Anterior Segment Developmental Anomalies (ASDA) is a general term for developmental disorders related to the anterior segment of the eye—the cornea, iris, lens, and anterior chamber. It is also called Anterior Segment Dysgenesis (ASD).
ASDA includes the following representative disease entities.
These diseases are diverse in both phenotype and genotype, and more than 50 genes have been found to be involved. Although genetic knowledge continues to expand through exome analysis and whole genome analysis, the causative gene has not been identified in 40–75% of cases. Cases that cannot be classified into a specific phenotype are described as “unclassified ASD.” 1)
Aqueous humor produced by the ciliary body of the iris is drained through the trabecular meshwork into Schlemm’s canal and via the uveoscleral outflow pathway. In ASDA, this process is often impaired, and secondary glaucoma is a common and important complication.
If only posterior embryotoxon is present without systemic symptoms, it is treated separately from ARS based on the 9th Consensus Report of the World Glaucoma Association. 1)
QAt what age is anterior segment developmental anomaly (ASDA) typically diagnosed?
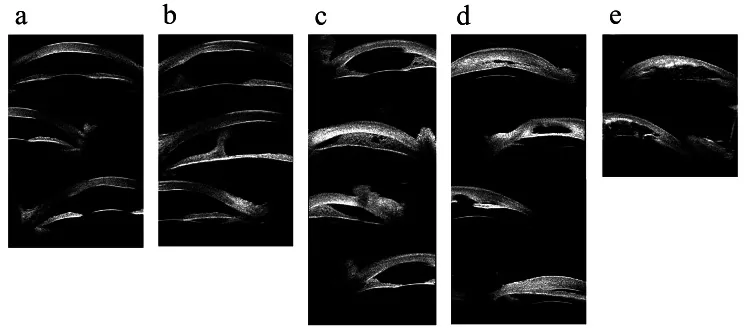
Hong J, et al. Classifications of anterior segment structure of congenital corneal opacity in infants and toddlers by ultrasound biomicroscopy and slit-lamp microscopic photographs: an observational study. BMC Ophthalmol. 2024. Figure 1. PMCID: PMC10804776. License: CC BY.
(a) Corneal opacity, (b) Corneal opacity with central anterior synechia, (c) Peripheral iridocorneal adhesion ≤180 degrees, (d) Peripheral iridocorneal adhesion >180 degrees, (e) Ultrasound biomicroscopy image of corneal opacity with iris and lens abnormalities. These correspond to anterior segment adhesions and corneal opacities discussed in the section “2. Main Symptoms and Clinical Findings”.
In older children and adults, late-onset cases may present with blurred vision or decreased visual acuity from a relatively young age. When intraocular pressure is very high, symptoms such as eye strain or headache may occur. In aniridia, patients may complain of photophobia (day blindness).
Buphthalmos (enlarged corneal diameter) and corneal opacity are often discovered by parents, prompting a visit to the doctor.
ASDA presents characteristic findings depending on the disease. The main findings of representative disease entities are shown below.
Posterior Embryotoxon / ARS
Posterior embryotoxon (PE): An anteriorly displaced and thickened Schwalbe’s line. Observed as a gray-white concentric line on the inner side of the corneal limbus under slit-lamp microscopy.
Axenfeld anomaly: Posterior embryotoxon with iris strands adherent to the peripheral cornea.
Rieger anomaly: In addition to the above, presents with corectopia, ectropion uveae, and pseudopolycoria due to iris stromal hypoplasia. Autosomal dominant inheritance. Glaucoma develops in 50–60% of cases.
Peters anomaly
Central corneal opacity: Essential diagnostic finding. Reflects defects in the corneal endothelium, Descemet’s membrane, and corneal stroma.
Type 1: Posterior corneal defect and corneal opacity only.
Type 2: Accompanied by iris adhesions.
Type 3: Accompanied by anterior lens displacement and cataracts. Approximately 80% are bilateral. Glaucoma is associated in 50–70% of cases.
Aniridia
Iris hypoplasia: Primarily a defect of the posterior iris. May be accompanied by macular hypoplasia, optic nerve hypoplasia, and glaucoma.
Aniridia-associated keratopathy (AAK): Reported incidence ranges from 20% to over 80%. It is a progressive corneal opacity due to limbal stem cell deficiency (LSCD) that progresses throughout life. 2)
WAGR syndrome: Occurs when PAX6 and the adjacent WT1 gene are mutated. Includes Wilms tumor, aniridia, genitourinary abnormalities, and intellectual disability. 3)
Corneal abnormality type
Megalocornea: Corneal diameter ≥13 mm (≥12 mm in newborns). Intraocular pressure and endothelial cell density are usually normal. Often X-linked recessive inheritance.
Sclerocornea: Opaque scleral tissue invades the peripheral cornea. The border between sclera and cornea is indistinct and accompanied by vascular invasion.
CHED: Bilateral symmetric corneal edema appears at birth to 1–2 years of age. Not associated with elevated intraocular pressure. Autosomal recessive.
Findings that may be added when secondary glaucoma is complicated are shown below.
Elevated intraocular pressure: May present with high intraocular pressure (approximately 30–50 mmHg).
Increased corneal diameter (buphthalmos): Due to distension of the ocular coat. If the diameter exceeds 12.0 mm immediately after birth, congenital glaucoma should be suspected.
Haab striae: Permanent linear opacities remaining at the site of Descemet’s membrane rupture.
Optic disc cupping enlargement: In infants, a cup-to-disc ratio of 0.3 or more suggests glaucoma. A difference of 0.2 or more between eyes is also suspicious.
QWhat percentage of patients with Axenfeld-Rieger syndrome develop glaucoma?
A
Glaucoma develops in 50–60% (some reports 50–75%) of cases, which is a high frequency. 3) It follows an autosomal dominant inheritance pattern. Cases with systemic findings (dental anomalies, facial bone anomalies, pituitary anomalies, etc.) are called Rieger syndrome. Glaucoma screening of relatives is recommended.
The main cause of ASDA is genetic abnormalities, with different genes and inheritance patterns involved depending on the disease. The causative genes for major diseases are shown below.
In addition, developmental glaucoma associated with gene abnormalities such as PAX6, PITX2, and FOXC1 has also been reported. The correlation between genotype and phenotype is diverse, and even within families with the same gene abnormality, the phenotype may differ.
Most cases of early-onset developmental glaucoma (primary congenital glaucoma) are sporadic, but about 10% follow an autosomal recessive inheritance pattern. A multifactorial inheritance theory also exists.
Neural crest cells play a central role in anterior segment formation. Trabecular meshwork cells are derived from the neural crest, while the juxtacanalicular connective tissue is derived from vascular endothelial cells. The greatest resistance to aqueous humor outflow exists at the junction of these tissues of different origins. ARS, Peters anomaly, and congenital irisectropion syndrome are all classified as congenital anomalies resulting from abnormal migration of neural crest cells.
A large-scale study in Korea showed that increased maternal exposure to PM2.5 (fine particulate matter) during the three months before conception and during the first and second trimesters of pregnancy was associated with an increased risk of ASDA in offspring.
Slit-lamp microscopy: Evaluates the degree and location of corneal opacity, presence of Haab striae, anterior chamber depth, iris abnormalities (posterior embryotoxon, iris attachment to Schwalbe line), and lens abnormalities. Checks for posterior embryotoxon, iris abnormalities (ARS), and cataract (Peters anomaly).
Intraocular pressure measurement: Goldmann applanation tonometry is standard, but portable tonometers such as rebound tonometer (iCare) or electronic tonometer (Tono-Pen) are useful in children. Note that intraocular pressure decreases under general anesthesia. Measurements are not interchangeable between different tonometers.
Corneal diameter measurement: Measures horizontal and vertical diameters with calipers. Normal range in newborns is 9.5–10.5 mm. If it exceeds 12.0 mm immediately after birth, congenital glaucoma is suspected.
Gonioscopy: Uses a handheld slit lamp and direct gonioscope such as Koeppe lens. Evaluates high iris insertion, iris attachment to Schwalbe line (ARS finding), and increased trabecular meshwork width.
Fundus examination: Observation of optic disc cupping. In infants, a cup-to-disc ratio of 0.3 or more suggests glaucoma. Reduction of cupping after lowering intraocular pressure indicates good pressure control.
Ultrasound biomicroscopy (UBM): Useful when corneal opacity makes gonioscopy difficult. It helps assess the degree of angle dysgenesis and predict the prognosis of outflow reconstruction surgery.
Anterior segment OCT (AS-OCT): As an adjunct, it noninvasively evaluates angle and corneal structures, but does not replace gonioscopy for diagnosis. 3)
Visual field testing: Essential for diagnosing glaucomatous optic neuropathy in children. In children under 5 years, it is difficult even for experienced examiners; kinetic perimetry is easier to perform.
According to the 4th edition of the Japan Glaucoma Society Guidelines for Glaucoma, childhood glaucoma is diagnosed when two or more of the following criteria are met.
Intraocular pressure > 21 mmHg
Progressive increase in cup-to-disc ratio, cup-to-disc ratio asymmetry ≥ 0.2, rim thinning
Corneal findings: Haab striae, or in neonates corneal diameter ≥ 11 mm, in infants under 1 year ≥ 12 mm, in all ages ≥ 13 mm
Progression of myopia due to axial elongation beyond normal development
Reproducible visual field defect consistent with glaucomatous optic neuropathy
Forceps delivery trauma: Unilateral, vertical or oblique linear opacities.
Congenital metabolic diseases such as mucopolysaccharidosis and cystinuria: Evaluation of systemic symptoms is important for differential diagnosis.
Disease groups included in ASD (Axenfeld-Rieger anomaly, Peters anomaly, aniridia, posterior polymorphous dystrophy, microphthalmia, microcornea, etc.) need to be considered in the differential diagnosis. 3)
QDoes posterior embryotoxon alone cause glaucoma?
A
Isolated posterior embryotoxon (without systemic symptoms) is distinguished from ARS, but it is also one of the associated findings of ARS. Posterior embryotoxon can also be observed in healthy eyes and does not necessarily indicate a risk of glaucoma. However, when associated with other diseases such as Alagille syndrome, intraocular pressure monitoring is necessary.
Pharmacotherapy is adjunctive therapy aimed at short-term intraocular pressure reduction before surgery and postoperative pressure control. Drug selection is generally the same as for adult open-angle glaucoma. However, beta-blockers require caution for bronchial asthma and bradycardia, and apnea has been reported in neonates. Oral acetazolamide (5–10 mg/kg every 6–8 hours) is also possible.
Early-onset developmental glaucoma is a disease that fundamentally requires surgical therapy. Pharmacotherapy is adjunctive.
Goniotomy: Suitable as initial surgery for cases with minimal corneal opacity. It has the advantage of not invading the conjunctiva. Using a Barkan lens or Swan-Jacob lens, the trabecular meshwork surface is scraped with a goniotomy knife.
Trabeculotomy: Can be performed regardless of corneal opacity. It is also performed as an additional surgery when goniotomy is insufficiently effective.
Trabeculectomy/Tube shunt surgery: Options when angle surgery is ineffective. In ARS, angle surgery is chosen if the angle is open and the trabecular meshwork coverage by peripheral anterior synechiae is not extensive, but the success rate is lower than in PCG. In cases where angle surgery is ineffective, trabeculectomy or plate-tube shunt surgery may be the first choice. 4)
In Peters anomaly, treatment follows that for PCG, but good postoperative intraocular pressure is achieved in only about one-third of surgical cases, and many have poor prognosis. Due to corneal abnormalities, achieving useful vision is often difficult. 4)
Peters anomaly: In mild cases, corneal opacity often gradually decreases. If intraocular pressure is normal, some improvement is common, and because the outcome of corneal transplantation is poor, corneal transplantation is usually not performed in early childhood. Many cases are refractory to glaucoma medication and outflow reconstruction surgery, with poor prognosis.
CHED: Corneal transplantation (including endothelial transplantation) may be indicated for corneal endothelial dysfunction.
Sclerocornea: May be associated with other ASD syndromes; severe cases may be candidates for corneal transplantation.
Even if intraocular pressure decreases, amblyopia treatment is often necessary. Since anisometropia, irregular astigmatism, corneal opacity, and Haab’s striae can cause amblyopia, visual acuity and refraction tests should be continued in parallel with intraocular pressure measurements. Progression of myopia and elongation of axial length suggest glaucoma progression, so regular measurements are required.
Normal anterior segment formation follows a complex developmental program. At the beginning of the third week of gestation, the optic sulcus forms in the neural plate, marking the start of visual organ development. At the end of the third week, the optic vesicle forms, and at the fourth week, the optic cup forms. Closure of the fetal fissure begins around the sixth week and is completed by the seventh week. The mesenchyme covering the anterior surface of the lens separates to form the anterior chamber.
Neural crest cells undergo epithelial-to-mesenchymal transition and migrate to various locations within the eye. Trabecular meshwork cells are derived from the neural crest, while the juxtacanalicular connective tissue is derived from vascular endothelial cells. This difference in origin forms the site of greatest resistance to aqueous humor outflow.
PITX2: A transcription factor. Located on chromosome 4 (4q25). Associated with both ocular and auditory symptoms in Axenfeld-Rieger syndrome.
FOXC1: A transcription factor. Located on chromosome 6 (6p25). Involved in Axenfeld-Rieger syndrome and associated with both ocular and auditory symptoms, similar to PITX2.
Secondary glaucoma in ASDA primarily results from maldevelopment of the aqueous humor outflow pathway. Specifically, the following factors are involved in combination.
Immature development of the trabecular meshwork: The juxtacanalicular connective tissue is abnormally thick, with excessive accumulation of extracellular matrix.
Attachment of the ciliary body to the trabecular meshwork: Contraction of the ciliary muscle pulls the scleral spur forward, compressing Schlemm’s canal and the trabecular meshwork.
High insertion of the iris root: The iris root is located at the trabecular meshwork, obstructing aqueous humor outflow.
Hypoplasia or absence of Schlemm’s canal.
ICE syndrome has a different etiology from other ASDA. A viral etiology involving herpes simplex virus (HSV) in corneal endothelial cell degeneration has been proposed but not confirmed. It is acquired, occurs in middle-aged adults (slightly more common in women), and is usually unilateral, which also differs from other ASDA.
Pathophysiology of Aniridia-Associated Keratopathy (AAK)
Patients with aniridia develop progressive corneal opacification throughout life. Limbal stem cell deficiency (LSCD) is considered the main mechanism. Multiple studies with confirmed PAX6 mutations have documented this progressive change. The incidence is reported to be 20–80% or more, and it often appears symmetrically but not always. 2)
Exome analysis and whole-genome analysis are advancing the identification of novel associated genes. However, the causative gene remains unidentified in 40–75% of cases, and analysis of the remaining “unexplained cases” is an important future challenge. Elucidation of the correlation between genotype and clinical phenotype is expected to lead to applications in personalized medicine.
In cases with FOXC1 and PITX2 mutations, the onset age and clinical features of glaucoma vary. While genotype may be associated with phenotypic diversity, even the same genetic mutation can present with different disease types, making diagnosis and prognosis prediction difficult. 1)
The incidence of aniridia-associated keratopathy (AAK) is reported to be 20–80% or higher, and multiple studies with confirmed PAX6 mutations have documented the progression of corneal opacification over a lifetime. Research on corneal limbal stem cell transplantation targeting LCSD is advancing, but it is still at the research stage and has not yet been established as a standard treatment. 2)
Epidemiological studies have shown an association between exposure to air pollution (PM2.5) before fertilization and during pregnancy and the risk of ASDA, and public health applications are being explored from the perspective of environmental preventive medicine. This may lead to future prevention strategies.
Application of Minimally Invasive Surgical Devices
The application of micropulse lasers and minimally invasive glaucoma surgery (MIGS) devices to children with ASDA is under research. Long-term outcome data are limited, and efficacy and safety equivalent to those in adult glaucoma have not been established.
Knight LSW, Ruddle JB, Taranath DA, et al. Childhood and Early Onset Glaucoma Classification and Genetic Profile in a Large Australasian Disease Registry. Ophthalmology. 2021;128(11):1549-1560. doi:10.1016/j.ophtha.2021.04.016.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.