Scleral contact lenses are rigid gas permeable (RGP) lenses with a diameter larger than the cornea, fitting on the sclera (over the conjunctiva). The lens vaults over the entire cornea and rests on the sclera and overlying conjunctival tissue. Before insertion, the bowl of the lens is filled with preservative-free saline, creating a fluid reservoir between the back surface of the lens and the front surface of the cornea4). The key feature is that the lens does not touch the cornea at all, masking corneal irregularities while continuously lubricating and protecting the ocular surface4).
They cause less foreign body sensation than regular hard contact lenses (HCL) and are useful for correcting corneal irregularities. The space enclosed by the corneal surface and the lens is filled with saline or tears, protecting the entire corneal surface from dryness and friction.
Scleral lenses are classified into the following four types by diameter.
Classification
Diameter
Characteristics
Corneo-scleral
12.9–13.5 mm
Small diameter covering cornea and limbus
Semi-scleral
13.6–14.9 mm
Intermediate type with minimal limbal extension
Mini-scleral
15.0–18.0 mm
Most commonly used standard type
Large-scleral
18.1–24.0 mm
Large diameter for severe ocular surface disease
In classification based on HVID, lenses within HVID + 6 mm are sometimes called mini-scleral lenses, and those exceeding 6 mm are called full scleral lenses.
Three-zone structure of the lens
Optical zone: The central part covering the cornea, including refractive power and base curve. The diameter is usually 9–10 mm.
Limbus/Transition Zone: The transition between the optical zone and the landing zone, providing clearance over the corneal limbus. It is important for protecting limbal stem cells.
Landing Zone/Haptic Zone: The area that rests on the scleral and conjunctival anatomy, where spherical or toric designs are selected.
Features of PROSE Treatment
FDA Approval: First approved in 1994 and updated in 2016. Uses custom prosthetic devices with diameters of 13–23 mm.
CAD/CAM Design: Enables seamless curvature design using spline functions, with specifications possible for up to eight independent meridians 1).
Advanced Customization: Allows precise placement of SmartChannels (fluid ventilation grooves) and fenestrations (perforations) to accommodate complex ocular surface shapes 1).
PROSE devices are manufactured from fluorosilicone acrylate polymer, with oxygen permeability (Dk) selectable from a range of 85 to 180 1). High Dk materials are used in cases with corneal endothelial dysfunction. While commercially available scleral lenses are typically limited to customization of 2–4 meridians, PROSE devices allow independent control of up to 8 meridians 1).
Scleral lenses can be prescribed as a self-pay treatment at some specialized facilities and are used to treat severe dry eye due to ocular pemphigoid or Stevens-Johnson syndrome. The BostonSight PROSE device itself is a treatment model provided at BostonSight clinics and network facilities in the United States.
QHow do PROSE devices differ from commercially available scleral lenses?
A
Commercially available scleral lenses are typically limited to customization of 2–4 meridians, whereas PROSE devices allow specification for up to eight independent meridians 1). Features include seamless curvature design using spline functions, precise placement of SmartChannels (fluid ventilation grooves) and fenestrations (perforations), and other advanced customizations 1). Additionally, PROSE treatment incorporates a 6-month fitting period and rigorous patient training, achieving high compatibility for severe corneal diseases 1).
The main subjective symptoms indicating the use of scleral lenses are as follows.
Decreased visual acuity due to irregular astigmatism is the most common indication, targeting cases where glasses or soft contact lenses do not provide adequate correction 5). In severe keratoconus, uncorrected visual acuity may drop to counting fingers (CF) 2).
Dryness, pain, and photophobia associated with dry eye are also important indications. Severe cases with an OSDI (Ocular Surface Disease Index) score reaching 95.83 have been reported 3). Discomfort and visual loss due to exposure keratopathy are seen in neuromuscular diseases such as CPEO (chronic progressive external ophthalmoplegia) 3).
Symptoms of corneal damage associated with contact lens (CL) wear may include foreign body sensation, discomfort, discharge, redness, eye pain, tearing, blurred vision, and decreased vision. If redness, discharge, and pain all appear, corneal infection is possible and caution is needed.
In the evaluation of corneal irregularity, the Kmax value (69.3 D in severe keratoconus) and thinnest corneal thickness (336 μm) on Pentacam corneal tomography are important indicators 2).
In the evaluation of ocular surface damage, the Oxford staining score (3.0/5.0) indicates the degree of ocular surface injury 3). Corneal opacity, neovascularization, and epithelial plaques are findings seen in ocular surface diseases such as KID syndrome 1). Slit-lamp examination is essential for confirming CL-related corneal damage, and fluorescein staining is useful for determining the pattern of epithelial defects.
Indications for scleral lenses are broadly divided into “visual impairment due to corneal irregularity” and “ocular surface disease.”
Corneal ectasia (keratoconus, keratoglobus, post-LASIK ectasia, pellucid marginal degeneration) is a major cause of irregular astigmatism5). In advanced keratoconus, management with scleral lenses can be an alternative to corneal transplantation 2). In a study of 846 eyes, only 1.65% required corneal transplantation after scleral lens use 2). Residual irregular astigmatism after corneal transplantation or radial keratotomy (RK) is also an indication 5).
Exposure keratopathy can result from lagophthalmos and incomplete blinking associated with CPEO 3). Even in cases where conventional surgical interventions such as frontalis suspension are ineffective, scleral lenses can be a useful option 3).
KID syndrome (Keratitis-Ichthyosis-Deafness syndrome) is a rare ectodermal dysplasia caused by GJB2 gene mutations, leading to corneal neovascularization, opacity, and epithelial plaques 1). Conventional surgical interventions (corneal transplantation, limbal transplantation, etc.) are reported to have low success rates 1).
QAre scleral lenses or PROSE available in Japan?
A
Scleral contact lenses can be prescribed as self-funded treatment at some specialized facilities, and are used for severe dry eye conditions such as ocular cicatricial pemphigoid and Stevens-Johnson syndrome. The BostonSight PROSE device itself is a treatment model provided at BostonSight clinics and network facilities in the United States, and direct provision of this device is not available in Japan. Commercially available scleral lenses, which are large-diameter rigid gas permeable lenses, are used instead.
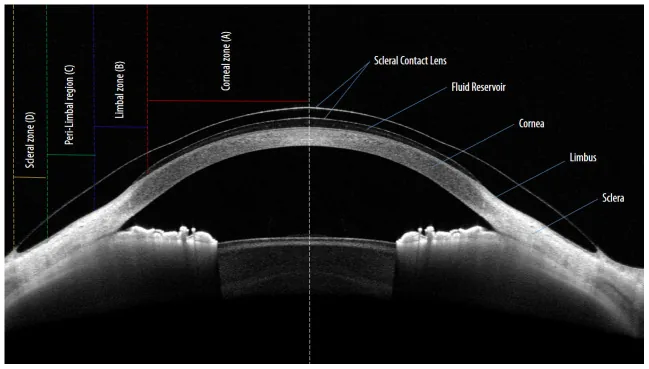
Kumar P, Carrasquillo KG, Chaudhary S, et al. A multi-parameter grading system for optimal fitting of scleral contact lenses. F1000Res. 2022;11:6. Figure 1. PMID: 35136587; PMCID: PMC8802154; DOI: 10.12688/f1000research.74638.2. License: CC BY 4.0.
An anterior segment OCT (AS-OCT) cross-sectional image clearly shows the scleral contact lens vaulting over the entire cornea, with a fluid reservoir formed between the posterior lens surface and the anterior corneal surface. This corresponds to the AS-OCT corneal clearance measurement and four-zone (corneal zone, limbal zone, perilimbal zone, scleral zone) evaluation discussed in the section “4. Diagnosis and Examination Methods.”
Comprehensive evaluation of corneal shape and ocular surface is essential for scleral lens fitting.
Examination
Purpose
Pentacam corneal tomography
Evaluation of corneal curvature, thickness, and keratoconus morphology 2)
Quantitative evaluation of subjective symptoms3)4)
Oxford staining score
Assessment of ocular surface damage3)
Slit-lamp microscopy + fluorescein staining
Fitting evaluation and confirmation of CL-related corneal disorders
Pentacam corneal tomography is particularly useful for evaluating severe keratoconus, with Kmax value, thinnest corneal thickness, and anterior/posterior elevation maps guiding lens selection2). Corneal tomography visualizes irregularity and toricity of the entire cornea, providing information not obtainable with simple keratometry2).
AS-OCT allows cross-sectional evaluation of corneal clearance, limbal clearance, and lens edge profile during wear2)3). Generally, a corneal clearance of 200–500 μm is considered appropriate. Since clearance decreases by approximately 100–150 μm a few hours after insertion due to sinking into conjunctival tissue, this change must be considered in initial settings.
Corneal endothelial cell density is an essential pre-wear assessment item; below 1000 cells/mm², the risk of corneal edema due to reduced oxygen permeability increases3).
Fluorescein pattern evaluation with a slit-lamp microscope is fundamental for fitting, confirming corneal clearance, limbal clearance, and alignment of the bearing zone2). Slit-lamp microscopy is also essential for monitoring CL-related disorders, used to determine epithelial defect patterns and assess signs of infection.
In cases with severe corneal edema or scarring, fitting soft contact lenses or RGP lenses may be difficult, and scleral lenses are also useful for visual acuity assessment6). Over-refraction with scleral lenses allows more accurate evaluation of visual potential before surgery6).
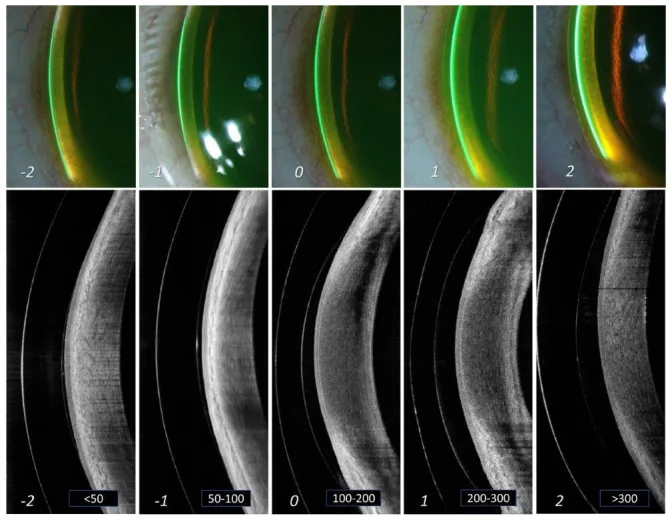
Kumar P, Carrasquillo KG, Chaudhary S, et al. A multi-parameter grading system for optimal fitting of scleral contact lenses. F1000Res. 2022;11:6. Figure 3. PMID: 35136587; PMCID: PMC8802154; DOI: 10.12688/f1000research.74638.2. License: CC BY 4.0.
The upper row shows a 5-grade slit-lamp microscopic grading (−2 to +2) of the scleral lens limbal bearing zone, and the lower row shows corresponding AS-OCT cross-sectional images with tear reservoir thickness (<50 μm to >300 μm) displayed numerically within white frames. This corresponds to the fitting evaluation and limbal clearance management discussed in the section “5. Standard Treatment.”
Fitting begins with diagnostic trial lenses 2). The total lens diameter is initially set as the horizontal visible iris diameter (HVID) plus 4 mm 2). Fluorescein pattern, clearance measurement by AS-OCT, and over-refraction are repeated to pursue the optimal design 2).
The combination of high Dk material (Dk 141–180) and low center thickness (CT 0.30–0.35 mm) maximizes oxygen supply to the cornea1)3). If oxygen permeability is insufficient, management with lens removal and refresh every 3–5 hours is recommended 3).
SmartChannels are radial grooves on the posterior haptic surface that promote tear exchange and reduce suction pressure under the lens 1). Fenestration (perforation) involves creating small holes of 0.25–0.50 mm in diameter in the lens to enhance oxygenation through air ventilation. It is used in cases with corneal edema or significant corneal endothelial dysfunction.
The space under the lens is filled with saline (or artificial tears if there is an allergy). Care must be taken to avoid air bubbles during insertion. Because the lens is larger in diameter than regular HCLs, a dedicated insertion/removal tool (plunger/suction cup) is used. Instruction in the examination room is necessary until the patient becomes proficient in wearing.
The basics of care are cleaning and rinsing, but disinfection is also recommended due to the complex shape of the lens.
In a 34-year-old male with severe keratoconus (Amsler-Krumeich Grade 4, Kmax 69.3D), a mini-scleral lens (16 mm) achieved improvement from counting fingers uncorrected visual acuity (UCVA) to best-corrected visual acuity (BCVA) of 20/30 2).
AS-OCT confirmed good fitting with corneal clearance of 278 μm 2). Surgery was avoided even in cases where other optical corrections were unsuccessful 2).
Exposure Keratopathy (CPEO)
In a 69-year-old female with CPEO, frontalis suspension surgery was ineffective and exposure keratopathy persisted 3).
With scleral lens (16.4 mm) wear, best-corrected visual acuity improved from 6/12 to 6/7.5, and the OSDI score dramatically decreased from 95.83 to 4.17 3). The Oxford staining score also improved from 3.0 to less than 1, and stability was maintained for 4 years 3).
KID Syndrome
With PROSE wear, regression of corneal epithelial plaques and improvement of corneal opacity and neovascularization were observed 1). In an adult case, disappearance of recurrent corneal erosion and stabilization of the ocular surface were maintained for 7 years 1).
If lens wear is discontinued, corneal plaques recur, so continuous use is important 1).
For dry eye disease, improvement in visual acuity and OSDI scores with scleral lenses has been reported in patients with severe dry eye due to underlying conditions such as Stevens-Johnson syndrome, Sjögren’s syndrome, and chronic ocular GVHD 4). Decreases in fluorescein/lissamine green staining scores of the cornea and conjunctiva and tear osmolarity have also been confirmed 4). Scleral lenses are considered effective and well-tolerated for severe dry eye4).
The fluid reservoir of scleral lenses is also utilized as a drug delivery modality. Improvement in corneal neovascularization and visual acuity has been reported with concomitant injection of bevacizumab (anti-VEGF drug) into the reservoir, and filling the reservoir with cyclosporine 0.05% has also been attempted 4).
QWhat is midday fogging?
A
Midday fogging is a phenomenon in which debris such as lipids and proteins accumulate in the tear fluid reservoir during scleral lens wear, causing visual blurring during the day 4). Because the fluid reservoir between the lens and cornea has limited tear exchange, debris tends to accumulate. Countermeasures include promoting tear exchange by adding SmartChannels, ensuring proper alignment of the landing zone, and refreshing the lens every few hours.
The use of scleral lenses has been reported to reduce the rate of corneal transplantation 5). Even in keratoconus cases that were unsuccessful with RGP lenses, good fitting was achieved in all cases with scleral lenses, avoiding corneal transplantation 5). Scleral lenses may also be used after corneal transplantation as a means of visual recovery for irregular astigmatism2).
Corneal transplantation carries risks such as graft rejection, infection, high astigmatism, and a long recovery period 2). In cases of severe keratoconus that can be managed with scleral lenses, the ability to avoid these surgical risks is a major advantage 2).
QCan corneal transplantation be avoided with scleral lenses?
A
Even in advanced keratoconus, if sufficient visual improvement is obtained with scleral lenses, corneal transplantation may be avoided 2)5). In a study of 846 eyes, only 1.65% of the scleral lens group required corneal transplantation 2). However, corneal transplantation may be necessary if corneal opacity, corneal edema, or contact lens intolerance is present. Scleral lenses may also be useful for residual irregular astigmatism after corneal transplantation 2).
The therapeutic mechanism of scleral lenses lies in completely avoiding direct contact with the cornea.
Elimination of mechanical irritation: While conventional HCLs slide over the cornea, scleral lenses do not touch the cornea at all, thus no mechanical irritation occurs. Stable wear is possible even in cases with irregular corneal shape.
Optical correction by the fluid reservoir: The saline or tear fluid in the lens reservoir fills the irregularities of the anterior corneal surface, forming a stable optical surface. This corrects high irregular astigmatism.
Continuous wetting of the ocular surface: The fluid reservoir keeps the corneal surface constantly moist, suppressing corneal epithelial damage due to dryness. In severe dry eye disease, this protective effect directly contributes to disease control.
Protection of limbal stem cells: The transition zone of the three-zone structure ensures clearance over the limbus, avoiding direct pressure on limbal stem cells. This is an important consideration in cases with limbal stem cell deficiency (LSCD).
Multifaceted protection for dry eye: In ocular surface disease, both corneal dryness and friction promote epithelial damage. Scleral lenses exert therapeutic effects by simultaneously protecting against both factors.
Research is underway to utilize the fluid reservoir of scleral lenses as a drug delivery platform 4). Improvement of corneal neovascularization by filling the reservoir with bevacizumab (anti-VEGF drug) and application of cyclosporine 0.05% for dry eye treatment have been reported 4).
The mechanisms of corneal plaque regression and neovascularization improvement in KID syndrome remain largely unclear, and further research is awaited 1).
The usefulness of scleral lenses for neuromuscular diseases such as CPEO is also attracting attention, and from both aspects of eyelid elevation effect (MRD improvement) and ocular surface protection, they are becoming established as a treatment alternative to conventional surgical intervention 3).
Although evidence on optimal fitting of scleral lenses is accumulating, high-quality comparative studies supporting their use in dry eye management are still lacking 4). Long-term prospective studies using patient-reported outcomes (OSDI, NEI VFQ-25, etc.) are expected in the future 2).
Gagliardi M, Asghari B. Two cases of therapeutic scleral lenses for KID syndrome. American journal of ophthalmology case reports. 2025;37:102261. doi:10.1016/j.ajoc.2025.102261. PMID:39927073; PMCID:PMC11804770.
Almaweri A. Avoiding Surgery: Successful Management of a Patient With Severe Keratoconus Using Scleral Contact Lenses. Cureus. 2025;17(8):e90263. doi:10.7759/cureus.90263. PMID:40964594; PMCID:PMC12438945.
Erdinest N, Shemesh N, London N, Landau D, Lavy I. Chronic Progressive External Ophthalmoplegia (CPEO): Rehabilitation utilizing scleral contact lenses. American journal of ophthalmology case reports. 2025;39:102411. doi:10.1016/j.ajoc.2025.102411. PMID:41017819; PMCID:PMC12460078.
Tear Film & Ocular Surface Society. TFOS DEWS III Management and Therapy Report. Am J Ophthalmol. 2025;279:72-178.
Jhanji V, Ahmad S, Amescua G, et al. Corneal Ectasia Preferred Practice Pattern. Ophthalmology. 2024 Apr;131(4):P205-P246. doi:10.1016/j.ophtha.2023.12.038. PMID:38349299.
AAO Cornea/External Disease PPP Panel. Corneal Edema and Opacification Preferred Practice Pattern. San Francisco: American Academy of Ophthalmology; 2024.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.