Cat scratch disease (CSD) is a zoonotic infection caused by the gram-negative bacterium Bartonella henselae (B. henselae). First described by Debré in 19503), it is known as the most common cause of Parinaud oculoglandular syndrome.
The main route of infection is scratches or bites from infected cats. The cat flea (Ctenocephalides felis) transmits B. henselae between cats, and flea feces on claws infect humans when a cat scratches2). One to two weeks after a scratch or bite, a skin lesion (red papule) appears at the infection site, followed 1–2 weeks later by swelling and tenderness of the regional lymph nodes.
In the United States, the incidence in children under 15 years of age is approximately 4.7 per 100,000 person-years1). It is more common in children and young adults, with a peak in autumn and winter3). More than 90% of cases resolve spontaneously, but ocular complications occur in 5–15% of cases4).
Main Ocular Complications of Cat Scratch Disease
Neuroretinitis: Most common. Optic disc edema + macular star.
Source of infection: Scratch or bite from an infected cat. Kittens under 1 year old have a higher risk of bacteremia2)
Common age group: Children to young adults
Seasonality: More common in autumn to winter3)
QCan you get infected just by owning a cat?
A
Usually, direct contact such as being scratched or bitten by a cat is necessary. However, recent studies have reported that B. henselae can stably exist in various biological and non-biological liquids, suggesting the possibility of infection through indirect contact3). Infected cats themselves are often asymptomatic, and it is important to always check for a history of contact with kittens during the interview.
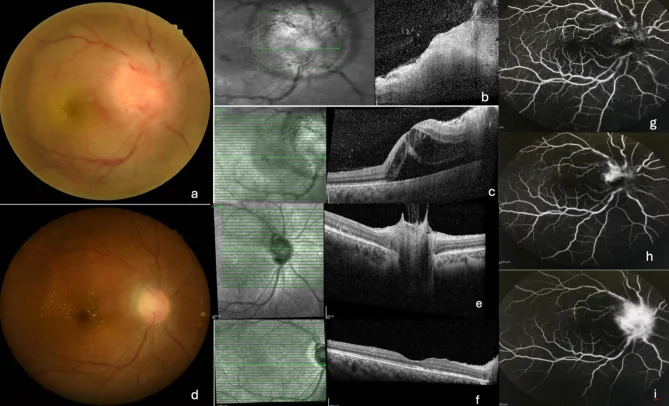
Rajan RS, et al. Clinical and imaging characteristics of neuroretinitis secondary to cat scratch disease from tertiary centers in Malaysia: a retrospective study. J Ophthalmic Inflamm Infect. 2025. Figure 1. PMCID: PMC12748332. License: CC BY.
The fundus photograph shows marked swelling of the optic disc and radial hard exudates in the macula, indicating neuroretinitis associated with cat scratch disease. OCT shows fluid accumulation from the peripapillary area to the macula, and fluorescein angiography confirms leakage from the optic disc lesion.
One to two weeks after being scratched by a cat, a skin lesion (red papule) appears at the infection site. One to two weeks later, swelling and tenderness of the regional lymph nodes occur. Fever and general malaise may accompany.
Unilateral vision loss and blurred vision (central visual field defect)
Headache and fever (may appear as prodromal symptoms 1))
Eye pain is usually absent (painless vision loss) 1)
In a 21-year-old female case, the chief complaint was painless blurred vision in the left eye, and central visual field defect was confirmed on Amsler grid 1).
Characteristics of macular star (stellate macular exudates):
Optic papillitis → fluid diffusion to peripapillary retina → radial deposition of lipid and fibrin exudates in the macula, forming a star-shaped pattern. The exudates align along the Henle fiber layer, resulting in a characteristic stellate appearance on fundus examination. It is visible on fundus examination 10–14 days after injury.
In fluorescein angiography, leakage from the optic disc is a characteristic finding of neuroretinitis. Fluid diffusion to the peripapillary retina and accumulation of exudates in the macula originate from this leakage. In cases of retinal periphlebitis, leakage from the venous wall is observed4).
Findings of retinal periphlebitis:
Segmental retinal venous sheathing
Perivenous retinitis
Fluorescein leakage from the venous wall on angiography4)
In recurrent cases, perivenous retinochoroidal atrophy may eventually remain4).
Encephalitis (central nervous system complication):
Neurological involvement occurs in approximately 2% of all cat scratch disease cases5)
Main symptoms: seizures, impaired consciousness, headache
Diagnosis: IgG antibody titer ≥1:64 with a fourfold or greater change5)
Some cases have residual sequelae (cognitive dysfunction, spastic paraplegia)5)
Ocular complications of cat scratch disease involve the following factors.
Risk factors
Details
History of cat contact
Kittens under 1 year old have a particularly high risk of bacteremia2)
Flea infestation
Flea infestation in cats is an independent risk factor for developing cat scratch disease2)
Immune status
Immunocompromised individuals have an increased risk of severe/disseminated bartonellosis (bacillary angiomatosis)3)
Season
Autumn to winter (overlap of kitten breeding season and flea activity period)3)
Age
Common in children and young adults, but older adults have a higher risk of endocarditis8)
B. henselae is transmitted among cats via the feces of cat fleas (C. felis). Infected cats are often in an asymptomatic bacteremic state and transmit the infection to humans through scratches or bites. Scratches, bites, or flea bites from infected cats are the main mechanisms of infection 2).
QWhat should be done for the cat itself?
A
Infected cats are often asymptomatic. However, treating cats can reduce B. henselae bacteremia and lower the risk of transmission to humans. Flea control is the most important intervention, and administration of doxycycline plus a fluoroquinolone antibiotic to cats (4–6 weeks) is recommended 2). A One Health approach involving collaboration among physicians, veterinarians, and pet owners is ideal 2).
Diagnosis is based on a combination of history of cat contact (especially with kittens), clinical symptoms, and serological testing. A history of redness and swelling at the wound site approximately 10 days after injury is key to diagnosis.
Serological testing:
Measurement of Bartonella henselae IgM/IgG (indirect fluorescent antibody test/ELISA)
IgG antibody titer ≥1:64 is diagnostically significant5)
A four-fold or greater change between acute and convalescent phases is useful for definitive diagnosis5)
Case reports have recorded IgG 1:512 and IgM 1:321)
Erythrocyte sedimentation rate (ESR), CRP, and syphilis serology are also measured for differential diagnosis
Warthin-Starry staining (tissue diagnosis):
Silver staining of conjunctival scrapings or lymph node biopsy specimens
Small bacilli stain brown to black
A diagnostic method with high specificity but not high sensitivity7)
Can also be visualized with Steiner stain or Dieterle stain3)
Fundus examination:
Confirmation of optic disc edema and macular star
Stellate exudate pattern on fundus photography1)
Basic examination that can directly confirm the triad of neuroretinitis
In the differential diagnosis of neuroretinitis, idiopathic Leber stellate neuroretinopathy (self-limiting type) and syphilis are important differential diseases. Cat scratch disease-related cases are typically unilateral1). History of cat contact and presence of lymphadenopathy are key points for differentiation, and it is essential to inquire about contact with kittens during the interview9).
Generally, the prognosis is good, and both systemic and ocular lesions often heal spontaneously within 1–2 months. For mild cases, observation for several weeks is the basic approach. Antibiotics are administered if the condition persists 10).
In a case of a 32-year-old man with B. henselae-associated bilateral segmental retinal periphlebitis, doxycycline monotherapy (100 mg twice daily) was administered twice but resulted in relapse. Eventually, a combination of doxycycline and rifampicin (100 mg twice daily and 300 mg twice daily, respectively) was continued for 3 months, with no recurrence for 8 years thereafter 4).
B. henselae is a facultative intracellular bacterium capable of infecting various cell types, including vascular endothelial cells, endothelial progenitor cells, epithelial cells, red blood cells, and monocytes/macrophages 4). This endotheliotropic property is the root cause of diverse ocular symptoms 4).
Stages of infection4):
After skin inoculation, a non-bacteremic phase in the primary niche (local granuloma formation → lymphadenopathy)
Dissemination into the bloodstream, infection of red blood cells (enabling vector transmission)
Tissue infection: hematogenous spread to the eye (retina, optic nerve), causing various ocular symptoms
Mechanism of Parinaud oculoglandular syndrome:
Bartonella directly invades through the conjunctiva, causing granulomatous inflammation in regional lymph nodes (preauricular, parotid, cervical, submandibular). B. henselae in conjunctival scraping specimens can be confirmed by Warthin-Starry silver stain.
Mechanism of neuroretinitis:
Optic disc edema (papillitis) → fluid diffusion to the peripapillary retina → macular star formation (lipid and fibrin exudates). Fluorescein angiography shows leakage from the optic disc6). Immune-mediated inflammation is thought to be involved in this process. Exudates align along the Henle fiber layer, forming a stellate pattern.
Mechanism of encephalitis:
Cat scratch disease-associated encephalitis is thought to involve two mechanisms: direct brain infection and para-infectious autoinflammation 5). In the para-infectious mechanism, high concentrations of IL-6 and IgG production in CSF have been confirmed 5).
Prognosis:
In optic neuritis and neuroretinitis, visual loss may be prolonged, but recovery occurs in most cases. Star-shaped maculopathy has a good visual prognosis, and hard exudates resolve over several months. However, even with a tendency toward spontaneous remission, permanent visual impairment due to sequelae of macular lesions can occur, with varying severity.
7. Latest Research and Future Perspectives (Research-stage Reports)
Association between COVID-19 and Cat Scratch Disease:
Cases have been reported where latent B. henselae infection was reactivated after COVID-19 infection. A 54-year-old man developed rapid enlargement of a mass and pleural effusion triggered by COVID-19 infection, and B. henselae was identified by NGS. Improvement was seen after switching to doxycycline plus azithromycin 3).
Diagnostic Application of Next-Generation Sequencing (NGS):
NGS is attracting attention as a technology that overcomes the limitations of conventional serological tests and PCR methods (cross-reactivity, difficulty distinguishing infection from past exposure). NGS provides species identification and quantitative data of pathogens, useful for monitoring infection severity 3).
One Health approach: To eradicate cat scratch disease, a One Health approach involving collaboration among physicians, veterinarians, pet owners, and public health officials has been proposed. Flea control and treatment in cats can directly reduce the risk of B. henselae infection in humans 2).
Use of ocular ultrasound: Measurement of optic nerve sheath diameter using point-of-care ultrasound (POCUS) in the emergency department is a promising adjunct tool for early detection of optic disc edema even when fundoscopy is difficult. It may lead to early diagnosis and treatment of neuroretinitis1).
Long-term management of recurrent ocular bartonellosis: In cases of recurrent ocular bartonellosis resistant to single-agent antibiotics, long-term combination therapy with doxycycline and rifampin (≥3 months) has been shown effective in case reports. Good long-term outcomes with no recurrence over 8 years of follow-up have also been reported 4).
Expanding spectrum of ocular bartonellosis: The range of ocular manifestations of Bartonella infection extends beyond neuroretinitis and Parinaud syndrome to include retinochoroiditis, orbital cellulitis, optic neuritis, and endophthalmitis-like conditions 8). In immunocompromised patients, progression to multi-organ infection (bacillary angiomatosis) is a concern.
QWill vision recover?
A
Neuroretinitis in immunocompetent patients has a good prognosis. With appropriate antibiotic therapy, visual recovery can be expected in most cases 9). In a case of a 21-year-old woman, complete recovery to corrected visual acuity of 20/20 was achieved 3 months after initial presentation 1). However, in recurrent retinal periphlebitis, long-term paravenous retinochoroidal atrophy may persist 4). In cases complicated by encephalitis, neurological sequelae may remain 5). Although spontaneous remission tends to occur, macular sequelae may persist, and the degree varies.
Avaylon J, Lau K, Harter K, Mamoor A, Mehendale R, Ranasinghe L, Durant E, Bains G.. Neuroretinitis as a Complication of Cat Scratch Disease. Cureus. 2023;15(9):e45866. doi:10.7759/cureus.45866. PMID:37885521; PMCID:PMC10599218.
Okrent Smolar AL, Chow CA, Dhoot DS, et al. Cat scratch disease: What to do with the cat. Vet Dermatol. 2022;33(5):475-e141.
Dong Y, Alhaskawi A, Zou X, Zhou H, Ezzi SHA, Kota VG, Abdulla MHAH, Olga A, Abdalbary SA, Lu H.. Post-COVID reactivation of latent Bartonella henselae infection: a case report and literature review. BMC Infect Dis. 2024;24(1):422. doi:10.1186/s12879-024-09336-7. PMID:38649899; PMCID:PMC11034019.
Ng CC, Ng J, McDonald HR, Cunningham ET Jr. Bartonella henselae-associated recurrent, bilateral segmental periphlebitis. American journal of ophthalmology case reports. 2022;26:101475. doi:10.1016/j.ajoc.2022.101475. PMID:35321248; PMCID:PMC8935419.
Nakamura M, Ura S, Yabe I, Otsuki M, Soma H, Ogata A.. Cat Scratch Disease-associated Encephalitis Followed by Parkinsonism. Intern Med. 2022;61(20):3115-3120. doi:10.2169/internalmedicine.9047-21. PMID:35314550; PMCID:PMC9646356.
Ksiaa I, Abroug N, Mahmoud A, Zina S, Hedayatfar A, Attia S, Khochtali S, Khairallah M.. Update on Bartonella neuroretinitis. J Curr Ophthalmol. 2019;31(3):254-261. doi:10.1016/j.joco.2019.03.005. PMID:31528758; PMCID:PMC6742623.
Carithers HA.. Cat-scratch disease. An overview based on a study of 1,200 patients. Am J Dis Child. 1985;139(11):1124-1133. doi:10.1001/archpedi.1985.02140130062031. PMID:4061408.
Florin TA, Zaoutis TE, Zaoutis LB.. Beyond cat scratch disease: widening spectrum of Bartonella henselae infection. Pediatrics. 2008;121(5):e1413-25. doi:10.1542/peds.2007-1897. PMID:18443019.
Habot-Wilner Z, Trivizki O, Goldstein M, Kesler A, Shulman S, Horowitz J, Amer R, David R, Ben-Arie-Weintrob Y, Bakshi E, Almog Y, Sartani G, Vishnevskia-Dai V, Kramer M, Bar A, Kehat R, Ephros M, Giladi M.. Cat-scratch disease: ocular manifestations and treatment outcome. Acta Ophthalmol. 2018;96(4):e524-e532. doi:10.1111/aos.13684. PMID:29504674.