Oculodermal melanocytosis (ODM) is a benign dermal melanocytosis that occurs in the distribution of the first (ophthalmic) and second (maxillary) branches of the trigeminal nerve. Also called nevus of Ota, it presents as bluish-gray to brown pigmentation of the skin, sclera, and uvea. It is classified as one of the phakomatoses.
First reported by Ota and Tanino in 1939, they proposed a classification into four subtypes based on the extent of skin involvement: orbital, zygomatic, frontal, and alar types; moderate type; severe type; and bilateral type 1).
It is a congenital, non-hereditary nevus, but pigmentation may intensify during puberty, pregnancy, or with aging 1). 90% are unilateral, and ocular involvement is seen in about 66% of cases 1). The female-to-male ratio is 5:1, suggesting a possible role of hormonal stimulation 1).
The incidence in Asians is 1–2 per 1,000 people 1). It is rare in Caucasians, but Caucasian patients have the highest risk of developing malignant melanoma associated with this condition. It is most common in Japanese individuals, but has also been reported in Indians and Caucasians.
QIs nevus of Ota hereditary?
A
It is a congenital nevus but not hereditary. It is often present at birth, but may newly appear or intensify during puberty or pregnancy 1). Familial occurrence is rare.
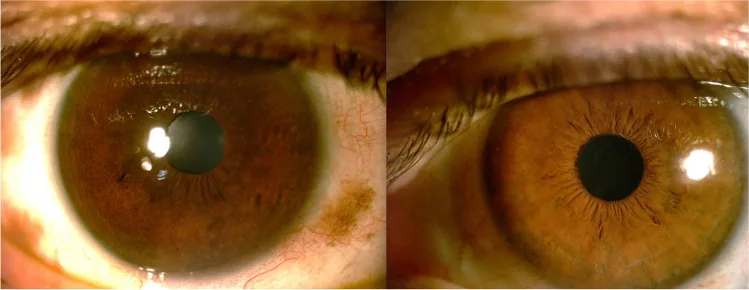
Solmaz Abdolrahimzadeh, Damiano Maria Pugi, Priscilla Manni, Clemente Maria Iodice, et al. An update on ophthalmological perspectives in oculodermal melanocytosis (Nevus of Ota) 2022 Jul 19 Graefes Arch Clin Exp Ophthalmol. 2023 Jul 19; 261(2):291-301 Figure 3. PMCID: PMC9837000. License: CC BY.
Slit-lamp images of both eyes show bluish-gray pigmentation of the sclera and conjunctiva. The left eye also shows a darker iris color, indicating ocular pigmentation associated with Nevus of Ota.
Nevus of Ota is usually asymptomatic. The main reason for consultation is cosmetic concerns due to facial skin pigmentation. If glaucoma is present, visual field defects may be noticed.
Pigmented spots: Flat, bluish-gray to brown pigmented macules in the trigeminal V1/V2 distribution. The color varies with depth: darker in superficial layers and lighter in deeper layers.
Distribution: Involves the eyelids, forehead, cheeks, nasal alae, and temporal region. Unilateral in 90% of cases 1).
Palatal mucosa: Rarely, pigmentation may be seen on the palate.
Ocular Findings
Episcleral and scleral pigmentation: The most common finding. Predominantly in the superotemporal quadrant, also seen inferonasally 1).
Iris heterochromia: The iris on the affected side is darker than the unaffected side. May be accompanied by iris mammillations (small pigmented uniform nodules) 1).
Fundus: The choroid on the affected side is darker than the unaffected side, and pigmented spots may be observed 1).
In conjunctival pigmentation, conjunctival melanosis (pigmentation within the conjunctival epithelium) is mobile, whereas congenital ocular melanocytosis including nevus of Ota is immobile because it is pigmentation in the deep subconjunctival to episcleral layers. The presence or absence of mobility is an important point for differentiation.
Iris mammillations are associated with elevated intraocular pressure and predisposition to intraocular melanoma, so differentiation from Lisch nodules in neurofibromatosis type 1 is necessary 1). Lisch nodules are distinguished by their pleomorphism, lighter color, and bilaterality 1).
Nevus of Ota is thought to occur when melanoblasts derived from the neural crest fail to migrate normally via the dorsolateral pathway to the epidermal basal layer during the 2nd to 8th week of gestation and remain in the upper dermis 1).
The major complication risks of nevus of Ota are shown below.
Risk
Frequency/Features
Glaucoma
Approximately 10% of patients 1)
Uveal melanoma
1/400 in Caucasians 1)
Melanoma metastasis
2-fold risk in ODM-complicated cases1)
ODM is observed up to 35 times more frequently in patients with uveal melanoma and is also a risk factor for bilateral, multiple atypical melanomas1).
QWhat is the probability of nevus of Ota transforming into malignant melanoma?
A
In Caucasian patients, about 1 in 400 develop uveal melanoma in their lifetime1). Furthermore, uveal melanoma with ODM has a 2-fold increased risk of metastasis compared to cases without ODM1). Early detection through regular eye exams is important.
The diagnosis of nevus of Ota is based on clinical findings. It is clinically diagnosed by characteristic skin pigmentation in the trigeminal V1/V2 distribution and pigmentation of the sclera and iris. Multifaceted examinations are needed to evaluate ocular complications.
Anterior segment OCT (ASOCT): Enables quantitative assessment of cross-sectional images of the angle, iris, and anterior chamber. However, it has limitations in evaluating deep pigmented lesions1)
Dilated fundus examination: Evaluates the degree of choroidal pigmentation, optic disc cupping, and presence of melanoma1)
Fundus autofluorescence (FAF): Useful for differentiating choroidal nevus from melanoma. Melanoma shows plaque-like hyperautofluorescence due to lipofuscin deposition1)
EDI-SDOCT: Enables detailed cross-sectional evaluation of the choroid. In affected eyes, choroidal thickness increases by 23% and perivascular interstitial tissue increases by 51%1)
Ultrasonography (A/B scan): Basic method for evaluating tumor size and morphology. Melanoma shows low to medium reflectivity on A-scan and dome-shaped or mushroom-shaped appearance on B-scan1)
In addition, differentiation from conjunctival nevus (localized, dark brown, well-defined borders) and benign acquired conjunctival melanosis (PAM: appears after middle age, unilateral patchy pigmentation) is also important. PAM with atypia requires histopathological diagnosis because approximately 50% become malignant within 5 years.
QHow often should I have eye examinations?
A
For early detection of glaucoma and malignant melanoma, slit-lamp microscopy and dilated fundus examination every 6 months are recommended 1). Even if intraocular pressure is normal, open-angle glaucoma can develop, so regular follow-up is important.
Nevus of Ota itself is a benign condition, and active treatment is not necessary if asymptomatic. Treatment targets are complications (glaucoma, malignant melanoma) and cosmetic skin pigmentation.
Ophthalmic Treatment
Glaucoma treatment: Prostaglandin analogs and alpha agonists are first-line. Beta-blockers and carbonic anhydrase inhibitors are second-line 1).
Melanoma surveillance: Regular screening with slit-lamp examination and dilated fundus examination every 6 months is mandatory 1).
Dermatological Treatment
Q-switched laser: The most effective treatment for skin pigmentation. Short pulses reduce the side effect of post-inflammatory hyperpigmentation 1).
Q-switched Alexandrite laser: 755 nm, energy density 4.75–7.0 J/cm², administered at 8–12 week intervals. Improvement is seen in 50% of cases after an average of 2 sessions.
Others: Camouflage creams and chemical peels can also make pigmentation less noticeable.
Approximately 50% of patients with uveal melanoma develop metastases within 15 years of diagnosis, so early detection and treatment are directly linked to prognosis 1).
The following procedures have been reported for cosmetic purposes 1).
Scleral allograft overlay: Good cosmetic results with minimal complications
Superficial sclerectomy: Short surgical time and smooth scleral bed
Flipped scleral flap surgery: Utilizes the characteristic that the superficial sclera is more pigmented than the deep layer, but complete removal is difficult
QCan laser treatment remove skin pigmentation of nevus of Ota?
A
The Q-switched alexandrite laser is most effective, with 50% of participants showing clinical improvement after an average of two treatments. Five out of seven patients achieved complete clearance after an average of five treatments, with no recurrence, scarring, or post-inflammatory pigmentary changes observed.
Nevus of Ota results from developmental abnormalities of neural crest-derived melanoblasts. During embryogenesis, melanoblasts migrate from the neural crest via the dorsolateral pathway to the epidermal basal layer; disruption of this process leads to melanocyte arrest in the upper dermis 1). Melanin produced by these arrested melanocytes is observed as bluish-gray to brown pigmentation.
The color depends on the depth of pigment. Superficial melanocytes appear brown, while deeper ones appear blue due to light scattering (Tyndall effect) 1).
Open-angle glaucoma occurs when abnormal accumulation of melanocytes extends to the trabecular meshwork and Schlemm’s canal, mechanically obstructing aqueous humor outflow 1). Glaucoma develops ipsilateral to pigmentation and is observed in about 10% of patients 1). Unlike glaucoma associated with pigment dispersion syndrome, which is usually bilateral, glaucoma associated with ODM is typically unilateral, which is useful for differentiation 1).
Somatic activating mutations in GNAQ are recognized as a common molecular basis for ODM and uveal melanoma. This mutation activates the GTPase RAS pathway, enhancing cell proliferation signals 1). BAP1 mutations are involved in metastatic tumor progression, and co-occurrence with GNAQ mutations is a poor prognostic factor 1).
7. Latest Research and Future Perspectives (Preliminary Reports)
Abdolrahimzadeh et al. (2023) reported that the combination of EDI-SDOCT and fundus autofluorescence has complementary value to conventional ultrasonography in differentiating choroidal nevi from small melanomas. EDI-SDOCT enables diagnosis of submillimeter choroidal melanomas that are difficult to detect with ultrasound, and can capture subtle changes such as subretinal fluid, shaggy photoreceptors, and RPE abnormalities 1).
OCT angiography (OCTA) noninvasively visualizes retinal and choroidal microvasculature and is useful for evaluating microvascular structures in melanoma. Quantitative assessment of FAZ enlargement and choroidal neovascularization is becoming possible 1).
Pan et al. (2019) reported an association between mutations in the FAM111B and DSC2 genes and tumor development in genomic analysis of three Chinese patients with choroidal melanoma complicated by ODM 1).
Mularoni et al. (2021) reported ASOCT-guided surgery in which the depth of scleral pigmentation is measured preoperatively with ASOCT, and superficial sclerectomy is performed at an accurate depth using a calibrated diamond blade. This is expected to reduce the risk of intraoperative scleral thinning 1).
Abdolrahimzadeh S, Pugi DM, Manni P, Iodice CM, Di Tizio F, Persechino F, et al. An update on ophthalmological perspectives in oculodermal melanocytosis (Nevus of Ota). Graefe’s archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2023;261(2):291-301. doi:10.1007/s00417-022-05743-1. PMID:35851619; PMCID:PMC9837000.
Plateroti AM, Scavella V, Abdolrahimzadeh B, Plateroti R, Rahimi S. An Update on Oculodermal Melanocytosis and Rare Associated Conditions. Semin Ophthalmol. 2017;32(4):524-528. PMID: 27083007.
Teekhasaenee C, Ritch R, Rutnin U, Leelawongs N. Ocular findings in oculodermal melanocytosis. Arch Ophthalmol. 1990;108(8):1114-20. PMID: 2383200.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.