuse unilateral subacute neuroretinitis (DUSN). American Journal of Ophthalmology Case Reports. 2024;36:102102. doi:10.1016/j.ajoc.2024.102102.
Sodhi SK, Golding J, Mandelcorn ED, Boggild S, Choudhry N. Enface vitreous OCT ‘worm holes’: A novel finding in a patient with diffuse unilateral subacute neuroretinitis (DUSN). Am J Ophthalmol Case Rep. 2021;23:101112. doi:10.1016/j.ajoc.2021.101112.
Siti-Khadijah AR, Azhany Y, Norwazilah MA, Nor-Azita AT. Presumed DUSN and cat-scratch disease: dual infection in a single patient. Taiwan J Ophthalmol. 2022;12(3):349-353.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.