Acquired ectropion uveae (AEU) is a condition in which the iris pigment epithelium prolapses or protrudes onto the anterior surface of the iris. It is also called acquired irisectropion. It commonly occurs near the pupil but can also occur in other parts of the iris.
Ectropion uveae can be congenital or acquired. Congenital ectropion uveae (CEU) results from delayed development of neural crest cells and is generally non-progressive. In contrast, AEU is secondary to various underlying diseases such as ischemia, inflammation, or tumors, and follows a progressive course 1).
ICE syndrome: 24.6% develop AEU. In Cogan-Reese syndrome, 54.2%
QHow do congenital and acquired ectropion uveae differ?
A
Congenital ectropion uveae is caused by delayed development of neural crest cells, with the iris stroma and sphincter muscle remaining normal, and is usually non-progressive. Acquired ectropion uveae is caused by traction of the iris stroma and sphincter muscle anteriorly due to fibrovascular membrane or corneal endothelial cell proliferation, accompanied by peripheral anterior synechiae and progression 1). For details, see the section on Pathophysiology.
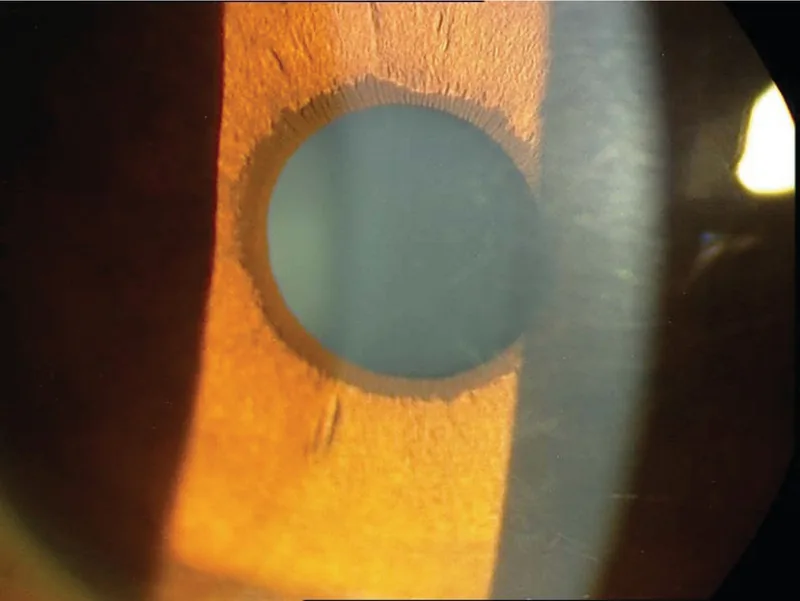
Hatami M, et al. Glaucoma in Ectropion Uveae Syndrome: A Case Report and Literature Review. Journal of Ophthalmic & Vision Research. 2019;14(3):370-375. Figure 2. PMCID: PMC6815341. License: CC BY.
Slit-lamp photograph. The iris pigment epithelium of the left eye is everted anteriorly from the pupillary margin, showing ectropion uveae. This provides a clue for considering anterior chamber angle abnormalities and secondary glaucoma.
Findings depend on the underlying disease. Conditions that caused neovascularization, such as retinal vein occlusion, proliferative diabetic retinopathy, chronic retinal detachment, and arterial occlusion, are observed.
Uveitis is a disease that frequently complicates glaucoma, and about 20% of uveitis patients have glaucoma3). Aqueous outflow obstruction due to iridocyclitis is classified into acute type (trabecular meshwork accumulation of inflammatory cells, trabecular edema, angle closure due to ciliary body swelling) and chronic type (scar formation, angle coverage by membranous tissue) 2)3).
Angle rubeosis (neovascularization) due to chronic inflammation is also seen in Behçet’s disease and juvenile chronic iridocyclitis, and can cause AEU.
QDoes diabetes make you more prone to uveal ectropion?
A
When diabetic retinopathy progresses, retinal ischemia leads to iris neovascularization (NVI), which causes AEU. However, it does not occur in all diabetic patients and can be prevented by controlling blood glucose and blood pressure and regular fundus examinations.
Specular microscopy: Performed when ICE syndrome or NF-1 is suspected. In NF-1, decreased corneal endothelial density, polymegathism (uneven cell area), and pleomorphism (uneven cell morphology) may be observed 1)
Fundus examination: Identification of underlying diseases (retinal ischemia, tumor, etc.)
Abnormal proliferation of corneal endothelial cells
In congenital ectropion uveae, the iris stroma and sphincter muscle are preserved, whereas in AEU these structures are also inverted, which is an important distinguishing feature. Axenfeld-Rieger syndrome is bilateral, characterized by a posterior embryotoxon where Schwalbe’s line is located anterior to the limbus, and may be associated with sensorineural hearing loss and cardiac or craniofacial abnormalities.
The EGS Guidelines (5th edition) recommend treatment of NVG divided into treatment of the underlying disease/retinal ischemia and intraocular pressure management 2).
Filtration surgery: Trabeculectomy with antimetabolites (mitomycin C, 5-FU). If NV activity is quiescent, a relatively good prognosis can be expected 2)
Tube shunt surgery: Recommended for cases resistant to drug therapy. In NVG, long-tube devices (such as Baerveldt) are commonly chosen 2)
In AEU associated with uveitis, the goal is simultaneous treatment of inflammation and intraocular pressure2). Anti-inflammatory therapy with steroids (topical and systemic) and intraocular pressure management with antihypertensive agents are performed concurrently. Steroids themselves can cause elevated intraocular pressure, so careful monitoring is necessary 3).
Antihypertensive eye drops are used in the order of beta-blockers, prostaglandin analogs, and carbonic anhydrase inhibitors. If intraocular pressure elevation is severe, oral carbonic anhydrase inhibitors and intravenous D-mannitol are added.
Iris melanoma: Appropriate treatment for the tumor (resection, radiation therapy, etc.)
QWhen is surgery necessary?
A
Surgery is considered when intraocular pressure cannot be adequately controlled with drug therapy (antihypertensive eye drops, anti-VEGF therapy). In NVG, tube shunt surgery is commonly chosen. Even in cases with extensive angle closure such as NF-1, there are reports of good intraocular pressure control with tube shunt surgery 1).
The central mechanism is the formation of a contractile fibrovascular membrane on the anterior surface of the iris. This membrane pulls the posterior pigment epithelium around the pupillary margin, the iris sphincter muscle, and the iris stroma forward, causing tractional curling. At the same time, it covers and occludes the trabecular meshwork, leading to increased intraocular pressure.
In NVG, retinal ischemia leads to the production of angiogenic factors such as VEGF, resulting in abnormal new blood vessels on the anterior iris (iris rubeosis) 2). Initially, it presents as open-angle glaucoma with elevated intraocular pressure, but as the fibrovascular membrane contracts, it progresses to synechial angle closure 2).
Aqueous outflow obstruction due to uveitis is classified into acute and chronic types 3).
Acute type (usually reversible): accumulation of inflammatory cells in the trabecular meshwork spaces, trabecular edema, and angle closure due to ciliary body swelling
Chronic type: scar formation in the angle, angle coverage by membranous tissue
When posterior synechiae become circumferential, iris bombe due to pupillary block occurs, leading to further elevation of intraocular pressure. Steroid treatment itself also contributes to increased intraocular pressure in some patients 2).
In NF-1, proliferation of corneal endothelial cells similar to ICE syndrome is considered the cause of uveal ectropion1). Edward et al.’s histological study confirmed corneal endothelial cell overgrowth in all 5 eyes with NF-1, and gene expression analysis showed loss of neurofibromin (NF1 gene product) and increased MAPK (mitogen-activated protein kinase) expression 1). Corneal endothelial cells cross Schwalbe’s line, invade the trabecular meshwork, and cause Descemetization of the angle, iris atrophy, pupillary deviation, and uveal ectropion.
QAre the mechanisms of uveal ectropion in ICE syndrome and NF-1 common?
A
Both share a common mechanism: abnormal proliferation of corneal endothelial cells invades the angle and causes uveal ectropion1). However, in NF-1, endothelial cell proliferation is due to loss of neurofibromin, which differs from ICE syndrome at the molecular level.
7. Latest research and future perspectives (research-stage reports)
Esfandiari et al. (2022) reported a case of progressive AEU and secondary angle-closure glaucoma associated with NF-11). An 11-year-old Hispanic boy with mild pupillary irregularity and uveal ectropion at age 3 showed AEU extending from 8 to 4 o’clock, with complete closure of the superior angle. IOP was 28 mmHg at age 6 and reached 35 mmHg at age 9 under maximum medical therapy. A Baerveldt glaucoma implant (BGI 101-350) was placed in the inferonasal quadrant, achieving good IOP control of 11-18 mmHg over 29 months postoperatively.
In the same report, postoperative specular microscopy revealed decreased endothelial density, polymegathism, and pleomorphism in the superior cornea of the affected eye, supporting the hypothesis of corneal endothelial cell proliferation in NF-11).
Pathological findings on glaucoma mechanisms in NF-1
Histopathological examination of 5 eyes with NF-1 and unilateral glaucoma confirmed uveal ectropion and corneal endothelial overgrowth in all cases1). Gene expression analysis in one case showed loss of neurofibromin and increased MAPK expression in corneal endothelial cells. It has been hypothesized that AEU results from corneal endothelial cell proliferation and angle invasion.
The progressive nature of AEU in NF-1 has been observed from childhood over long periods, suggesting the importance of regular anterior segment evaluation and intraocular pressure monitoring1).
Esfandiari H, Lasky Zeid J, Tanna AP. Progressive ectropion uveae and secondary angle-closure glaucoma in type 1 neurofibromatosis. American journal of ophthalmology case reports. 2022;25:101345. doi:10.1016/j.ajoc.2022.101345. PMID:35169657; PMCID:PMC8829075.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
Siddique SS, Suelves AM, Baheti U, Foster CS. Glaucoma and uveitis. Surv Ophthalmol. 2013;58(1):1-10.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.