The vitreous is a transparent tissue without blood vessels, so bleeding from adjacent tissues spreading into the vitreous gel causes vitreous hemorrhage. Traumatic vitreous hemorrhage is bleeding into the vitreous due to blunt, penetrating, or perforating ocular trauma, leading to sudden vision loss and floaters after injury.
The overall incidence of vitreous hemorrhage (including spontaneous cases) is reported to be about 7 per 100,000 population per year. By cause, proliferative diabetic retinopathy, posterior vitreous detachment, and trauma account for 59–88.5% of all cases. 4) In particular, trauma is the most common cause in young people under 40 years of age.
ICD-10 code: S05 (Injury of eye and orbit)
Closed globe injury (blunt trauma)
Mechanism: Anteroposterior compression of the globe causes equatorial expansion, exerting inward traction on retinal vessels. This leads to rupture of retinal vessels, retinal tears, or retinal dialysis, resulting in vitreous hemorrhage.
Features: Common in blunt trauma (sports injuries, traffic accidents, assaults). In young patients, strong vitreoretinal adhesion leads to greater tractional changes.
Open globe injury (penetrating/perforating trauma)
Mechanism: Full-thickness defect of the ocular wall can cause bleeding throughout the intraocular layers. Vitreous prolapse (incarceration) may occur.
Features: May involve retained intraocular foreign bodies (metal fragments, glass pieces). High risk of endophthalmitis, requiring early surgical intervention.
Fresh bleeding appears red, but over time it changes from yellowish-white to grayish-white, making it difficult to distinguish from old vitreous opacities.
The following associated findings specific to trauma should be confirmed:
Hyphema (blood accumulation in the anterior chamber): Blood may accumulate in the anterior chamber even if the fundus is visible.
Iridodialysis or lens damage: These complications are common in blunt trauma.
Perforating wound or scleral rupture: In open globe injuries, check for a wound on the anterior surface of the eye.
Rubeosis iridis (neovascularization of the iris): Seen in chronic or long-standing cases.
QIs vitreous hemorrhage after trauma always painful?
A
Vitreous hemorrhage itself is usually painless, but it is often accompanied by periorbital pain, hyphema, or iritis due to trauma. Open globe injuries are associated with severe ocular pain. Regardless of the presence or absence of pain, if sudden vision loss or floaters occur, prompt ophthalmologic evaluation is necessary.
Since the vitreous body is an avascular tissue without blood vessels, direct damage to adjacent tissues (retinal vessels, ciliary body, choroid) or indirect traction forces become the source of vitreous hemorrhage.
In young people, the adhesion between the vitreous and retina is stronger than in adults, so traction changes during blunt trauma are greater, and retinal dialysis is more likely to occur.
In infants with bilateral vitreous hemorrhage, head trauma due to abuse should be considered. Do not judge solely by ocular findings; evaluate the consistency of systemic findings and mechanism of injury with pediatrics and emergency medicine. 3)
QWhat should be particularly noted in children with vitreous hemorrhage?
A
If bilateral vitreous hemorrhage is observed in an infant, head trauma due to abuse should be considered. 3) In children, the adhesion between the vitreous and retina is strong, and traction changes are greater than in adults. Additionally, retinopathy of prematurity, Coats disease, and retinoblastoma are important differential diagnoses, and referral to a specialist should be considered.
Age: Under 40 years, trauma is the most common cause. In the elderly, hemorrhage associated with posterior vitreous detachment is common.
Sports and occupational environment: High risk in racquetball, boxing, martial arts, metalworking, etc.
Pre-existing eye diseases: Lattice degeneration of the retina makes traumatic retinal tears more likely.
Anticoagulants and antiplatelet drugs: They may increase bleeding, but if medically necessary, stopping them to resolve vitreous hemorrhage is not recommended. 1)
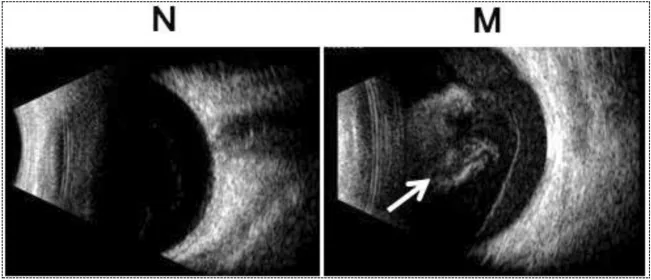
Yan W, He Q, Chen M, et al. SSFVEP as a potential electrophysiological examination for evaluating visual function of fundus diseases with vitreous hemorrhages: a clinical study. Sci Rep. 2024;14(1):2378. Figure 1. PMID: 38287026; PMCID: PMC10825178; DOI: 10.1038/s41598-023-47714-4. License: CC BY.
In the normal eye (N, left), a uniform dark area is seen in the vitreous cavity, whereas in the vitreous hemorrhage eye (M, right), high-intensity echoes (opacities due to vitreous hemorrhage) indicated by white arrows are visualized within the vitreous cavity. This corresponds to the B-mode ultrasound findings of vitreous hemorrhage discussed in section “4. Diagnosis and Examination Methods.”
Traumatic vitreous hemorrhage is a clinical finding, so it is important to quickly assess the extent of bleeding, presence of retinal detachment, and presence of intraocular foreign bodies.
Obtain detailed information on the mechanism of trauma (blunt or penetrating), time of injury, and course of visual changes. Check for history of retinal disease, lattice degeneration, diabetes, etc. In children, if the mechanism of injury and clinical findings are inconsistent, consider abuse.
Slit-lamp examination: Identify red blood cells in the anterior vitreous, check for pigment epithelial cells, inflammatory cells, hyphema, iris dialysis, lens dislocation/damage, and rubeosis iridis.
Dilated fundus examination: Check the morphology and extent of hemorrhage, and the presence of retinal tears or retinal detachment. In open-globe injuries, first evaluate the wound with tonometry and slit-lamp examination, and carefully consider dilated scleral depression.
When blood is aggregated on the posterior hyaloid membrane, it may be difficult to differentiate from detached retina. If continuity with the optic disc is confirmed, detached retina is more likely.
B-scan ultrasonography can yield false negatives, so detailed fundus examination after hemorrhage resolution is important.
In open-globe injuries, check for globe deformation and intraocular foreign bodies (hyperechoic spots).
The following shows the main uses of each examination.
Treatment strategy varies depending on the severity of bleeding, presence of retinal detachment, and type of trauma. Delayed treatment can lead to permanent retinal damage or neovascular glaucoma due to ischemia, so careful consideration is needed between conservative observation and surgical treatment.
If bleeding is mild, natural absorption is awaited while continuing observation. Red blood cells disappear at a rate of about 1% per day. Complete absorption may take several weeks to months.
Rest and head positioning: Instruct to keep the head elevated while sleeping. This allows blood to settle, improving vision and enabling a more complete fundus examination.
Restriction of strenuous activities: Avoid heavy lifting, strong straining, and contact sports.
Indications for Vitrectomy (Pars Plana Vitrectomy: PPV)
Vitrectomy after trauma is generally performed after acute inflammation subsides (usually a waiting period of 2–4 weeks). However, early surgery is prioritized in the following cases:
During the waiting period, inflammation management (steroid eye drops, anti-inflammatory drugs) and intraocular pressure management are performed concurrently.
Weeks to months after trauma, degenerated (ghost) red blood cells remaining in the vitreous can obstruct the trabecular meshwork (the eye’s drainage structure), leading to elevated intraocular pressure, a condition known as ghost cell glaucoma.
Diagnosis: Brownish degenerated red blood cells (ghost cells) are observed in the anterior chamber using a slit lamp microscope.
Treatment: Administer intraocular pressure-lowering medications (beta-blocker eye drops, carbonic anhydrase inhibitors). If medical treatment is ineffective, consider vitrectomy for removal.
If chronic hemorrhage or ischemic changes progress, new blood vessels may form in the iris and angle, leading to neovascular glaucoma. Treatment delay is the greatest risk, so even during follow-up observation, regular gonioscopy and intraocular pressure management are important.
QHow long does it take for vitreous hemorrhage to be absorbed?
A
Red blood cells are thought to disappear at a rate of about 1% per day, and complete absorption may take several weeks to months. Elevating the head during sleep allows blood to settle, which may improve daytime vision. If absorption does not occur, if retinal detachment is present, or if there is a risk of neovascular glaucoma, vitrectomy is indicated.
The vitreous is a transparent tissue without blood vessels, so hemorrhage spreads from adjacent tissues (retinal vessels, choroid, ciliary body). In traumatic cases, the mechanisms are broadly divided into direct damage from mechanical force and traction.
When the eye is compressed anteroposteriorly, the equator expands in the coronal plane, generating inward traction from the vitreous to the retina. Especially in young patients, the adhesion between the vitreous and retina is strong, so this traction can cause retinal dialysis, retinal vessel rupture, and vitreous hemorrhage.
When a full-thickness defect occurs in the eyewall, intraocular pressure drops sharply, and full-layer hemorrhage can occur in the choroid, ciliary body, and vitreous cavity. Vitreous prolapse (incarceration) may cause retinal traction.
In abusive head trauma, multilayered intraocular hemorrhage may occur, including preretinal, intraretinal, subretinal, and vitreous cavity hemorrhage. Findings should be evaluated together with the mechanism of injury and systemic damage. 3)
Blood released into the vitreous cavity rapidly forms a clot and clears at a rate of approximately 1% per day. Red blood cells are either eliminated through the trabecular meshwork, undergo hemolysis and phagocytosis, or remain in the vitreous for several months.
Degenerated (ghost) red blood cells can obstruct the trabecular meshwork, causing ghost cell glaucoma. Additionally, red blood cell components in the vitreous may stimulate fibrous proliferation, leading to proliferative vitreoretinopathy.
Evidence regarding the optimal timing of surgery for traumatic vitreous hemorrhage is limited. Tan et al. (2010) reported a retrospective case series of 40 eyes with vitreous hemorrhage and retinal tears undergoing early vitrectomy, showing favorable outcomes and acceptable complication rates 5). Further prospective studies are needed to evaluate the efficacy of early intervention in traumatic cases.
Application of Small-Incision Vitrectomy (25G, 27G) in Traumatic Eyes
25-gauge and 27-gauge microincision vitrectomy surgery (MIVS) is less invasive even in eyes with residual post-traumatic inflammation and is expected to promote early postoperative recovery. Reports on safety and efficacy in traumatic eyes are accumulating.
Based on the hemorrhage-reducing effect of preoperative anti-VEGF agents observed in proliferative diabetic retinopathy, attempts are being made to apply this to tractional lesions after trauma. However, rapid contraction of neovascular membranes may worsen tractional retinal detachment, and careful patient selection is necessary for use in traumatic eyes. 1)
Lim JI, Kim SJ, Bailey ST, et al. Diabetic Retinopathy Preferred Practice Pattern. Ophthalmology. 2025 Apr;132(4):P75-P162. doi:10.1016/j.ophtha.2024.12.020. PMID:39918521.
Kim SJ, Bailey ST, Kovach JL, Lim JI, Vemulakonda GA, Ying GS, et al. Posterior Vitreous Detachment, Retinal Breaks, and Lattice Degeneration Preferred Practice Pattern®. Ophthalmology. 2025;132(4):P163-P196. doi:10.1016/j.ophtha.2024.12.023. PMID:39918519.
Christian CW, Block R; Committee on Child Abuse and Neglect, American Academy of Pediatrics. Abusive head trauma in infants and children. Pediatrics. 2009;123(5):1409-1411. doi:10.1542/peds.2009-0408.
Tan HS, Mura M, Bijl HM. Early vitrectomy for vitreous hemorrhage associated with retinal tears. Am J Ophthalmol. 2010;150:529-533. PMID: 20579632. doi:10.1016/j.ajo.2010.04.005.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.