Sclerocornea is a rare congenital disease in which abnormal migration of neural crest cells prevents normal formation of the limbal anlage, causing the cornea to become white and opaque like the sclera. It is non-progressive, bilateral, and asymmetric. It is unrelated to inflammatory or infectious causes, and there is no sex predilection.
Corneal opacity is white with vascular invasion, and the limbal border becomes indistinct. In Europe, it is often called cornea plana, while in the United States, it is commonly referred to as sclerocornea.
Complicated by anterior segment abnormalities such as iridocorneal adhesions
Total type
Diffuse opacity of the entire cornea
50% of cases show autosomal dominant (AD) or autosomal recessive (AR) inheritance. The remaining 50% occur sporadically.
QWhat is the relationship with cornea plana?
A
In sclerocornea, the peripheral cornea becomes scleralized, leading to corneal flattening, so cornea plana is frequently associated. Cornea plana is clinically classified into two genetic forms: CNA1 (autosomal dominant, 12q) and CNA2 (autosomal recessive, KERA gene mutation). CNA2 involves more severe corneal flattening and multiple anterior segment abnormalities.
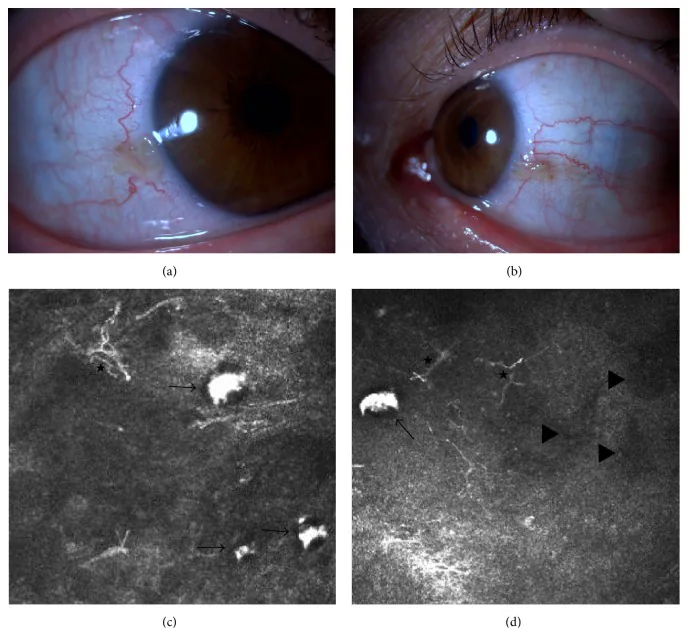
Biler ED, Yilmaz SG, Palamar M, et al. In Vivo Confocal Microscopy and Anterior Segment Optic Coherence Tomography Findings in Ocular Ochronosis. Case Reports in Ophthalmological Medicine. 2015 Dec 15; 2015:592847. Figure 3. PMCID: PMC4693010. License: CC BY.
The anterior segment photograph shows continuous opacification from the corneal periphery, and the microscopic image shows disruption of the superficial structure. The limbus becomes indistinct, and the border between the cornea and sclera appears continuous.
Corneal opacity: Scleral-like white opacity from the periphery toward the center. In the total type, it involves the entire cornea, but the central opacity density is slightly lower. In the partial type, the central area may be clear.
Loss of corneal border: The boundary between the cornea and sclera becomes indistinct. In cases with peripheral opacity, accurate measurement of corneal diameter is difficult.
Corneal flattening: Flattening of the cornea is clearly visible on slit-lamp examination from the side.
Corneal neovascularization: Invasion of blood vessels from the episclera and conjunctiva is observed throughout the entire thickness of the cornea.
Craniofacial abnormalities: Related to abnormal formation of tissues derived from neural crest cells.
Cardiovascular malformations: Rarely associated.
Urogenital malformations: Rarely associated.
Skin abnormalities: Related to neural crest cell abnormalities.
QWhat is the risk of glaucoma?
A
In sclerocornea, corneal flattening and narrowing of the anterior chamber increase the risk of secondary glaucoma. Developmental glaucoma typically occurs after the teenage years. The risk is considered higher in cases with autosomal recessive mutations. Angle abnormalities are often present, and regular intraocular pressure evaluation is essential.
Sclerocornea results from abnormal migration of neural crest cells during embryonic development. Normally, the limbal anlage forms at 7–10 weeks of gestation, defining the corneal curvature and the border between the cornea and sclera. Failure of this structure to form disrupts the normal boundary between the sclera and cornea, leading to flattening of the corneal curvature.
CNA1 (Cornea Plana 1): Autosomal dominant inheritance. The locus is on the long arm of chromosome 12, but the causative gene has not been identified.
CNA2 (Cornea Plana 2): Autosomal recessive inheritance. Caused by mutations in the KERA gene in the 12q22-q23 region. The KERA gene encodes keratocan, a keratan sulfate proteoglycan important for corneal transparency. CNA2 is associated with more severe corneal flattening and anterior segment abnormalities.
PAX6, FOXC1, PITX2: Mutations may be associated with iridocorneal adhesions, corectopia, and iris atrophy.
RAD21: A mutation identified in families with sclerocornea. It regulates the differentiation of neural crest cells into corneal keratocytes or scleral stromal cells via WNT9B signaling.
Slit-lamp microscopy: Evaluates the extent and severity of corneal opacity, indistinctness of the corneal limbus, and presence of vascular invasion. Flattening of the cornea can be confirmed by lateral observation.
Anterior segment optical coherence tomography (AS-OCT): Allows non-invasive and rapid evaluation. It has the advantage of being assessable without anesthesia in newborns. It images corneal thickness and scleralization due to high reflectivity.
Genetic testing: Searches for mutations in genes such as KERA, PAX6, FOXC1, PITX2, and RAD21. Performed in conjunction with genetic counseling.
Systemic evaluation: Checks for associated systemic abnormalities such as intellectual disability, hearing loss, cardiovascular malformations, and genitourinary malformations.
Peters anomaly: Involves central corneal opacity with defects in Descemet’s membrane and corneal endothelium. Presents with iridocorneal adhesions or iridolenticular adhesions.
Congenital glaucoma: Opacity due to corneal edema, differentiated by increased corneal diameter (buphthalmos) and Descemet’s membrane ruptures (Haab’s striae).
Congenital hereditary endothelial dystrophy (CHED): Bilateral diffuse corneal edema and opacity, but the corneal limbus is clear.
Birth trauma: Often unilateral, accompanied by Descemet’s membrane rupture.
For corneal opacity affecting the visual axis, penetrating keratoplasty (PKP) is the first choice. Surgery should be performed as early as possible to avoid form deprivation amblyopia. However, visual prognosis is poor, and the rate of graft rejection is high.
Reports on transplantation outcomes:
Full-thickness corneal transplantation for sclerocornea shows approximately 75% failure, with the main cause being neovascularization of the limbal region.
A case series of 15 total and 12 partial types reported a 1-year graft survival rate of 70%.
In pediatric cases, the 1-year graft clarity rate is reported to be only about 37%.
In cases of corneal transplant failure, peripheral neovascularization is a risk factor, and concurrent anterior segment reconstruction surgery (e.g., angle reconstruction, pupilloplasty, lens extraction, intraocular lens repositioning) may be required 1).
In partial types where the visual axis is preserved, early optical correction (glasses) should be performed to prevent amblyopia due to high hyperopia. In cases with glaucoma, intraocular pressure management with eye drops or surgery is necessary.
QWhat is the success rate of corneal transplantation?
A
The prognosis of corneal transplantation for sclerocornea is poor. Reports indicate a 1-year graft survival rate of 37–70%, with 75% eventually failing. The main factor for failure is neovascularization of the limbal region. In pediatric cases, the prognosis is even worse, and multiple regrafts may be required.
6. Pathophysiology and Detailed Mechanism of Onset
Normal anterior segment development involves three important processes: formation from the neuroectoderm of the forebrain, separation of the lens vesicle from the surface ectoderm, and anterior migration of mesenchymal progenitor cells derived from the neural crest.
In normal development, after the lens vesicle separates at 4 weeks of gestation, the surface ectoderm differentiates into corneal epithelium. At 6 weeks, neural crest cells near the anterior rim of the optic cup enter between the corneal epithelium and lens, forming Bowman’s layer and the corneal endothelium. Subsequently, neural crest cells re-enter between Bowman’s layer and the corneal endothelium to form the corneal stroma. At 7 weeks, the sclera begins to form from neural crest cells, progressing from anterior to posterior and reaching the posterior pole by 5 months of gestation.
In sclerocornea, the limbal primordium fails to form at 7–10 weeks of gestation, so the normal boundary between the cornea and sclera is not established. As a result, the corneal curvature flattens and the corneal stroma takes on sclera-like properties.
Epithelium: Immunohistochemically positive for keratin 3 and 12 (corneal epithelial markers), confirming its corneal origin. Goblet cells are absent.
Bowman’s layer: Either absent or accompanied by irregular patches of hyaline material.
Stroma: The lamellar structure of collagen fibers is disorganized and irregularly arranged. Fiber diameter is inconsistent, with thinner fibers in the deeper layers (sclera-like feature). However, the presence of glycosaminoglycans such as keratan sulfate and type I collagen suggests that the stroma is of corneal origin rather than scleral origin. Vascular invasion from the episclera and conjunctiva is present in the anterior and mid-stroma.
Descemet’s membrane: Absent or thinned (0.8–1.5 μm), with homogeneous material and fibroblast proliferation.
Endothelium: Complete absence of the endothelium has been reported in some cases.
QWhy does the cornea become white and opaque?
A
In sclerocornea, the collagen fiber arrangement in the corneal stroma is irregular and the lamellar structure is disorganized, so corneal transparency is not maintained. In the normal cornea, the regular arrangement of uniform collagen fibers controls light interference and maintains transparency, but in sclerocornea this structure is disrupted. In addition, vascular invasion throughout the entire corneal thickness also contributes to opacity.
A RAD21 gene mutation was identified in a family with sclerocornea. RAD21 is a component of the cohesin complex and is involved in the regulation of gene expression. Research has found that in processes influenced by RAD21 expression, WNT9B plays a crucial role in determining the differentiation direction of neural crest cells into corneal keratocytes or scleral stromal cells.
This finding provides clues to understanding why corneal and scleral stromal cells, both derived from neural crest cells, have different tissue characteristics. In the future, development of new therapeutic strategies through regulation of the WNT9B signaling pathway is expected.