Elevated episcleral venous pressure (EVP) is a condition in which intraocular pressure (IOP) rises due to abnormal elevation of venous pressure downstream of the aqueous humor outflow pathway, leading to secondary open-angle glaucoma3). In the classification of glaucoma, it is categorized as secondary open-angle glaucoma where the main resistance to aqueous outflow is located posterior to Schlemm’s canal 4). The angle is essentially open.
Normal EVP values range from 8 to 11.5 mmHg and vary with body position. There is no clinically available device to measure EVP; elevated EVP is usually inferred indirectly from clinical findings and imaging. According to Goldmann’s equation, intraocular pressure is expressed by the following relationship:
IOP = (F / C) + EVP
Here, F is the aqueous humor production rate (μL/min), C is the aqueous humor outflow facility (μL/min/mmHg), and EVP is the episcleral venous pressure (mmHg). As this equation shows, an increase in EVP directly leads to an increase in IOP. Measured data indicate that a 1 mmHg rise in EVP increases IOP by approximately 0.83 ± 0.21 mmHg, with a linear relationship between the two. Normal EVP values in healthy eyes range from “8–10 mmHg” to “8–11.5 mmHg” depending on the literature, but in all cases, EVP plays an important role in determining IOP as the downstream pressure of the aqueous outflow pathway.
In the conventional outflow pathway, aqueous humor flows from Schlemm’s canal through collector channels, the deep scleral venous plexus, the intrascleral venous plexus, and the episcleral venous plexus, eventually joining the superior ophthalmic vein. The superior ophthalmic vein drains into the cavernous sinus, then via the internal jugular vein and superior vena cava to the right atrium. Obstruction or pressure elevation at any point along this route can lead to elevated EVP 3).
When IOP is above 8 mmHg (equivalent to episcleral venous pressure), aqueous inflow into Schlemm’s canal increases linearly in proportion to IOP.
During nighttime sleep in the supine position, EVP increases. This is one of the main mechanisms of IOP elevation during sleep. Changing from a sitting to a supine position reduces venous return from the head, raising episcleral venous pressure. Even in normal individuals, IOP increases by 1–6 mmHg in the supine position, but in patients with underlying conditions that elevate EVP, this fluctuation is amplified. IOP changes with postural changes are also used as an aid in diagnosing elevated EVP.
When all other causes are excluded, the condition is diagnosed as idiopathic (Radius-Maumenee syndrome) 1). It was first described by Minas and Podos in 1968, and named after Radius and Maumenee, who reported four cases in 1978 1). It is extremely rare, with approximately 60 cases reported in the literature 1).
QWhy does elevated episcleral venous pressure increase intraocular pressure?
A
According to the Goldmann equation, intraocular pressure (IOP) is determined by aqueous humor production, outflow resistance, and episcleral venous pressure (EVP). Aqueous humor drains from Schlemm’s canal through collector channels and episcleral veins into the systemic circulation. When venous pressure increases downstream in this outflow pathway, resistance to aqueous outflow from Schlemm’s canal increases. As a result, aqueous humor accumulates in the eye, raising IOP. A linear relationship exists: a 1 mmHg rise in EVP increases IOP by approximately 0.83 mmHg.
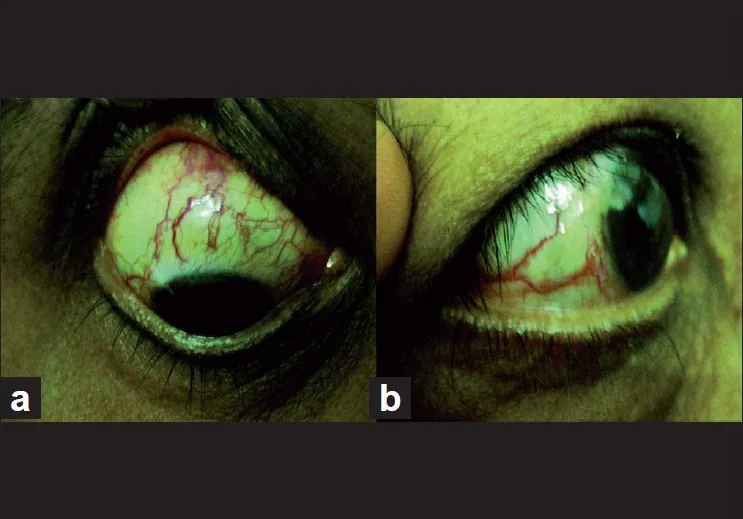
Estacia CT, Gameiro Filho AR, da Silveira IBE. Radius-Maumenee syndrome (idiopathic dilated episcleral vessels). GMS Ophthalmol Cases. 2024;14:Doc15. Figure 1. PMID: 39811492; PMCID: PMC11730685. DOI: 10.3205/oc000247. License: CC BY 4.0.
Slit-lamp photograph (A) shows tortuous and dilated episcleral vessels; gonioscopic photograph (B) shows blood reflux into Schlemm’s canal. This corresponds to elevated venous pressure downstream of the aqueous outflow pathway, discussed in section “2. Main Symptoms and Clinical Findings.”
Patients with elevated EVP often present with chronic ocular hyperemia that does not respond to conventional treatment. It is frequently misdiagnosed as chronic conjunctivitis3). Usually, there are few complaints of pain or irritation.
In acute cases (e.g., carotid-cavernous fistula), ocular irritation and pain may occur 3). In CCF, patients may perceive an intracranial bruit synchronized with the pulse. Diplopia due to ocular motility disturbance may also be present.
Clinical Findings (Findings Confirmed by Physician Examination)
A characteristic finding is spiral episcleral vessel dilation without inflammation, and gonioscopy reveals an open angle and blood reflux into Schlemm’s canal 1, 2). In chronic cases, hyalinization of the Schlemm’s canal wall may also be observed.
Pulsatile proptosis: due to arterial blood flow from the cavernous sinus into the orbit
Bruit: heard with a stethoscope over the orbit or temporal region
Conjunctival injection and chemosis: tortuous and engorged conjunctival vessels are called “caput Medusae”
Other findings include ocular motor nerve (oculomotor, abducens, trochlear) palsy causing eye movement disorders and diplopia, retinal hemorrhage, venous tortuosity and dilation, choroidal detachment, eye pain, headache, and tinnitus.
Clinical differences between Direct CCF and Dural CCF:
Direct CCF: Direct flow from the main trunk of the internal carotid artery into the cavernous sinus. Shunt volume is large and symptoms are severe. 75% are due to head trauma, but recent reports indicate an increasing proportion of idiopathic cases.
Dural CCF (dural arteriovenous fistula): Blood flows from dural penetrating branches of the internal or external carotid artery into the cavernous sinus. Congenital arteriovenous malformations, hypertension, and diabetes can be triggers. The shunt volume is small and the course is chronic. In cases where drainage is mainly into the inferior petrosal sinus and reflux into the superior ophthalmic vein is minimal, characteristic ocular symptoms may not appear, so caution is required.
It occurs secondary to infections of the face, orbit, pharynx, or paranasal sinuses. Staphylococcus aureus is the most common causative organism. Acute onset with fever, marked eyelid swelling, proptosis, and diplopia due to extraocular muscle palsy. Engorgement and tortuosity of conjunctival vessels, decreased visual acuity, and papilledema are characteristic. Bilateral cases with contralateral extension may occur. Prompt treatment with antibiotics is essential; delay can lead to serious complications.
It is a localized phakomatosis characterized by the triad of facial hemangioma (port-wine stain), ipsilateral leptomeningeal angioma, and glaucoma. Most cases are sporadic, and the cause is thought to be abnormal vascular development due to sympathetic nerve dysfunction during the embryonic period. A characteristic flame nevus (usually unilateral) is present at birth in the distribution of the first and second branches of the trigeminal nerve.
Glaucoma is the most important ocular finding and is associated with the following findings:
Dilation and tortuosity of conjunctival and episcleral vessels: Reflects elevated EVP
Choroidal hemangioma: The fundus shows a diffuse red color. Fluorescein angiography shows a pattern of large choroidal vessels in the early phase and hyperfluorescence of the entire tumor in the late phase.
Tortuosity of retinal vessels: Reflects circulatory disturbance associated with choroidal hemangioma
Ipsilateral leptomeningeal angioma leads to progressive cerebral cortical atrophy and calcification, and epileptic seizures (often refractory) develop with high frequency by age 3. It may be complicated by mental developmental delay, hemiparesis, and homonymous hemianopia.
Eyelid symptoms such as upper eyelid swelling and upper eyelid retraction appear early. Proptosis, diplopia, and visual impairment are present. Increased intraorbital pressure due to extraocular muscle hypertrophy causes venous stasis, which is a mechanism of EVP elevation. It is often associated with hyperthyroidism, but may also occur as euthyroid ophthalmopathy.
It often occurs unilaterally or bilaterally asymmetrically1, 2). In a case of a 38-year-old woman, the main complaint was redness in the right eye persisting for more than 3 years, with diffuse engorgement of episcleral vessels, IOP 22 mmHg (on timolol), and normal fundus findings1).
Superior vena cava syndrome: Obstruction of the superior vena cava due to mediastinal tumors, etc. Accompanied by venous stasis of the entire head and neck3).
Cavernous sinus thrombosis: Secondary to facial, orbital, or sinus infections. The causative bacteria are often staphylococci. Presents with fever, eyelid swelling, proptosis, extraocular muscle palsy, and papilledema.
Thyroid eye disease: Venous stasis due to extraocular muscle hypertrophy and increased orbital pressure is the mechanism of EVP elevation. TSH receptors act as antigens, leading to lymphocyte infiltration and inflammatory response in the orbit.
Others: Orbital tumors, orbital pseudotumor, orbital phlebitis, jugular vein occlusion (after neck dissection), pulmonary vein occlusion3).
Arteriovenous anomalies and idiopathic
Carotid-cavernous fistula (CCF): Direct type involves direct inflow from the internal carotid artery trunk, with large shunt volume and severe symptoms. Dural type involves inflow from dural perforating branches and follows a chronic course.
Dural fistula: Low-flow arteriovenous shunt3)
Sturge-Weber syndrome: Vascular developmental abnormality due to sympathetic nerve dysfunction during the embryonic period. When a hemangioma is present on the eyelid, glaucoma develops in 30–70% of cases4).
Orbital varix: Characterized by proptosis that worsens with the Valsalva maneuver.
Radius-Maumenee syndrome: Diagnosis of exclusion. Approximately 60 cases reported1).
EGS classifies the etiology of EVP elevation in more detail3).
Orbital/episcleral diseases: Episcleral venous obstruction due to chemical burns or radiation, Sturge-Weber syndrome, Nevus of Ota, endocrine orbital disease (thyroid eye disease), orbital tumors/pseudotumors, orbital phlebitis.
In CCF, persistent ocular ischemia can lead to neovascularization of the iris and angle, posing a risk of neovascular glaucoma. If left untreated, blood may reflux into the cerebral venous system, potentially causing cavernous sinus rupture, cerebral hemorrhage, or subarachnoid hemorrhage, especially in Direct CCF. This can be directly life-threatening.
In scleritis or episcleritis, inflammation spreading to the episcleral veins can cause aqueous outflow obstruction and elevated intraocular pressure10).
Onset timing and etiology of Sturge-Weber syndrome
Early-onset type (immediately after birth to 4 years): Accounts for about 60%. Primarily due to angle developmental abnormalities.
Late-onset type (infancy or later): Involves EVP elevation and choroidal hemangioma
QWhat are the causes of elevated episcleral venous pressure?
A
They are broadly classified into three groups: venous occlusion (superior vena cava syndrome, cavernous sinus thrombosis, thyroid eye disease, orbital tumor), arteriovenous abnormalities (carotid-cavernous fistula, dural fistula, Sturge-Weber syndrome, orbital varix), and idiopathic (Radius-Maumenee syndrome). CCF is classified into direct and dural types; the direct type has a large shunt volume and strong symptoms. Radius-Maumenee syndrome is a diagnosis of exclusion, made after all secondary causes have been ruled out by imaging.
CT/MRI: Evaluate enlargement of the cavernous sinus, dilation of the superior ophthalmic vein, and enlargement of extraocular muscles. In mild CCF, CT/MRI findings may not be obvious 1)
MRI-specific findings: The normal cavernous sinus shows contrast enhancement on MRI, but in CCF, due to high blood flow velocity, it appears as a flow void (signal loss area)
MRA: Useful for visualizing dilation of the superior ophthalmic vein and the cavernous sinus and abnormal vessels
Definitive diagnosis: Cerebral angiography (confirmation of arteriovenous shunting from the internal and external carotid arteries) is required. For dural CCF, four-vessel angiography of both internal and external carotid arteries is needed
CT angiography: Useful for evaluating vascular abnormalities in the orbit and cranium
Direct puncture (most accurate) and indirect methods (venous pressure gauge, air jet, etc.) exist, but they have not been adopted for routine clinical use 2). There is no device for measuring EVP in clinical practice.
Should be performed in all cases of elevated EVP 1). A diagnosis of thyroid eye disease is made when any of TSH receptor antibodies (TRAb, TSAb), anti-TG antibodies (TgAb), or anti-TPO antibodies (TPOAb) are positive.
Diagnosed by skin findings + epileptic seizures + intracranial calcifications on head CT. Even before calcification appears, brain lesions can be detected by contrast-enhanced MRI and SPECT. In children, precise intraocular pressure measurement, anterior segment, angle, and fundus examination under general anesthesia are essential. Fluorescein fundus angiography is useful for diagnosing choroidal hemangioma, showing a large choroidal vascular pattern in the early phase and hyperfluorescence of the entire tumor in the late phase.
It is important to differentiate from diseases that present with chronic ocular congestion.
Episcleritis/scleritis: Inflammatory vasodilation that blanches with pressure. Often painful 10)
Chronic conjunctivitis: Diffuse conjunctival congestion. Shows a different distribution from the spiral vascular dilation of elevated EVP
Acute angle-closure glaucoma: Involves angle closure, with a different pathophysiology from elevated EVP
Rosacea: Accompanied by facial flushing and telangiectasia
Polycythemia vera: Accompanied by conjunctival vascular engorgement, but with systemic erythrocytosis as the background
In cases of Radius-Maumenee syndrome, it has been reported that intracranial MRI angiography, thyroid function tests, and cerebral angiography were all normal 1). A diagnosis of idiopathic disease is made only when no abnormalities are found in these tests.
The basis of treatment is treatment of the underlying disease, and collaboration with other departments such as neurosurgery is necessary 3). If EVP normalizes with treatment of the underlying disease, intraocular pressure improves, but in some cases, high intraocular pressure persists even after treatment of the underlying disease. Drug therapy similar to that for primary open-angle glaucoma is performed, but in many cases, intraocular pressure control is achieved with drug therapy alone and surgery is not required.
Aqueous Humor Production Suppressants (First-line)
Beta-blockers: Timolol 0.5%, etc. Suppress aqueous humor production and are effective even under elevated EVP 3)
Carbonic anhydrase inhibitors (CAI): Dorzolamide 1%, brinzolamide 1% eye drops, oral acetazolamide (severe cases). Effect is enhanced when used with beta-blockers 3)
Fixed combinations: Beta-blocker + CAI fixed combinations are useful for improving medication adherence
Rho Kinase Inhibitors and Others
Netarsudil 0.02%: Increases trabecular outflow + EVP-lowering effect. IOP reduction rate 20–25%. After instillation, EVP decreases by an average of 0.79 mmHg 3)
Ripasudil 0.4%: Increases trabecular outflow. IOP reduction rate approximately 20%. Eight hours after instillation, the aqueous humor column width in the episcleral vein significantly increases 3)
Prostaglandin-related drugs: Effect is limited because they dilate the entire episcleral vessels. They have some effect by promoting outflow through alternative pathways
In 6 eyes with Sturge-Weber syndrome-associated glaucoma, significant IOP reduction after adding netarsudil has been reported.
Cavernous sinus thrombosis: Antibiotic administration is the mainstay of treatment
CCF: If the shunt volume is small, observation (may close spontaneously in a few months). Surgical indications include large shunt volume, persistent IOP elevation, visual loss, diplopia, risk of cerebral hemorrhage or subarachnoid hemorrhage, and when spontaneous closure is not expected. Surgical treatment includes endovascular surgery (for fistula closure) performed by neurosurgeons
Trabeculectomy: An appropriate surgical option, but in eyes with elevated episcleral venous pressure (EVP), there is a high risk of choroidal effusion. Adjustable sutures are recommended to prevent rapid intraocular pressure drop during surgery 2).
Glaucoma drainage device (GDD): Ahmed valve or Baerveldt implant is used for refractory cases. Five-year outcomes show GDD is better than trabeculectomy in reoperation cases 2).
XEN45 gel stent: A minimally invasive alternative. It preserves conjunctival tissue 2).
In a long-term follow-up of three cases of Radius-Maumenee syndrome, trabeculectomy, XEN45, Ahmed valve, Baerveldt implant, and cyclophotocoagulation were performed 2). All cases had at least one eye that underwent trabeculectomy, but reoperation was often required, and choroidal effusion (without hypotony) occurred in two cases 2). In case 1, XEN45 provided good intraocular pressure control over a long-term follow-up of 73 months 2).
Age-specific treatment algorithm for Sturge-Weber syndrome
Congenital/infantile onset: Trabeculotomy or goniotomy is indicated 4, 6, 7).
Older children (predominantly elevated EVP): Medical therapy is first-line4). If medical therapy or outflow reconstruction fails, consider trabeculectomy or tube shunt surgery with a plate 4, 8).
QHow is glaucoma associated with elevated episcleral venous pressure treated?
A
The first step in treatment is to address the underlying cause. For CCF, neurosurgical endovascular surgery is performed; for cavernous sinus thrombosis, antibiotics are administered. For intraocular pressure control, suppression of aqueous humor production with beta-blockers or carbonic anhydrase inhibitors is effective. Rho kinase inhibitors (netarsudil 0.02% and ripasudil 0.4%) have an effect of lowering EVP. In Sturge-Weber syndrome, treatment selection according to age is important: surgery is the first choice for infantile-onset cases, while medication is the first choice for older children. Filtration surgery carries a high risk of choroidal effusion and requires careful technique.
Aqueous humor is drained out of the eye via two pathways: the main pathway (80–95% of total outflow) and the accessory pathway (5–20%) 9). In the main pathway, aqueous humor flows through the trabecular meshwork → Schlemm’s canal → collector channels → aqueous veins → episcleral veins → superior ophthalmic vein → cavernous sinus → internal jugular vein → superior vena cava.
Aqueous outflow through the main pathway is pressure-dependent, increasing as intraocular pressure rises. However, when EVP is elevated, this compensatory mechanism alone is insufficient to normalize intraocular pressure.
When venous pressure increases downstream of the episcleral anastomosis, resistance to aqueous outflow from Schlemm’s canal to the episcleral veins increases 3). In chronic cases, blood reflux into Schlemm’s canal occurs, reducing aqueous outflow through the trabecular meshwork. As a result, intraocular pressure rises chronically, leading to glaucomatous optic neuropathy3).
Outflow via the accessory pathway (uveoscleral route) is non-pressure-dependent and less affected by EVP elevation. This characteristic provides the rationale for the moderate efficacy of prostaglandin-related drugs in promoting outflow through the accessory pathway.
In CCF, prolonged EVP elevation impairs ocular blood flow, leading to ocular ischemia. Because arterial blood shunts into the cavernous sinus, perfusion pressure in the ophthalmic artery decreases. Chronic ocular ischemia induces retinal ischemia, which stimulates production of vascular endothelial growth factor (VEGF), leading to neovascularization of the iris and angle, resulting in neovascular glaucoma. Once this stage is reached, the open angle becomes occluded, making treatment even more difficult. Treatment of CCF (closure of the fistula) may improve ocular ischemia and lead to regression of neovascularization, but advanced cases may leave irreversible angle damage.
Intraocular pressure elevation in Sturge-Weber syndrome: multifactorial mechanisms
Choroidal hemangioma-related increased permeability: leakage from thinned vessel walls
Because these multiple factors combine, glaucoma in Sturge-Weber syndrome is more refractory than developmental glaucoma. However, if good intraocular pressure control is achieved early, vision can be preserved.
QWhy is glaucoma in Sturge-Weber syndrome refractory?
A
Elevated intraocular pressure in Sturge-Weber syndrome is not due to a single mechanism but results from a combination of five factors: primary angle dysgenesis, Schlemm’s canal atrophy, EVP elevation, PAS formation, and choroidal hemangioma-related increased permeability. Therefore, drug therapy alone is often insufficient for pressure control. Furthermore, surgical treatment carries risks of suprachoroidal hemorrhage and retinal detachment associated with ipsilateral choroidal hemangioma, requiring careful decision-making.
A study using an automated venomanometer reported that after instillation of netarsudil 0.02%, EVP decreased by an average of 0.79 mmHg. Red blood cell-mediated angiography also confirmed a significant increase in episcleral venous outflow. For ripasudil, the aqueous humor column width in the episcleral vein significantly increased 8 hours after instillation, suggesting enhanced episcleral venous outflow.
Intracamerally administered bimatoprost selectively dilates the episcleral venous system and enhances outflow. Unlike topical prostaglandin analogs that dilate the entire episcleral vasculature, intracameral administration acts only on the venous system.
A novel topical eye drop that selectively targets episcleral vessels and reduces EVP. It has vasodilatory effects mediated by ATP-sensitive potassium channel modulation. It is under development, and preliminary data show significant intraocular pressure reduction and absence of serious side effects.
Long-term surgical outcomes of Radius-Maumenee syndrome
Elksne et al. (2023) reported long-term follow-up of three cases. In case 1, a XEN45 gel stent was inserted in the left eye, and good intraocular pressure control was achieved over 73 months of follow-up. Management of complications such as postoperative choroidal effusion and cystoid macular edema remains a challenge 2).
Estacia CT, Gameiro Filho AR, da Silveira IBE, Cas MED, Gameiro RR. Radius-Maumenee syndrome (idiopathic dilated episcleral vessels). GMS ophthalmology cases. 2024;14:Doc15. doi:10.3205/oc000247. PMID:39811492; PMCID:PMC11730685.
Elksne E, Steiner V, Hohensinn M, Reitsamer HA, Lenzhofer M. Radius-Maumenee syndrome: A case series with a long-term follow-up. Clinical case reports. 2023;11(2):e6918. doi:10.1002/ccr3.6918. PMID:36814708; PMCID:PMC9939581.
European Glaucoma Society. European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition. Br J Ophthalmol. 2021 Jun;105(Suppl 1):1-169. doi:10.1136/bjophthalmol-2021-egsguidelines. PMID:34675001.
Addison PK, et al. Serous retinal detachment induced by topical bimatoprost in a patient with Sturge-Weber syndrome. Eye (Lond). 2011;31:124-125.
Olsen KE, Huang AS, Wright MM. The efficacy of goniotomy/trabeculotomy in early-onset glaucoma associated with the Sturge-Weber syndrome. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 1998;2(6):365-8. doi:10.1016/s1091-8531(98)90036-2. PMID:10532726.
Iwach AG, Hoskins HD Jr, Hetherington J Jr, Shaffer RN. Analysis of surgical and medical management of glaucoma in Sturge-Weber syndrome. Ophthalmology. 1990;97(7):904-9. doi:10.1016/s0161-6420(90)32483-1. PMID:2381705.