Ocular toxocariasis (OT) is a zoonotic infectious disease caused by the hematogenous invasion of larvae of the dog roundworm (Toxocara canis) or cat roundworm (Toxocara cati) into the eye. It is also called ocular larva migrans (OLM). It was first reported in 1950 by Wilder as nematode endophthalmitis3).
Toxocariasis has two main clinical forms. Visceral larva migrans (VLM) is a systemic infection with fever, hepatomegaly, and eosinophilia, while ocular toxocariasis (OT) is limited to the eye. It is very rare for both to occur simultaneously. The average age of onset is 15–30 months for VLM and 7.5 years for ocular toxocariasis.
Toxocariasis accounts for approximately 1.1% of cases of infectious uveitis5). The seroprevalence of Toxocara antibodies in the United States is estimated at about 13.9%1). However, symptomatic ocular toxocariasis is rare, with only 68 new cases reported in the US over a 12-month period from 2009 to 20101). The median age at diagnosis was 8.5 years, and 68% of patients developed permanent visual impairment1). In Southeast Asia, seroprevalence has been reported to reach 34%2).
QCan ocular toxocariasis occur in adults?
A
Most cases occur in children, but adult-onset cases have also been reported. In adults, a history of contact with dogs or cats and consumption of raw meat are risk factors, and diagnosis is often delayed due to low clinical suspicion1). A literature review includes case reports ranging from 17 to 68 years of age1).
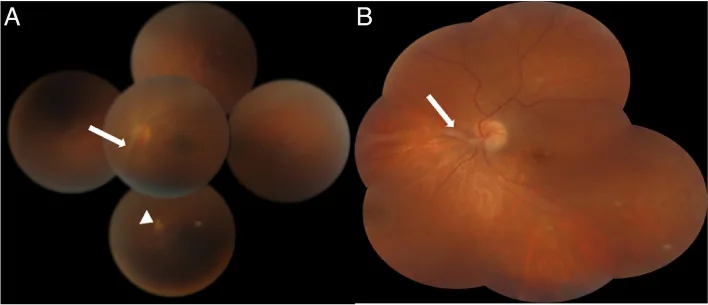
Maamouri R, et al. Peripheral retinal cysts in presumed ocular toxocariasis. J Ophthalmic Inflamm Infect. 2023. Figure 1. PMCID: PMC10397159. License: CC BY.
Wide-angle fundus montage shows white vitreoretinal traction bands extending from the periphery toward the optic disc. In A, peripheral chorioretinal scars are also seen, representing typical posterior segment inflammatory findings of ocular toxocariasis.
Ocular toxocariasis progresses slowly and may have few subjective symptoms other than visual loss.
Visual loss: The most common complaint, presenting as progressive unilateral visual loss. Visual acuity ranges from 20/40 to 20/400 depending on the disease type.
Floaters: Appear when vitreous inflammation is present.
Photophobia (sensitivity to light): This is a symptom associated with uveitis.
White pupil: In infants, a white pupil or strabismus may be the first sign. Amblyopia and strabismus are particularly common in young children with the posterior pole granuloma type.
Ocular toxocariasis is unilateral in approximately 90% of cases and is classified into the following three clinical types.
Posterior pole granuloma
Frequency: Accounts for 25–46% of all cases.
Findings: A white to gray elevated granuloma forms in the macula. Its size ranges from 0.5 to 4 times the optic disc diameter. It is often accompanied by epiretinal membrane formation.
Course: In the acute phase, it appears as a white lesion with indistinct borders accompanied by vitritis, and after inflammation subsides, it becomes a well-defined white elevation.
Visual prognosis: The median visual acuity is around 20/50.
Peripheral granuloma
Frequency: The most common type, accounting for 20–40%.
Findings: A yellowish-white tumor forms in the peripheral fundus, from which vitreous strands and retinal folds extend toward the posterior pole. Traction on the optic disc and macular displacement are observed.
Complications: Tractional retinal detachment and macular displacement are frequently associated, making this the most severe disease type.
Visual prognosis: The median visual acuity is around 20/70.
Endophthalmitis type
Frequency: Accounts for approximately 25%.
Findings: Presents with diffuse inflammation involving both the anterior and posterior segments, characterized by dense vitreous opacities.
Features: Almost always unilateral, requiring differentiation from bacterial endophthalmitis.
Visual prognosis: Median visual acuity is worst, ranging from 20/200 to 20/400.
Vitreitis is observed in over 90% of patients and is the most common finding. Other complications may include retinal perivasculitis 4), cystoid macular edema, epiretinal membrane, and cataracts. 80–90% of visual acuity loss is 20/40 or worse, primarily caused by vitreitis, cystoid macular edema, and tractional retinal detachment3). Tractional retinal detachment occurs in 20–40% of the peripheral granulomatous type; surgery improves vision in more than half of cases, but reoperation is often required.
Ocular toxocariasis is caused by infection with the dog roundworm (Toxocara canis) or the cat roundworm (Toxocara cati). These roundworms parasitize the intestines of dogs and cats and shed eggs in their feces. Dogs and foxes are endemically infected, and infection can also occur by consuming raw liver of paratenic hosts such as chickens and cattle.
The main routes of infection in humans are as follows.
Oral ingestion of eggs: Ingesting eggs while playing in contaminated soil or sandboxes. Pica (soil eating) in children is an important risk factor.
Contact with pets: Close contact with infected dogs or cats, especially puppies. In puppies aged 2–6 months, the prevalence of Toxocara canis exceeds 80%.
Ingestion of raw meat: Infection can also occur through consumption of raw liver from paratenic hosts such as chickens and cattle.
Inquiry about contact with pets and consumption of raw meat is useful for diagnosis. Antibody positivity rates of 20–80% have been reported in young children, indicating frequent actual exposure, but most cases are asymptomatic.
Young age: Common in children under 10 years old. Associated with playing in sandboxes and immature hygiene awareness.
Pet ownership: Especially owning young dogs with inadequate deworming1)4).
Pica: Toddlers with a habit of putting soil in their mouths.
Low income and education level: An association between seropositivity and low household income and education level has been reported1).
QWill I definitely get infected if I own a pet dog?
A
Simply owning a dog does not guarantee infection. Regular deworming and proper hygiene management can reduce the risk. In dogs aged 1 year or older, the prevalence of Toxocara canis is about 20%. However, puppies have a high rate of carrying the parasite, so special caution is needed.
The diagnosis of ocular toxocariasis is made comprehensively by combining clinical findings, medical history, and serological tests. The uveitis clinical practice guidelines recommend diagnosis based on characteristic fundus findings combined with serum antibody positivity against Toxocara larval-specific antigens 5).
A detailed history of contact with pets (dogs and cats), pica, and consumption of raw meat should be obtained. More than 90% of patients have an identifiable exposure history.
ELISA: ELISA using Toxocara excretory-secretory (TES) antigens is the most useful test. For visceral larva migrans, sensitivity is 90% and specificity is 92%, but for ocular toxocariasis, sensitivity is significantly lower 1). In one study (N=22), ELISA was positive in only 50% of cases.
Toxocara CHECK®: A simple test kit used in Japan.
ELISA of intraocular samples: Even if serum ELISA is negative, ELISA of aqueous humor or vitreous may be positive, providing high diagnostic value 1).
Goldmann-Witmer coefficient: Evaluates intraocular production of anti-Toxocara antibodies in the aqueous humor.
PCR test: Detection of Toxocara DNA from aqueous humor also provides diagnostic evidence.
B-mode ultrasound: Confirms vitreous opacity, retinal detachment, and a mass without calcification. This is important for differentiating from retinoblastoma3). If calcification is present, suspect retinoblastoma; if a non-calcified mass with inflammatory findings is present, suspect ocular toxocariasis.
Unlike visceral larva migrans, ocular toxocariasis often does not show peripheral blood eosinophilia or elevated IgE. Even if eosinophil count is normal, this disease cannot be ruled out1). In children, polyclonal IgE elevation may be observed. Confirmation of serum anti-Toxocara antibodies (especially elevated IgM) is useful.
Differentiation from the following diseases is necessary.
Retinoblastoma: The most important differential diagnosis. If calcification is observed on ultrasound, retinoblastoma is strongly suspected.
Coats disease: Characterized by dilation of retinal blood vessels and exudative changes.
Toxoplasmosis: Presents with necrotizing retinochoroiditis and characteristic scar lesions. If focal necrotizing retinal vasculitis is present, fungal retinochoroiditis should also be considered.
QIs it possible to have ocular toxocariasis even if eosinophils are normal on blood test?
A
Yes. Ocular toxocariasis is a local ocular infection, and unlike visceral larva migrans, it generally does not cause peripheral blood eosinophilia1). Even if eosinophils are within the normal range, this disease should not be ruled out.
Treatment of ocular toxocariasis is based on three pillars: suppression of inflammation, elimination of the causative microorganism, and management of vitreoretinal complications.
Corticosteroids are the mainstay of treatment. For endophthalmitis type or posterior/peripheral granuloma type with severe vitritis, local injection (sub-Tenon triamcinolone acetonide 40 mg) 2) or oral prednisolone (0.5–1 mg/kg/day) is administered.
Local injection/systemic administration: Performed for severe inflammation.
Topical steroid eye drops: Used to prevent formation of tractional membranes and retinal detachment.
Mydriatic agents: In cases of anterior segment inflammation, cycloplegic agents are used together to prevent posterior synechiae.
The efficacy of anthelmintic drugs in ocular toxocariasis has not been well established. Granulomas containing live larvae often have mild inflammation, and treatment may not be necessary. However, use is considered in the following cases.
Albendazole: The standard regimen is 400 mg twice daily for 14 days1). It has high blood-brain barrier permeability and is also used when neurotoxocariasis needs to be excluded3). In children, it is administered at 15 mg/kg/day3)4).
Diethylcarbamazine citrate (Supatonin®): Oral administration as an anthelmintic may be performed. It is used in combination with steroids to reduce inflammation caused by the parasite. Opinions on its efficacy vary in the literature.
In rare cases where ocular toxocariasis occurs simultaneously with VLM, systemic administration of albendazole along with steroids is necessary.
Approximately 25% of ocular toxocariasis cases require surgery.
Pars plana vitrectomy (PPV): This is the most common surgical treatment for persistent vitreous opacities, tractional retinal detachment, and epiretinal membranes 3)4). During surgery, because the membranes are very adherent, it is important to perform circumcision rather than peeling or stripping. The anatomical success rate of modern vitrectomy is 83–100%.
Cryocoagulation: This is performed for peripheral mass-type lesions that are resistant to medical treatment and have formed vitreous strands, to prevent progression of tractional retinal detachment. It is important to apply sufficient freezing to the entire mass, aiming to form a coagulative scar.
Laser photocoagulation: This may be performed for posterior pole mass-type lesions that do not involve the fovea. However, there is a risk of severe inflammatory reaction due to larval death. It is contraindicated for cysts in the endophthalmitis type.
87% of patients requiring surgery had visual acuity less than 20/400 preoperatively, and despite anatomical success, functional improvement is often limited. Visual acuity at initial presentation is the strongest predictor of final visual acuity. Young children with posterior pole granuloma may develop visual field defects or macular folds, leading to decreased vision or amblyopia, and the need for amblyopia treatment (such as occlusion therapy) should be considered.
QWill vision recover with treatment?
A
Prognosis depends largely on the disease type, presence of complications, and timing of treatment initiation. The median visual acuity is 20/50 for posterior pole granuloma, 20/70 for peripheral granuloma, and 20/200 to 20/400 for endophthalmitis type. Cases without secondary complications follow a favorable course, but those with tractional retinal detachment may not achieve visual improvement even after surgery. Early diagnosis is most important.
Dogs and cats are definitive hosts; adult worms parasitize the intestinal tract and shed eggs. Eggs mature into embryonated eggs in the environment over 2–4 weeks and become infective.
When humans ingest embryonated eggs, larvae hatch in the intestine. The larvae penetrate the intestinal wall and disseminate hematogenously throughout the body, potentially reaching multiple organs such as the liver, lungs, brain, muscles, and eyes1). Larvae that reach the eye invade the posterior segment and trigger a local inflammatory response. VLM and ocular toxocariasis rarely occur in the same patient, presenting different clinical pictures depending on the site of infection.
The host forms eosinophilic granulomas to encapsulate larvae that have invaded the eye. Histologically, non-necrotizing giant cell granulomas are characteristic, accompanied by a mixed inflammatory infiltrate of plasma cells and eosinophils 3).
Melendez et al. (2025) reported early ocular toxocariasis in a 5-year-old girl. Histological analysis of a macular epiretinal granuloma revealed a non-necrotizing giant cell granuloma within a fibrous nodule, with a mixed inflammatory infiltrate of plasma cells and eosinophils. No worm was detected 3).
Persistent inflammation leads to the formation of vitreous bands and traction on the retina. This traction causes tractional retinal detachment. The formation of vitreous fibrovascular bands from a peripheral granuloma toward the optic disc is a characteristic finding of this disease 3)4).
Furthermore, when a retinal tear forms, it can lead to rhegmatogenous retinal detachment3). It should be noted that even if vitreous strands are not clinically apparent in the early stages, retinal tears can occur due to traction at the base of the granuloma 3).
There are reports on the safety and efficacy of intravitreal dexamethasone sustained-release implants in ocular toxocariasis 3). In cases with severe vitritis where the macula is not involved, this approach is being considered as a means to achieve high local steroid concentrations while avoiding systemic administration.
Intravitreal administration of anti-VEGF agents (ranibizumab, bevacizumab) has been reported at the case report level for ocular toxocariasis complicated by choroidal neovascularization or macular edema4). It is considered promising for controlling vascular leakage and neovascularization associated with chronic inflammation, but it is not a substitute for antiparasitic therapy.
Tanchuling et al. (2025) reported a 16-year-old male with ankylosing spondylitis and ocular toxocariasis presenting with bilateral panuveitis. Both Toxocara IgG and HLA-B27 were positive, suggesting that infection may contribute to the development of autoimmune diseases through immune abnormalities2).
Regarding the association between parasitic infection and autoimmune diseases, it has been reported that the positivity rate of Toxocara antibodies reaches 38% in ankylosing spondylitis patients with uveitis2), highlighting the role of infection as a common basis for immune abnormalities.
Jowsey GW, McLeod GX.. A delayed diagnosis of ocular toxocariasis presenting as total monocular retinal detachment in an immunocompetent 57-year-old male. IDCases. 2023;32:e01764. doi:10.1016/j.idcr.2023.e01764. PMID:37122593; PMCID:PMC10130852.
Tanchuling RV, Lopez JS, Maliwat RD.. Coexistent Ankylosing Spondylitis and Ocular Toxocariasis in a Pediatric Patient Manifesting As Bilateral Panuveitis. Cureus. 2025;17(4):e82767. doi:10.7759/cureus.82767. PMID:40406765; PMCID:PMC12096418.
Melendez AM, Puebla Robles GA, Marcos Martinez MJ, Villegas VM, Singh AD.. Early-stage ocular toxocariasis: Progression and histopathologic analysis. Am J Ophthalmol Case Rep. 2025;40:102474. doi:10.1016/j.ajoc.2025.102474. PMID:41323766; PMCID:PMC12661507.
El Korno O, Hilali Z, Tachfouti S, Amazouzi A, Cherkaoui LO.. Unilateral Vision Loss in a Child Revealing Ocular Toxocariasis. Cureus. 2025;17(12):e99150. doi:10.7759/cureus.99150. PMID:41531620; PMCID:PMC12795621.