Congenital ectropion uveae (CEU) is a rare disease characterized by ectropion uveae present from birth and secondary glaucoma due to dysgenesis of the trabecular meshwork and Schlemm’s canal. Alternative names include congenital irisectropion syndrome and primary iris pigment epithelium hyperplasia.
In the EGS guidelines, CEU (ectropion uveae) is classified as a type of childhood glaucoma associated with congenital ocular malformations 1). Along with Axenfeld-Rieger anomaly, Peters anomaly, aniridia, and persistent fetal vasculature, it is included in glaucoma associated with non-acquired ocular diseases 1).
The term “congenital ectropion” was first introduced by Colsman in 1869, but his description was later found to be iris mammillations. The first accurate descriptions of CEU were by Wicherkiewicz in 1891 and Spiro in 1896.
QWhat is the difference between congenital uveal ectropion and acquired uveal ectropion?
A
Congenital uveal ectropion is present at birth, caused by incomplete regression of the primitive endothelium in the anterior chamber, and is non-progressive. Acquired uveal ectropion occurs due to traction from fibrovascular membranes associated with proliferative diabetic retinopathy or central retinal vein occlusion, and progresses unless the underlying disease is treated. Congenital uveal ectropion is unilateral and seen in children, while acquired uveal ectropion is more common in adults.
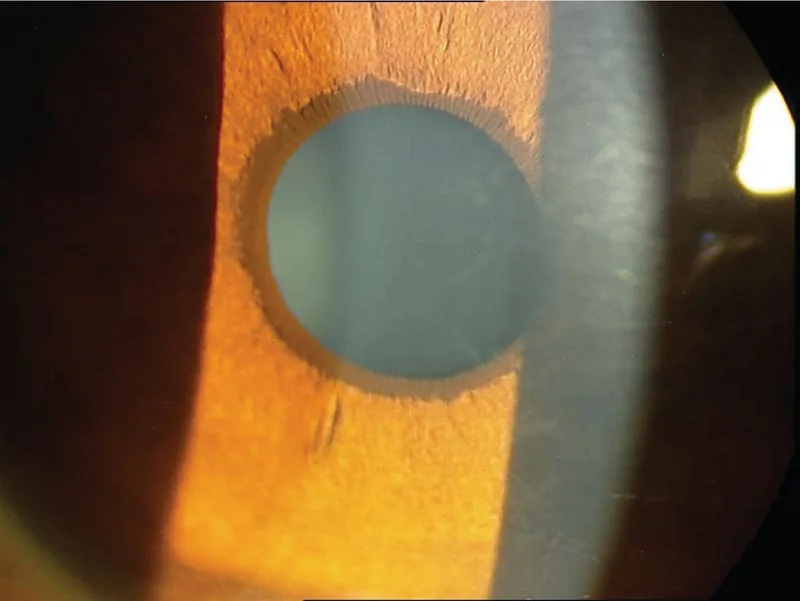
J Ophthalmic Vis Res. 2019 Jul 18;14(3):370-375. Figure 2. PMCID: PMC6815341. License: CC BY.
Slit-lamp photograph showing uveal ectropion of the left eye. The iris posterior pigment epithelium is everted at the pupillary margin, and the difference from the normal contralateral eye is visible.
CEU usually occurs unilaterally (bilateral cases have also been reported).
Iris findings: Glassy, smooth iris surface without crypts, iris stromal atrophy, proliferation of pigment epithelium on the anterior iris surface
Pupil: Usually round with light reflex. May appear irregular due to abnormal pigment epithelium.
Gonioscopy: High insertion of the iris (may extend to Schwalbe’s line). No peripheral anterior synechiae (PAS) or lesions beyond it.
Eyelid: Mild ptosis may be present in the affected eye (levator function is normal; related to the neural crest origin of Müller’s muscle).
Glaucoma: Enlarged optic disc cupping, marked asymmetry between eyes. Often accompanied by significantly elevated intraocular pressure in the affected eye.
The age at diagnosis of glaucoma varies widely, from 7 months to 42 years according to reports. It is often diagnosed in late school age to adolescence.
The cause of CEU is incomplete regression of the primitive endothelium covering the anterior chamber. This incomplete regression is thought to result from arrested development of neural crest tissue in utero. Incomplete regression induces reactive proliferation of the iris pigment epithelium, leading to high iris insertion and angle dysgenesis.
The trigger for developmental arrest has not been identified. Some authors hypothesize a primary vascular insult leading to defective migration of neural crest cells.
CEU has no specific inheritance pattern and is often not associated with systemic diseases. However, associations with the following conditions have been reported.
Neurofibromatosis type 1 (NF-1): The most important associated condition. In NF-1 patients, endothelialization of the iris creates traction forces, causing uveal ectropion. The presence of uveal ectropion is closely related to the risk of developing glaucoma.
In a cohort of 56 NF-1 patients, uveal ectropion was found in 8 of 13 patients with glaucoma. Among 43 patients without glaucoma, only 4 had uveal ectropion, and all of them had partial angle closure.
Multiple mutations in the CYP1B1 gene have been reported in neonatal-onset CEU3). CYP1B1 is known as a causative gene for primary congenital glaucoma (PCG) and is associated with glaucoma accompanied by congenital anterior chamber dysgenesis3).
Humphrey visual field test: evaluate characteristic glaucomatous visual field defects
The diagnostic criteria for childhood glaucoma include meeting two or more of the following: intraocular pressure >21 mmHg, progressive increase in cup-to-disc ratio, corneal diameter enlargement, axial length elongation, and visual field defects consistent with glaucomatous optic neuropathy2). In infants and young children, examination under general anesthesia may be necessary1)2).
Both are unilateral and present with pupillary abnormalities, but ICE syndrome often occurs in middle-aged women and is characterized by high peripheral anterior synechiae (PAS) extending beyond Schwalbe’s line. CEU is present from birth and does not show peripheral anterior synechiae. Also, ICE is progressive, while the uveal ectropion of CEU itself is non-progressive.
Used as a bridge to surgery or for postoperative intraocular pressure control.
Beta-blockers: Can be used in children. In neonates, be aware of the risk of apnea.
Carbonic anhydrase inhibitors (CAI): Used both topically and systemically. Oral acetazolamide (5-10 mg/kg every 6-8 hours) is also possible.
Prostaglandin analogs: Also used in children.
Alpha-2 agonists (brimonidine): Contraindicated in children under 2 years (risk of respiratory depression and CNS depression). Avoid in children under 8 years if possible.
Glaucoma treatment for CEU primarily requires surgical intervention1).
First-line
Trabeculectomy: with or without antimetabolite (mitomycin C). In CEU, because angle dysgenesis is severe, the success rate of goniotomy is significantly lower than in primary congenital glaucoma1).
Trabeculotomy: can be performed regardless of corneal opacity. In cases with increased corneal diameter, the sclera is thin, so care must be taken to avoid perforation.
The success rate of goniotomy for primary congenital glaucoma is high at 94% between 1 month and 2 years of age, but this rate cannot be expected in CEU1).
QCan glaucoma in CEU be treated with goniotomy?
A
In CEU, because angle dysgenesis is severe, the success rate of goniotomy is significantly lower than in primary congenital glaucoma (PCG). In many cases, trabeculectomy with antimetabolite is the first-line treatment. In refractory cases, implantation of a glaucoma drainage device may be necessary.
The pathogenesis of CEU centers on reactive proliferation of the iris pigment epithelium. This proliferation is induced by incomplete regression of the primitive endothelium covering the anterior chamber.
As a mechanism for incomplete regression, arrest of neural crest tissue development in utero has been proposed. Neural crest cells are precursor cells that form the corneal endothelium, trabecular meshwork, and iris stroma of the anterior chamber, and arrest of their migration leads to underdevelopment of the entire anterior chamber.
“A primary vascular disorder leading to neural crest cell migration defects may be involved in the pathogenesis of CEU.”
Histopathological examination has reported CEU cases with a fibrovascular membrane in the anterior iris stroma, supporting a causal relationship between vascular disorder and neural crest migration defect (Harasymowycz et al.).
A different mechanism is postulated for CEU associated with NF-1. Endothelialization of the iris generates traction, pulling the iris pigment epithelium to the anterior iris surface. This change, along with iridocorneal adhesions, leads to glaucoma.
Glaucoma in CEU is primarily due to increased resistance to aqueous humor outflow caused by high iris insertion and underdevelopment of the trabecular meshwork and Schlemm’s canal1). In pediatric glaucoma generally, reduced aqueous outflow causes a marked elevation of intraocular pressure1)2).
Visual impairment in CEU is closely related to the severity of glaucoma. Visual prognosis depends largely on early diagnosis and early treatment of elevated intraocular pressure, but no clear correlation has been found between the severity of uveal ectropion and the severity of glaucoma. Neonatal-onset cases are characterized by bilateral severe glaucoma and may be treatment-resistant.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.