Ocular syphilis is a condition in which Treponema pallidum subsp. pallidum infects ocular tissues, causing intraocular inflammation. Any ocular structure can be affected, and because of its diverse clinical presentations, it is called “the great imitator.” Treatment follows the guidelines for neurosyphilis.
Globally, 5.7 to 6 million new syphilis infections are reported annually among individuals aged 15–49 years 1). Ocular involvement occurs in approximately 0.6–2% of all syphilis cases 1)2). A study in North Carolina found ocular syphilis in 63 of 4,232 cases (1.5%), of which 38% were diagnosed during primary or secondary syphilis 1). In recent years, the incidence has been increasing, particularly among MSM and patients with HIV co-infection. In Japan, the prevalence decreased markedly after the introduction of penicillin, but cases are rising again.
The disease was first named by Girolamo Fracastoro in 1530 in his work “Syphilis sive Morbus Gallicus,” and the spirochetal etiology was discovered by Fritz Schaudinn and Erich Hoffmann in 1905 1).
QAt what stage of syphilis does ocular syphilis occur?
A
Ocular syphilis can occur at any stage of syphilis, including primary, secondary, tertiary, and latent stages. In some cases, ocular symptoms are the first indication of syphilis. Therefore, syphilis should always be considered in cases of uveitis of unknown cause.
Demographic, Clinical and Laboratory Characteristics of Ocular Syphilis: 6-Years Case Series Study From an Eye Center in East-China. Front Immunol. 2022 Jun 10; 13:910337. Figure 3. PMCID: PMC9226556. License: CC BY.
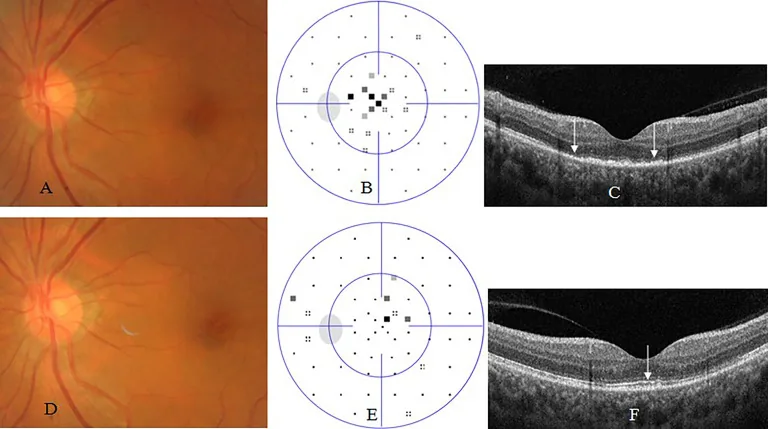
Acute occult outer retinopathy -like syphilic retinitis. A 54-year old woman complained of blurred vision in the left eye for 2 weeks. At presentation, his left eye had visual acuity of 20/40, clear anterior segment and normal fundus (A), small central scotoma on visual field test (B), and disruption or loss of outer segments of macular retina (arrow, C) on OCT. Two months after antibiotic therapy, her visual acuity recovered to 20/20 in the left eye, with normal fundus (D), nearly normal visual field test (E), and nearly complete recovery of outer segments of macular retina (arrow, F).
The findings of ocular syphilis vary depending on the affected site.
Anterior Segment
Conjunctiva: Chancre in the first stage, mild conjunctivitis in the second stage, and gumma in the third stage.
Sclera: Episcleritis (common in the second stage), scleritis (common in the third stage). Nodular or diffuse.
Syphilitic interstitial keratitis: Immune-mediated non-ulcerative, non-suppurative interstitial keratitis. Neovascularization → leaves ghost vessels. Responds to steroids but not to penicillin alone. One of the Hutchinson triad of congenital syphilis (permanent tooth M-shaped defect, sensorineural hearing loss, interstitial keratitis).
Uvea and Posterior Segment
Uveitis: Can be anterior, posterior, or panuveitis. Granulomatous or non-granulomatous. In a report of 24 cases by Barile and Flynn, granulomatous iridocyclitis was the most common (46%) 1).
ASPPC (Acute Syphilitic Posterior Placoid Chorioretinitis): Reported in patients with secondary syphilis. Disc-shaped, yellow lesions at the RPE level in the macula to peripapillary area. OCT shows disruption and hyperreflective elevation of the outer retina and RPE. Responds well to antibiotic treatment.
Optic neuritis: Unilateral or bilateral. Anterior or retrobulbar optic neuritis, papilledema, neuroretinitis, optic atrophy. Optic nerve involvement is seen in 12–78% of ocular syphilis cases 3).
Argyll Robertson pupil: Miosis, loss of light reflex but preserved near reflex. Common in tertiary stage but can appear early.
Ocular motor abnormalities: In tertiary stage, caused by superior orbital fissure syndrome, brainstem infarction, or compression by aneurysm.
HIV co-infection: Increases the risk of ocular syphilis by approximately 2-fold1). It tends to be bilateral and more often involves the posterior segment. Prevalence increases with CD4 count <200 cells/ml and viral load >200 copies/ml.
It occurs through transplacental infection. Early congenital syphilis presents with chorioretinitis. Late congenital syphilis is characterized by Hutchinson’s triad (notched permanent incisors, sensorineural hearing loss, interstitial keratitis). In Japan, late-onset cases are rare because the disease is detected and treated early in infancy.
QIf diagnosed with syphilis, is HIV testing also necessary?
A
HIV co-infection is an important risk factor for ocular syphilis, and HIV testing is recommended for all patients at the time of syphilis diagnosis. In HIV-positive individuals, the severity of uveitis increases and it tends to become bilateral, altering the clinical presentation. Additionally, in AIDS, serological tests may be false negative, which requires attention 1).
In Japanese clinical practice, the following two types of tests are combined.
Type of Test
Representative Test
Purpose
Non-treponemal test (STS)
RPR, VDRL
Infection screening and treatment efficacy evaluation
Treponemal test (TP antigen method)
TPHA, FTA-ABS, TP-PA
Specific confirmatory diagnosis
Activity assessment: RPR ≥16-fold and TPHA ≥1,280-fold → high activity.
Treatment efficacy assessment: RPR ≤8-fold or decreased to ≤1/4 of initial value → effective anti-syphilitic treatment.
Prozone phenomenon: High titers may cause false-negative non-treponemal tests (dilution testing required).
Reverse sequence algorithm (CDC recommended): First perform treponemal test (EIA/CLIA) → if positive, then non-treponemal test. Advantageous for detecting early cases1). For discordant results (treponemal positive, non-treponemal negative), retest with TP-PA.
In ocular syphilis, CSF examination is recommended to assess for neurosyphilis4). However, the CDC 2021 guidelines state that if isolated ocular symptoms, confirmed ocular abnormalities, and positive treponemal test are all present, CSF examination before treatment is not mandatory3).
CSF-VDRL: High specificity but low sensitivity.
CSF FTA-ABS: High sensitivity but low specificity.
Sawacillin tablets (250 mg) 4 tablets 4 times daily for 4 weeks.
Neurosyphilis and ocular syphilis (inpatient intravenous therapy):
In syphilitic uveitis, neurosyphilis is often complicated, and high-dose intravenous penicillin therapy according to CDC guidelines is standard.
Aqueous crystalline penicillin G: 1,800,000–2,400,000 units/day (300,000–400,000 units IV every 4 hours or continuous infusion) for 10–14 days2)3)5)1).
Alternative regimen: Procaine penicillin G 2.4 million units intramuscularly once daily + Probenecid 500 mg orally four times daily for 10–14 days2)1).
In a 46-year-old male reported by Nwaobi et al. (2023), neurosyphilis treatment with IV PCG 4 million units q4h was administered for ocular syphilis with RPR 1:64 and TPHA 1:512, and visual acuity recovered after 6 months2).
Refer to the trend of RPR (lipoidal antigen test). A decrease in antibody titer to ≤8-fold or ≤1/4 of the initial value is considered evidence of effective antisyphilitic treatment.
Penicillin desensitization is recommended first 1)7).
Ceftriaxone: 1–2 g IM or IV once daily for 14 days 1)6).
Doxycycline: 200 mg/day (100 mg twice daily) for 28 days 1)7).
Cubelo et al. (2022) reported that a 24-year-old HIV-positive man with PCG allergy received doxycycline 100 mg BID for 14 days, and his RPR decreased from 1:1,024 to 1:32 7). PCG desensitization was subsequently performed.
It occurs as a reaction to inflammatory lipoproteins derived from dead Treponema pallidum within 24 hours of starting treatment.
Symptoms: Fever, headache, myalgia. Occurs in 30–70% of early syphilis and 2% of neurosyphilis 1).
Ocular symptoms: Decreased vision, macular edema, optic disc swelling, and cotton-wool spots have been reported.
Management: Continue treatment. Use antipyretics and analgesics for symptomatic relief.
QHow is it treated if there is a penicillin allergy?
A
Penicillin desensitization is recommended first. If this is difficult, alternatives include ceftriaxone (1–2 g once daily for 14 days) or doxycycline (200 mg/day for 28 days) 1)7). However, evidence for these in ocular syphilis is limited compared to penicillin.
QShould treatment be stopped if a Jarisch-Herxheimer reaction occurs?
A
Treatment should be continued without interruption. Systemic symptoms such as fever and headache are managed symptomatically with antipyretics and analgesics. Ocular symptoms (including vision loss and optic disc swelling) are usually temporary and improve with continued treatment.
Chancre: Painless induration at the inoculation site. Disappears in about 4 weeks. May occur on the conjunctiva or around the eye.
Secondary Stage
Timing: 4 to 10 weeks after the appearance of the chancre.
Systemic dissemination: Hematogenous spread affects the nerves, eyes, digestive tract, and liver. The eye is involved in about 10% of cases. Maculopapular rash on the palms and soles is seen in over 70% of cases.
Ocular findings: Mainly uveitis, retinitis, and optic neuritis.
Latent Stage
Classification: Early (within 1 year) and late (after 1 year).
Course: About 1/3 of untreated cases progress to the tertiary stage. Ocular syphilis may become apparent even without symptoms.
Tertiary Stage
Cardiovascular: Aortitis, aortic aneurysm.
Neurosyphilis: Meningeal syphilis, meningovascular syphilis, tabes dorsalis, general paresis.
Treponema pallidum induces production of IL-1β, IL-6, IL-12, and TNF-α via TLR2/TLR4/TLR5-dependent signaling, causing tissue damage similar to delayed-type hypersensitivity 1). CD4+ cells and macrophages dominate primary lesions, while CD8+ cells dominate secondary lesions. IFN-γ production activates and recruits macrophages.
Treponema pallidum has slow growth and the ability to invade immune-privileged tissues such as the eye, CNS, and placenta 1). Apoptosis of CD4+ cells via the Fas-associated death pathway leads to incomplete immune clearance, establishing chronic infection.
In HIV-positive patients, progression to ocular syphilis after the secondary stage is accelerated. Bilateral involvement is more frequent in HIV-positive patients (62%) compared to HIV-negative patients (38%) (study of 96 cases)1). In AIDS, serological tests may be false-negative, requiring caution in diagnosis.
7. Latest Research and Future Perspectives (Research Stage Reports)
iCNV associated with ocular syphilis is an extremely rare condition. In the report by Świerczyńska et al. (2021), approximately one-third of cases achieved disease stability after a single intravitreal injection of aflibercept, and about two-thirds achieved visual stability after two injections 6).
The same report included cases treated with ceftriaxone 2 g/day IV for 14 days due to penicillin allergy. iCNV did not resolve with antibiotic therapy alone, and additional intravitreal anti-VEGF injections were effective 6).
Typically, syphilitic retinal vasculitis is more commonly arteritic or mixed, but cases with predominant phlebitis have been reported in HIV-coinfected patients.
Mammo et al. (2022) reported a case of a 53-year-old HIV-positive male with panuveitis predominantly involving phlebitis, treated with IV PCG 4 million units for 14 days × 2 courses 9). After treatment, it progressed to paravenous pigmentary retinopathy. The findings were similar to PPRCA but lacked bone-spicule pigmentation.
Improved diagnostic accuracy with multimodal imaging
The combination of EDI-OCT, ultra-widefield autofluorescence (FAF), and ICG is expected to improve diagnostic accuracy for ocular syphilis3)1). ICG detects choroidal dark dots, hot spots, and blurred choroidal vessels. Accumulation of these multimodal imaging findings may contribute to differentiation from sarcoidosis and tuberculosis.
Chauhan K, Bhatt DL, Bhardwaj P, et al. Demystifying Ocular Syphilis – A Major Review. Ocul Immunol Inflamm. 2023. DOI:10.1080/09273948.2023.2217246.
Nwaobi S, Nwaobi A, Karunakaran K, et al. Through the Eyes: A Case of Ocular Syphilis. Cureus. 2023;15(11):e48XXX. PMC10694475.
Kayabai M, Doğan R, Kaçar İ, et al. Presentation of Ocular Syphilis with Bilateral Optic Neuropathy: A Rare Case Report. Neuro-Ophthalmology. 2023. PMC10732629.
Fekri S, Golabdar M, Rahimi M, et al. The First Reported Case of Ocular Syphilis in an Iranian Patient Presenting with Intermediate Uveitis. J Ophthalmic Vis Res. 2023. PMC10794801.
Das P, Chakraborty PP, Mondal SK, et al. Ocular syphilis in antibiotic era: A review with case series. Indian J Sex Transm Dis AIDS. 2025. PMC12716672.
Świerczyńska MP, Nowak M, Michalak J, et al. Choroidal neovascularization secondary to ocular syphilis treated with intravitreal aflibercept. Rom J Ophthalmol. 2021;65(4). PMC8764425.
Cubelo M, Almeida MJ, Sobrinho-Simões J, et al. A Case of Ocular Syphilis in an HIV-Positive Patient With Penicillin Allergy. Cureus. 2022;14(9). PMC9574520.
Kiani R, Patel L, Gupta N, et al. Blurry Diagnosis of Ocular Syphilis: A Case Report. Cureus. 2022;14(10). PMC9635406.
Mammo DA, Ober MD, Dansingani KK. Ocular Syphilis With Phlebitis and Paravenous Pigmentary Retinopathy. J VitreoRetinal Dis. 2022. PMC9954775.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.