Orbital decompression surgery is a procedure performed for proptosis and compressive optic neuropathy associated with thyroid eye disease (TED). It involves removing bone from the orbital walls (medial, inferior, and lateral walls) and, if necessary, resecting intraorbital fat tissue to expand the orbital volume and reposition the eye posteriorly.
Thyroid eye disease can occur in association with hyperthyroidism (Graves’ disease) or as euthyroid ophthalmopathy with normal thyroid function. It is essentially an autoimmune disease that progresses independently of thyroid hormone levels, involving thyroid-related autoantibodies. Enlargement of orbital fat and extraocular muscles increases intraorbital pressure, leading to proptosis.
Orbital decompression surgery has two main purposes.
Cosmetic purpose: Reduction of marked proptosis that does not improve with medication. Changes in appearance and social difficulties are criteria for determining indication.
Preservation of visual function: Relief of compressive optic neuropathy (dysthyroid optic neuropathy: DON) caused by enlarged extraocular muscles compressing the optic nerve at the orbital apex. This is the most important surgical purpose and can be an emergency indication.
Orbital decompression surgery is performed for optic neuropathy or marked proptosis that does not respond to medical treatment. During the inflammatory (active) phase, steroid pulse therapy or radiation therapy is generally given first. In cases of severe compressive optic neuropathy, emergency orbital decompression may be performed even during the inflammatory phase, but steroid treatment is continued postoperatively to control inflammation.
QIs surgery necessary for all cases of proptosis in thyroid eye disease?
A
Not all cases of proptosis require surgery. During the inflammatory phase, steroid pulse therapy (methylprednisolone 500–1,000 mg/day for 3 days as one course) or radiation therapy is the first choice, and many cases achieve resolution of inflammation and improvement of symptoms. Orbital decompression surgery is an established treatment option for optic neuropathy or marked proptosis that does not respond to medical treatment.
Clinical symptoms of thyroid eye disease are classified into four categories: eyelid symptoms, proptosis, diplopia, and visual impairment. In younger patients, proptosis is predominant, while in older patients, ocular motility disorders and diplopia are more common.
Visual impairment includes two types: decreased vision due to corneal damage and decreased vision due to compressive optic neuropathy from enlarged extraocular muscles. The inferior rectus and medial rectus are commonly affected, leading to vertical and esotropia.
Inflammatory phase (active phase): Edema and inflammation of retrobulbar tissues are predominant. Steroid pulse therapy and radiation therapy are prioritized. Orbital decompression is indicated only in emergencies with severe compressive optic neuropathy.
Non-inflammatory phase (chronic phase): The phase where inflammation subsides and fixed proptosis, ocular motility disorders, and optic neuropathy persist. This is the main indication period for orbital decompression.
CAS (Clinical Activity Score) is a 7-item scoring system that evaluates the inflammatory activity of thyroid eye disease1). A score of 3 or more out of 7 indicates active disease and is an indication for medical treatment.
The EUGOGO (European Group on Graves’ Orbitopathy) severity classification categorizes the disease into three stages: mild, moderate-to-severe, and sight-threatening 8). Sight-threatening refers to compressive optic neuropathy or corneal ulceration and requires urgent intervention.
TSH receptors (TSHR) present on fibroblasts in the retrobulbar tissues of the orbit act as antigens, promoting lymphocyte infiltration into orbital tissues, activating macrophages, and triggering an inflammatory response through a local cytokine network. This leads to an increase in orbital volume, resulting in proptosis, elevated intraorbital pressure, and compressive optic neuropathy.
The inferior rectus and medial rectus are most frequently affected. The inferior rectus is the most commonly involved extraocular muscle, followed by the medial rectus, superior rectus, and lateral rectus in decreasing order. Therefore, upward gaze impairment is most common, followed by abduction impairment.
Smoking is the greatest risk factor for thyroid eye disease and is associated with the risk of onset, severity, and treatment resistance. In a multicenter study of 633 eyes of 386 patients, smoking rates ranged widely from 16.2% to 71.1% across institutions. Although smoking exacerbates the severity of eye disease, it did not significantly affect the reduction in proptosis after decompression surgery 4).
The diagnosis is established when any of the thyroid-related autoantibodies are positive. The measured targets are TSH receptor antibody (TRAb), thyroid-stimulating antibody (TSAb), anti-thyroglobulin antibody (TgAb), and anti-thyroid peroxidase antibody (TPOAb). Even if thyroid function is normal, testing should be performed if there are findings of proptosis, eyelid retraction, or diplopia.
Proptosis is measured using a Hertel exophthalmometer. The normal range in Japanese individuals is 10–15 mm (mean 13 mm); values exceeding this are considered proptosis. A difference of 2 mm or less between eyes is normal. It is routinely used for preoperative and postoperative evaluation.
MRI (first choice): T1-weighted images evaluate the morphology of the extraocular muscles. STIR (short-TI inversion recovery) sequences depict inflammatory sites as high-signal areas, which is useful for assessing inflammatory activity. Coronal sections are essential because they allow simultaneous evaluation of all extraocular muscles except the inferior oblique.
CT: Confirms thickening of the extraocular muscles (tendon thickening is mild, while the muscle belly is thickened, resulting in a fusiform shape overall). Bone window CT is used to evaluate the orbital walls and for surgical planning. Measurement of the orbital cross-sectional area (coronal CT cross-sectional area approximately 1.5 cm anterior to the superior orbital fissure) before decompression surgery is used to predict postoperative changes in proptosis4).
It is a 7-item scoring system (0–7 points) that evaluates inflammatory activity in thyroid eye disease1). The seven items are: ① spontaneous retrobulbar pain, ② pain on eye movement, ③ eyelid redness, ④ conjunctival injection, ⑤ conjunctival edema, ⑥ caruncular swelling, and ⑦ eyelid edema, each scored 1 point. A score of 3 or more indicates the active phase. It is an important clinical indicator used to determine inflammatory activity and the indication for steroid pulse therapy.
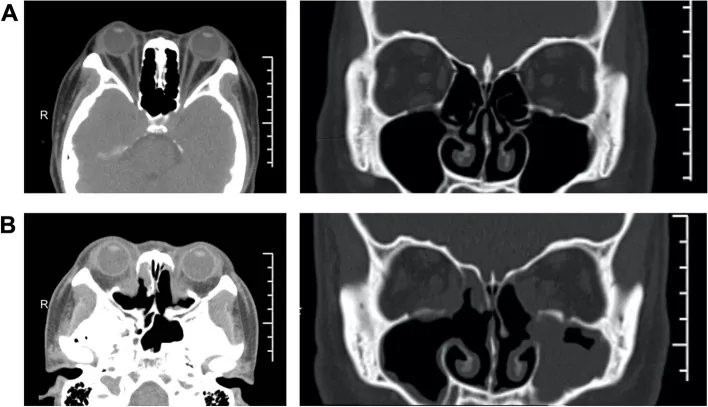
Ye Y, Hu F, Ji Y, et al. The outcomes of endoscopic orbital decompression combined with fat decompression for thyroid-associated ophthalmopathy. BMC Ophthalmol. 2023;23:217. Figure 5. PMCID: PMC10186627. DOI: 10.1186/s12886-023-02957-7. License: CC BY 4.0.
Axial CT of a patient with thyroid eye disease: preoperative (A) shows bilateral proptosis and crowding of the orbital apex with preservation of the medial wall; postoperative (B) shows removal of the posterior medial wall, expansion of the orbital cavity, and marked recession of proptosis. This corresponds to the bony orbital decompression (medial wall removal) for orbital volume expansion discussed in section “5. Standard Treatment”.
If hyperthyroidism is present, normalization of thyroid hormones is an essential prerequisite, and close collaboration with an endocrinology department is required. Surgery is planned after the inflammation has subsided and the Rundle curve has entered a stable (non-inflammatory) phase. The order of procedures is orbital decompression → strabismus surgery → eyelid surgery, and this order must be strictly followed because the results of the preceding surgery directly affect the subsequent surgical plan.
Steroid pulse therapy (first-line): Methylprednisolone 500–1,000 mg/day for 3 days is administered as one course. After 2–3 courses at one-week intervals depending on symptoms, the dose is tapered via intravenous infusion or oral administration.
Local steroid injection: Steroid injection is performed under the Tenon’s capsule around the hypertrophied extraocular muscles. For upper eyelid edema and eyelid retraction due to inflammation, local injection of triamcinolone acetonide (Kenacort-A® 1 ampule) is effective.
Radiation therapy: Indicated when steroid therapy cannot be performed or in cases of recurrence. Irradiation of 1.5–2.0 Gy/day to the retrobulbar tissue is given for 10 days.
Teprotumumab (IGF-1R antibody): A biologic agent reported to significantly improve proptosis overseas 5). It inhibits the IGF-1 receptor and suppresses activation of orbital fibroblasts. Currently not approved in Japan and is considered an investigational treatment option.
Based on the combination of orbital wall resection and fat removal, the procedures are mainly classified into five types. The reduction in proptosis by surgical type from a multicenter study (7 surgeons) of 633 eyes is as follows 4).
Surgical technique
Number of walls
Proptosis reduction (mean)
Medial wall only
1 wall
1.4–2.3 mm
Fat + lateral wall
2 walls
2.9–3.6 mm
Medial wall + inferior wall
2 walls
2.6–3.7 mm
Fat + lateral wall + medial wall
3 walls
3.1–3.9 mm
Fat + lateral wall + medial wall + inferior wall
3 walls + fat
4.6–5.0 mm (maximum effect)
The amount of proptosis reduction increases with the number of walls resected. Graded decompression according to severity is a basic principle of surgical selection 2)6), and the surgical approach is also determined by whether the goal is cosmetic or optic nerve protection. It has been statistically significantly shown that the higher the preoperative proptosis, the greater the postoperative improvement (p < 0.001) 4).
After strabismus stabilizes following decompression
3
Eyelid surgery
Performed last
Strabismus surgery: For strabismus that has become fixed in the chronic phase, surgery mainly involves recession of thickened rectus muscles. New diplopia may occur after orbital decompression, so surgical planning should be done after strabismus has stabilized.
Eyelid surgery: For eyelid retraction, if due to inflammation, local injection of triamcinolone acetonide is performed. For fixed eyelid retraction in the non-inflammatory stable phase, recession correction surgery (Müller muscle resection or levator aponeurosis recession) is performed.
QHow much does orbital decompression improve proptosis?
A
It varies by surgical technique. One-wall decompression (medial wall only) can reduce proptosis by 1.4–2.3 mm, and three-wall plus fat decompression (maximal procedure) can reduce it by 4.6–5.0 mm4). The effect increases with the number of walls decompressed, and the greater the preoperative proptosis, the larger the postoperative improvement. Graded decompression according to severity is recommended6).
TSH receptors present in fibroblasts of retrobulbar orbital tissues act as antigens, promoting lymphocyte infiltration into orbital tissues, activating macrophages, and activating inflammatory responses through local cytokine networks. Inflammatory cytokines (IL-1, IL-6, TNF-α) are produced, and orbital volume increases progressively.
Changes in adipose tissue: Enlargement of adipocytes and lymphocytic infiltration of the interstitium occur, with edema and scar formation due to chronic inflammation. Increased synthesis of glycosaminoglycans (GAG) and hyaluronic acid causes fluid retention and swelling of the tissue.
Changes in extraocular muscles: Lymphocyte-predominant inflammatory cell infiltration is seen between striated muscle fibers, and muscle fibers undergo degeneration and necrosis. Edema and thickening due to inflammation occur in the interstitium, connective tissue proliferates between muscle fibers, and extraocular muscle hypertrophy develops. On CT/MRI, tendon thickening is mild, and the muscle belly is enlarged, giving a fusiform shape overall.
Increased orbital pressure due to increased orbital volume and thickening of extraocular muscles compress the optic nerve at the orbital apex. Positive RAPD, decreased CFF, and visual field defects are signs. This mechanism provides the rationale for orbital decompression surgery (orbital volume expansion) to relieve optic nerve compression.
IGF-1 receptor (IGF-1R) forms a complex with TSHR on orbital fibroblasts and synergistically participates in the activation of orbital fibroblasts 5). Blockade of this complex signal is the mechanism of action of teprotumumab and is the theoretical basis for the therapeutic outcome of proptosis reduction overseas.
Removing the orbital wall eliminates the bony septum between the orbit and adjacent paranasal sinuses (ethmoid, maxillary, sphenoid), allowing orbital fat to herniate into the sinuses and expanding orbital volume. This reduces intraorbital pressure and moves the eye posteriorly. Combining fat removal can further enhance the decompression effect.
In a multicenter retrospective study by Hong et al. (2025) involving 7 institutions, 7 surgeons, and 633 eyes, it was confirmed that there was no significant difference in the amount of proptosis reduction between surgeons when the same surgical technique was performed 4) (standard error 0.14–0.56 mm). The reproducibility of standardized surgical techniques demonstrated at a multicenter level is an important finding supporting the statistical validity of multicenter RCTs.
Furthermore, preoperative proptosis was shown to be the most significant factor predicting postoperative change in proptosis (p<0.001), reaffirming the importance of preoperative assessment4).
The same study also examined the effect of approach method for each surgical technique. For medial wall plus floor decompression, the endoscopic group showed significantly greater reduction in proptosis than the open surgery group (-3.67mm vs -2.97mm, p=0.008). On the other hand, for fat plus lateral wall plus medial wall decompression, there was no significant difference between endoscopic and open surgery4).
Teprotumumab (IGF-1R antibody) is a biologic agent reported to significantly improve proptosis overseas5). Although not yet approved in Japan, it is internationally positioned as a drug therapy for active moderate-to-severe thyroid eye disease. Long-term safety (hearing impairment, hyperglycemia, etc.) is being monitored through Phase IV trial results.
Predictive Model for Postoperative New-Onset Diplopia
A model predicting the occurrence of new-onset diplopia after decompression surgery has been developed7), and it is expected to be used in preoperative counseling and surgical planning.
Smoking is the greatest risk factor exacerbating the severity of thyroid eye disease, but in the study of 633 eyes, smoking did not significantly affect the degree of proptosis reduction after decompression surgery4). The role of smoking in predicting treatment outcomes is being refined.
Mourits MP, Prummel MF, Wiersinga WM, Koornneef L. Clinical activity score as a guide in the management of patients with Graves’ ophthalmopathy. Clinical endocrinology. 1997;47(1):9-14. doi:10.1046/j.1365-2265.1997.2331047.x. PMID:9302365.
European Group on Graves’ Orbitopathy (EUGOGO), Mourits MP, Bijl H, Altea MA, Baldeschi L, Boboridis K, et al. Outcome of orbital decompression for disfiguring proptosis in patients with Graves’ orbitopathy using various surgical procedures. The British journal of ophthalmology. 2009;93(11):1518-23. doi:10.1136/bjo.2008.149302. PMID:19028743.
Bahn RS, Heufelder AE. Pathogenesis of Graves’ ophthalmopathy. The New England journal of medicine. 1993;329(20):1468-75. doi:10.1056/NEJM199311113292007. PMID:8413459.
Hong A, Shoji MK, Villatoro GA, Radha-Saseendrakumar B, Baxter SL, Dolman PJ, et al. Intersurgeon Variability in Proptosis Reduction After Orbital Decompression for Thyroid Eye Disease: A Multicenter Analysis. Ophthalmic plastic and reconstructive surgery. 2026;42(3):318-324. doi:10.1097/IOP.0000000000003090. PMID:41082925.
Rootman DB. Orbital decompression for thyroid eye disease. Surv Ophthalmol. 2018;63:86-104. doi:10.1016/j.survophthal.2017.03.007.
Kikkawa DO, Pornpanich K, Cruz RC Jr, Levi L, Granet DB. Graded orbital decompression based on severity of proptosis. Ophthalmology. 2002;109(7):1219-1224. doi:10.1016/S0161-6420(02)01068-0.
Nair AA, Ediriwickrema LS, Dolman PJ, et al. Predictive modeling of new-onset postoperative diplopia following orbital decompression for thyroid eye disease. Ophthalmic Plast Reconstr Surg. 2022;38(6):551-557. PMID:35551414. doi:10.1097/IOP.0000000000002196.
Bartalena L, Kahaly GJ, Baldeschi L, et al. The 2021 European Group on Graves’ orbitopathy (EUGOGO) clinical practice guidelines for the medical management of Graves’ orbitopathy. Eur J Endocrinol. 2021;185(4):G43-G67. doi:10.1530/EJE-21-0479. PMID:34297684.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.