Endophthalmitis is a general term for purulent inflammation characterized by massive infiltration of inflammatory cells into the intraocular fluids, including the vitreous cavity and anterior chamber. It progresses rapidly, and if appropriate treatment is delayed, it can lead to irreversible visual impairment within a short period, making it a representative ophthalmic emergency.
Based on the route of onset, it is broadly classified into two types: exogenous and endogenous.
Exogenous Endophthalmitis
Acute postoperative type: Most common after cataract surgery. Onset occurs within 6 weeks postoperatively.
Delayed-onset (chronic postoperative) type: Onset occurs weeks to months or more after surgery. Caused by organisms such as P. acnes.
Traumatic: Pathogens directly enter through a perforating wound of the eyeball. Incidence rate is 0.9–18% in adults and 5–54% in children. 2)
Filtering bleb-associated and after intravitreal injection: The incidence after anti-VEGF administration is increasing.
Endogenous Endophthalmitis
Bacterial: Complicates 0.04–0.5% of bacteremia cases. 1) Hematogenous dissemination from other organ infections such as lung, liver, and endocarditis.
Fungal: Candida species are common, and it tends to occur in immunocompromised patients or those with long-term central venous catheterization.
K. pneumoniae-associated: In a 12-year dataset from Taiwan, it accounts for 55.8% of EE. 1) Closely associated with diabetes and liver abscess.
Endogenous endophthalmitis (EE) occurs in 0.04–0.5% of bacteremia cases 1), and in cases of liver abscess (PLA) due to hypervirulent K. pneumoniae (hvKP), the incidence of EE reaches 3.4–12.6%. 3)
QDoes endophthalmitis only occur after cataract surgery?
A
Cataract surgery is the most common cause, but there are various exogenous routes such as trauma, intravitreal injection of anti-VEGF drugs, and bleb-associated infections. Additionally, endogenous endophthalmitis occurs when systemic infections spread to the eye via the bloodstream, requiring special attention in diabetic and immunocompromised patients.
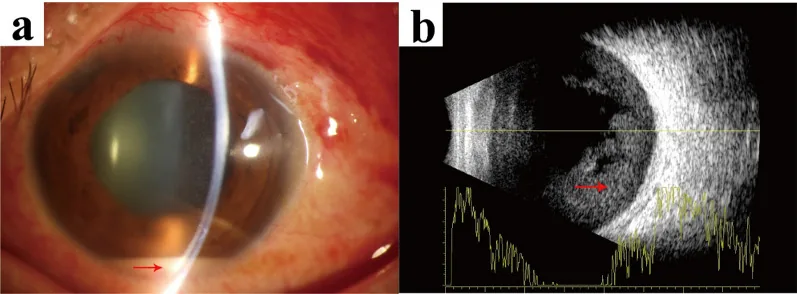
Xiaojie Lu; Bei Liu; Tiemei Yie; Weiwei Wang. Endophthalmitis caused by Abiotrophia defectiva with initial presentation as retinal vasculitis: a case report. J Med Case Rep. 2025 Jul 11; 19:336. Figure 2. PMCID: PMC12247376. License: CC BY.
Images were obtained following the patient’s hospitalization. a: Slit lamp examination revealed a 1.5-mm hypopyon (red arrow showing hypopyon). b: A brightness scan ultrasound confirmed dense vitreous opacities (red arrow showing vitreous opacity)
Decreased vision: The most common initial complaint reported by patients. 5)
Eye pain: Present in 74% of EVS cases, but approximately 25% or more of cases have no pain. Endophthalmitis should not be ruled out based solely on the presence or absence of pain.
Redness and photophobia: Appear early as acute signs of inflammation. 5)
Floaters: Visual symptoms due to inflammatory cell infiltration into the vitreous. 5)
QDoes endophthalmitis always cause pain?
A
According to EVS data, eye pain is present in 74% of cases, but more than 25% of patients have no pain. If sudden vision loss or redness occurs after surgery or injection, endophthalmitis should be actively suspected and evaluated even without pain.
In a multicenter study of 610 eyes, infection with highly virulent bacteria had an odds ratio of 4.48 for severe vision loss (LP or worse) and 1.90 for retinal detachment or enucleation.4)
Poor prognostic factors:
Low visual acuity at presentation (light perception or worse)
After glaucoma surgery or trauma (due to conjunctival barrier disruption) 4)
Diabetes: EE risk increases 3.6–11 times. In EE with hvKP liver abscess, diabetes is present in 68.3% 1)
HbA1c >9%: Associated with increased risk of invasive infection 3)
QHow often does endophthalmitis occur after cataract surgery?
A
Postoperative endophthalmitis after cataract surgery is rare but serious. ESCRS recommends intracameral antibiotic administration at the end of surgery to reduce the risk of postoperative endophthalmitis 8).
Assessment of visual acuity at the time of presentation is most important for determining treatment strategy. Based on EVS findings, the distinction between light perception (LP) or worse and hand motion (HM) or better is a decision point for treatment selection (see “Standard Treatment” section).
When the fundus is difficult to visualize due to vitritis or corneal edema, this examination is essential for evaluating intravitreal echoes and confirming the presence or absence of retinal detachment.
Vitreous specimen: Has a higher positivity rate than aqueous humor. In the EVS, the positivity rate of aqueous humor is only 4.2%, making vitreous puncture the key to diagnosis.
Culture positivity rate: In a multicenter study, 296 of 610 eyes (48.5%) were positive. 4)
mNGS (metagenomic next-generation sequencing): Useful for identifying rare pathogens that are difficult to culture (e.g., Paenibacillus species). 2)
In early postoperative anterior chamber inflammation, differentiation from TASS is important. 5)
TASS: Rapid onset within 12–24 hours after surgery, no vitritis, responds to steroid eye drops
Postoperative endophthalmitis: Usually onset 2–7 days after surgery, with vitreous opacity, requires antibiotic treatment
QHow to distinguish endophthalmitis from TASS?
A
TASS develops the day after surgery (within 12–24 hours) and does not involve vitritis, which is a key differentiating point from endophthalmitis. 5)TASS responds to steroid eye drops, whereas early administration of antibiotics is essential for endophthalmitis; distinguishing between the two directly affects treatment strategy. If in doubt, vitreous aspiration for specimen collection should be performed.
Indication: Cases with visual acuity of hand motion (HM) or better at presentation.
Procedure: Perform vitreous tap and intravitreal antibiotic injection.
In the EVS, for patients with visual acuity of hand motion or better, there was no significant difference in final visual acuity between immediate vitrectomy and tap & inject. Therefore, tap & inject is the first choice as a less invasive treatment.
Immediate Vitrectomy
Indication: Cases with light perception (LP) or worse visual acuity at presentation.
Outcome: The proportion achieving visual acuity of 20/40 or better was 33% in the vitrectomy group and 11% in the tap group. 5)
Immediate vitrectomy removes causative organisms and inflammatory substances from the vitreous. In Japan, many facilities perform early vitrectomy to improve visual prognosis.
The ESCRS guidelines (2024) recommend the following:8)
Intracameral cefuroxime: ESCRS recommends intracameral antibiotic administration at the end of cataract surgery.8)
Preoperative and postoperative antibiotic eye drops are an adjunctive measure to reduce ocular surface bacterial load, but their additional benefit over intracameral antibiotics is not clear.9)10)
Standardization of infection prevention measures including intracameral antibiotics is central to preventing postoperative endophthalmitis.8)
Management of systemic infection is the top priority. IDSA recommends administering antibiotics for 4 to 6 weeks for endogenous endophthalmitis (EE) associated with K. pneumoniae liver abscess (PLA). 1) Ocular local treatment (intravitreal antibiotic injection and vitrectomy) is performed concurrently with systemic treatment.
QHow is endogenous endophthalmitis treated?
A
Standard treatment involves local ocular therapy with vitrectomy and intravitreal antibiotic injection, combined with systemic antibiotic therapy for the underlying disease (e.g., liver abscess, bacteremia) continued for 4 to 6 weeks. 1) Management of underlying conditions such as diabetes and immunosuppression should be performed concurrently, and collaboration with an infectious disease specialist is essential.
During surgery or trauma, commensal bacteria from the periocular area enter the eye and rapidly proliferate in the immunologically isolated vitreous cavity and anterior chamber. Because the intraocular environment lacks defense mechanisms against organisms such as staphylococci, even a small number of bacteria can establish infection.
Highly virulent bacteria are relatively more common after glaucoma surgery and vitrectomy, likely because these procedures disrupt the conjunctival barrier, facilitating the entry of oral commensals and environmental bacteria. 4)
Pathogens are hematogenously disseminated into the eye from infectious foci in other organs (e.g., liver abscess, pneumonia, endocarditis). Infection typically begins in the posterior segment through retinal vessels and spreads to the uvea and vitreous.
Virulence factors of hvKP (hypervirulent K. pneumoniae):
Capsular polysaccharide (CPS): Confers resistance to phagocytosis. Forms the mucoid colony (hypermucoviscosity) characteristic of hvKP. 1)3)
Lipopolysaccharide (LPS): Activates the inflammatory cascade.
Siderophores (iron acquisition systems): Promote growth by scavenging iron from the host.
Virulence genes:peg-344, iutA, rmpA, etc., are associated with hypervirulence. 1)3)
In diabetes, hyperglycemia-induced increased vascular permeability promotes the invasion of hvKP into retinal blood vessels 3), and impaired neutrophil function weakens infection defense. This is considered one of the reasons for the high frequency of PLA-associated EE in diabetic patients.
Yap et al. (2025) reported in a multicenter study of 610 eyes that endophthalmitis caused by highly virulent bacteria (e.g., oral bacteria, Streptococcus) had an odds ratio of 4.48 for severe vision loss (LP or worse) and 1.90 for retinal detachment or enucleation compared to low-virulence bacteria. 4) The culture positivity rate was 48.5% (296/610 eyes). This finding indicates that estimating the causative organism at the time of presentation (based on surgical procedure, injury mechanism, and clinical course) contributes to prognosis prediction.
Endophthalmitis after anti-VEGF injection: Large-scale analysis using the IRIS Registry
A study using the IRIS Registry (2025) reported that in 1044 cases of endophthalmitis after intravitreal anti-VEGF injection, there was no significant difference in final visual acuity between early vitrectomy and intravitreal antibiotic injection alone. 6) This suggests that tap and inject may avoid excessive invasiveness in cases with good presenting visual acuity.
Timing of post-traumatic globe closure and endophthalmitis
Blanch et al. (Ophthalmology) conducted a systematic review including 8497 eyes comparing early versus delayed primary closure in open globe injuries and examined the impact on endophthalmitis incidence. 7) Early closure is recommended to prevent pathogen entry into the eye and reduce infection risk.
Lu et al. (2025) reported a case of systemic infection and endophthalmitis caused by Paenibacillus species, a rare bacterium difficult to identify by culture, which was identified using mNGS (metagenomic next-generation sequencing).2) mNGS is attracting attention as a promising technique for investigating the cause of culture-negative endophthalmitis.
Chen Y, Gong Y, Song B, Du Y, Cai K. Pyogenic liver abscess complicated with endogenous endophthalmitis caused by Klebsiella pneumoniae: A case report and Literature Review. Immunity, inflammation and disease. 2023;11(7):e943. doi:10.1002/iid3.943. PMID:37506152; PMCID:PMC10373569.
Lu S, Li H, Ma C, Li X. Systemic and localized infections in humans caused by Paenibacillus: a case report and literature review. BMC ophthalmology. 2025;25(1):133. doi:10.1186/s12886-025-03966-4. PMID:40087598; PMCID:PMC11907811.
Liu J, Dai M, Sun Q, Fang W. A typical multisite invasive infection caused by hvKP: A case report and literature review. Medicine. 2022;101(52):e32592. doi:10.1097/MD.0000000000032592. PMID:36595971; PMCID:PMC9803426.
Yap A, Kaur D, Muttaiyah S, et al. Impact of microorganism virulence on endophthalmitis outcomes. Br J Ophthalmol. 2025;109(3):347-352. doi:10.1136/bjo-2024-325605. PMID:39299710.
American Academy of Ophthalmology. Cataract in the Adult Eye Preferred Practice Pattern. Ophthalmology. 2022;129(1):S64-S164.
Early Vitrectomy vs Injection Only for Endophthalmitis After Anti-VEGF Injections. Ophthalmology. 2025.
Blanch RJ, et al. Early versus Delayed Timing of Primary Repair after Open Globe Injury. Ophthalmology.
Passaro ML, Posarelli M, Avolio FC, Ferrara M, Costagliola C, Semeraro F, et al. Evaluating the efficacy of postoperative topical antibiotics in cataract surgery: A systematic review and meta-analysis. Acta Ophthalmol. 2025;103(6):622-633. PMID: 40018950.
Matsuura K, Miyazaki D, Inoue Y, Sasaki Y, Shimizu Y. Comparison of iodine compounds and levofloxacin as postoperative instillation; conjunctival bacterial flora and antimicrobial susceptibility following cataract surgery. Jpn J Ophthalmol. 2024;68(6):702-708. PMID: 39240403.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.