Progressive outer retinal necrosis (PORN) is a necrotic herpetic retinitis caused by varicella-zoster virus (VZV), first reported by Forster et al. in 1990. 2) As the name suggests, inflammation begins mainly in the outer retina and rapidly progresses to full-thickness necrosis. It is resistant to treatment and has an extremely poor prognosis.
It commonly occurs in AIDS patients with peripheral blood CD4-positive T-lymphocyte counts ≤50/mm³, but also develops in immunocompromised patients after bone marrow transplantation, with collagen diseases, or malignant lymphoma. 1) Herpes simplex virus (HSV) and cytomegalovirus (CMV) can also be causative agents. VZV is the most common cause, accounting for about 71.5%, followed by HSV.
Acute retinal necrosis (ARN), also caused by VZV, occurs in immunocompetent individuals, whereas PORN is a different disease with severe immunodeficiency as a background, and its clinical features, treatment, and prognosis are fundamentally different. In recent years, similar cases in immunocompetent individuals have been reported, and the concept of an ARN/PORN spectrum has been proposed. 9)
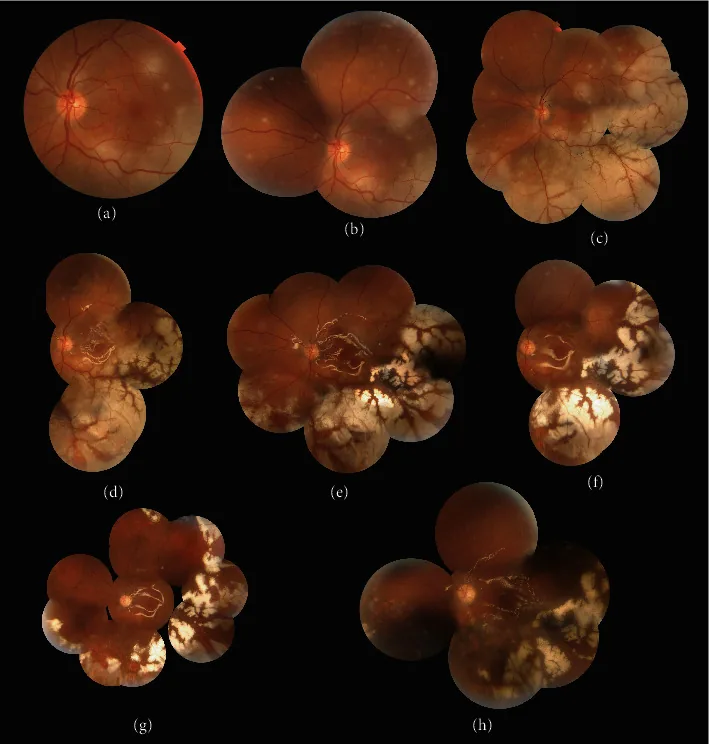
Riazi-Esfahani H, et al. The Role of Early Vitrectomy in the Healing of Retinal Lesions in Progressive Outer Retinal Necrosis. Case Rep Ophthalmol Med. 2022. Figure 2. PMCID: PMC8898816. License: CC BY.
The fundus photograph shows extensive yellow-white necrotic lesions extending from the peripheral retina to the posterior pole. The lesions are coalescing and enlarging, representing typical clinical findings of progressive outer retinal necrosis.
If the lesion affects the macula, it causes decreased visual acuity; when confined to the periphery, it causes visual field narrowing. Herpes zoster often precedes the condition. During the course, almost all cases become bilateral, so visual impairment often becomes severe in the end.
White spots: Multiple isolated white spots appear in the deep retina of the peripheral fundus, rapidly enlarging and coalescing within 1–2 weeks after onset.
Perivascular clearing: A characteristic finding where white spots disappear around blood vessels.
“Cracked mud”-like necrosis: Necrotic foci develop cracks and progress to retinal detachment through multiple holes.
Rapid progression: In severely immunosuppressed stages, it rapidly progresses to posterior pole and full-thickness necrosis without accompanying retinal vasculitis or retinal hemorrhage.
Anterior Segment and Vitreous Findings
Minimal anterior segment inflammation: Mutton-fat keratic precipitates (KP) and anterior chamber cells are almost absent.
Almost no vitritis: Inflammatory findings are markedly less compared to ARN.
Iris adhesion and elevated intraocular pressure are rare
This “paucity of inflammation” is the most important distinguishing point from ARN and requires attention at diagnosis.
QWhat is the biggest difference between ARN and PORN?
A
The biggest difference is the patient’s immune status and the degree of intraocular inflammation. ARN occurs in immunocompetent healthy individuals and is accompanied by severe anterior segment inflammation (mutton-fat KP, anterior chamber cells) and vitritis. PORN occurs in patients with severe immunodeficiency (AIDS: CD4 ≤50/mm³) and has almost no anterior segment or vitreous inflammation, progressing more rapidly and extensively. Additionally, acyclovir is effective for ARN, but for PORN, acyclovir alone is ineffective, and a combination of ganciclovir and foscarnet is required.
The most important risk factor for the development of PORN is severe cellular immunodeficiency. The following conditions are the main risks.
HIV infection/AIDS: CD4-positive T lymphocyte count ≤50/mm³ (most common underlying disease)
After hematopoietic stem cell transplantation or kidney transplantation: Onset during use of immunosuppressive drugs
Malignant lymphoma/leukemia: Immunosuppression due to chemotherapy
Biologics/long-term steroid use: Immunosuppression associated with treatment of collagen diseases/autoimmune diseases
Collagen disease with severe immunosuppression: During active phase or treatment of systemic disease
Uncontrolled diabetes mellitus: Long-term hyperglycemia may contribute to immunosuppression9)
Prior herpes zoster: Skin herpes zoster often precedes, and if there is a history of long-term acyclovir treatment, ACV-resistant VZV may be present1)
The essence of the pathology lies in the lack of immune response due to severe immunodeficiency. In ARN, the host inflammatory response suppresses VZV spread to some extent, but in PORN, the immune response is extremely poor, so the virus is not controlled within the retina and progresses rapidly. In patients with a long history of herpes zoster treatment, acyclovir-resistant VZV may be present. 1)
Extensive retinal yellowish-white lesions centered on the outer retina, extending from the posterior pole to the periphery, with mild retinal hemorrhage and vasculitis
2. Lack of inflammation
Minimal inflammatory findings in the anterior chamber and vitreous
3. Clinical course
Progression over several weeks
4. Systemic condition
Systemic immunosuppressive state
5. Virological testing
Detection of VZV DNA by PCR in aqueous humor or vitreous fluid (detection rate decreases if no inflammatory cells in anterior chamber or during anti-VZV therapy)
6. Blood tests
In AIDS patients, CD4 count is usually ≤50/mm³. In non-AIDS patients, confirm immunocompromised state such as post-organ transplant, malignancy, or collagen disease
Important notes on testing:
PCR detection rate decreases when there are no inflammatory cells in the anterior chamber or during anti-VZV therapy1)
The Q value (Goldmann-Witmer coefficient) is not used for PORN (unlike ARN). In severe immunodeficiency, intraocular antibody production is poor, making measurements unreliable3)
Serum VZV antibody titer has no diagnostic value due to latent VZV infection.
OCT (Optical Coherence Tomography): Can confirm selective destruction/damage pattern of the outer retinal layers. Also useful for differentiation from ARN9)
Brain MRI: Performed to check for concurrent VZV central nervous system infection. May show hyperintense areas in the temporal lobe, etc. 10)
Focal granulomatous retinitis; often adjacent to old scars (satellite lesions).
Intraocular lymphoma
Vitreous cells and subretinal infiltration; middle-aged to elderly; may be associated with brain lesions; confirmed by cytology.
QWhy can't the Q value (antibody titer) test be used for PORN?
A
The Q value (Goldmann-Witmer coefficient) is calculated from the ratio of intraocular antibody production to serum antibody levels, and is a highly reliable test in diseases with strong inflammation such as ARN. However, because PORN develops in a state of severe immunodeficiency, the immune system is barely functional. Since intraocular antibody production itself is poor, calculating the Q value does not yield meaningful results and cannot be used for diagnosis. This is a major difference from ARN (which utilizes PCR and Q value).
No effective treatment has been established. Acyclovir alone is ineffective, and the basic approach is systemic combination therapy with ganciclovir (Denosine) and foscarnet (Foscavir), or systemic administration of one agent plus intravitreal injection of the other. 1)
Drug Therapy Regimen (Combination of two drugs is standard)
Induction: 5 mg/kg twice daily; Maintenance: 5 mg/kg once daily
Foscarnet (Foscavir injection)
Intravenous
Induction: 60 mg/kg three times daily; Maintenance: 90 mg/kg once daily
Intravitreal ganciclovir injection (off-label)
Intravitreal
400 μg/0.1 mL (can be increased up to 2,000 μg) once weekly
Foscarnet intravitreal injection (off-label)
Intravitreal
2,400 μg/0.1 mL; active phase 2 times/week, then 1 time/week
The above two drugs are administered systemically (intravenously), or one drug is given systemically and the other intravitreally. Combining systemic therapy with intravitreal injection increases local concentration and is expected to suppress disease progression. 7)
In HIV-infected cases, initiating or optimizing antiretroviral therapy (ART) to restore CD4 count is the fundamental treatment. For non-AIDS immunodeficiencies (post-organ transplant, biologic use, chemotherapy for malignancy), manage the underlying disease and discuss reduction of immunosuppressive drugs with the primary physician.
Prophylactic laser photocoagulation: May be performed, but its usefulness is not established1)
Vitrectomy: Performed when retinal detachment occurs. Silicone oil tamponade is also an option6)
QWhy is acyclovir alone ineffective?
A
There are two main reasons: ① Many patients have used acyclovir long-term for herpes zoster (VZV), so acyclovir-resistant VZV is likely to have emerged. ② Viruses such as HHV-6, which lack thymidine kinase required for acyclovir action, can also be pathogens. Therefore, it is necessary to combine ganciclovir and foscarnet, which do not depend on thymidine kinase.
PORN develops due to the collapse of immune surveillance against VZV caused by severe cellular immunodeficiency (especially marked decrease in CD4-positive T cells).
VZV infection has been demonstrated in the retina, and herpes simplex virus and CMV can also be causative pathogens. Initially, necrosis is confined to the outer retinal layers, but as the disease progresses, it extends to the full thickness of the retina. In severe immunodeficiency, the immune response is minimal, with weak inflammation in the anterior segment and vitreous, and the virus cannot be contained, leading to a rapid course.
In ARN, the host inflammatory response suppresses viral spread to some extent, observed as anterior segment inflammation, vitritis, and occlusive vasculitis. In contrast, in PORN, the immune response is extremely poor, resulting in almost no inflammation, and the virus spreads unchecked within the retina. This clinical picture of “quiet but rapidly progressing necrosis” is characteristic of PORN. 4)
Outer layer predominance: Initially, the outer retinal layers (photoreceptors and retinal pigment epithelium) are selectively affected. As the disease progresses, full-thickness necrosis occurs. 3)
Mechanism of perivascular clearing: It is thought that cells around blood vessels remain, possibly contributing to blood flow maintenance at the edge of necrosis.
Involvement of ACV-resistant VZV: In patients who have used acyclovir long-term for herpes zoster, resistant mutant VZV is likely to emerge, contributing to acyclovir ineffectiveness.
Involvement of HHV-6: HHV-6 does not possess thymidine kinase, so acyclovir is ineffective. Use of two or more drugs such as ganciclovir or foscarnet is necessary.
Concept of the Acute Retinal Necrosis/PORN Spectrum
Acute retinal necrosis and PORN can be understood as a continuous spectrum. 9) In intermediate immune states (e.g., uncontrolled diabetes, immunocompetent individuals), intermediate clinical features may be observed. Cases with VZV DNA exceeding 1 million copies have been reported to progress to no light perception (NLP). 9)
In HIV-infected patients, initiation and continuation of HAART (highly active antiretroviral therapy) to restore CD4 counts contributes to suppressing PORN progression and improving visual prognosis. Since immune reconstitution inflammatory syndrome (IRIS) may occur, careful timing of combination with antiviral drugs is necessary. 11)
For acyclovir-resistant VZV, the use of foscarnet and cidofovir is being considered. Reports suggest that drug susceptibility testing at facilities capable of resistance testing is desirable for drug selection. 5) Some opinions recommend early switching to foscarnet, especially in patients with a long history of acyclovir treatment.
With the widespread use of antiretroviral therapy (ART), the incidence of ocular opportunistic infections has significantly decreased by maintaining CD4 counts in AIDS patients. However, rapid immune recovery due to ART can cause immune recovery uveitis (IRU). Similar to IRU after CMV retinitis, caution is needed regarding the timing of ART initiation in PORN. 6)
Significance of Early Vitrectomy with Silicone Oil Tamponade
Intravitreal antiviral injections (ganciclovir or foscarnet) in addition to systemic administration have been reported to be useful in suppressing disease progression. Especially in cases difficult to control with systemic therapy alone, intensification of local therapy is considered. 7) PORN has also been reported in pediatric AIDS patients, and the same treatment principles as in adults apply. 8)
Riazi-Esfahani et al. (2022) reported a case of a 33-year-old HIV patient (CD4=42/μL) who underwent PPV with silicone oil tamponade and intravitreal ganciclovir (2 mg) early after onset. 11) At 7 months, BCVA was maintained at 20/60 (right eye) and 20/100 (left eye). With HAART, CD4 improved from 42 to 147/μL. It is suggested that silicone oil may play an antiviral role beyond mechanical support.
Management in Immunocompetent and Non-HIV Immunocompromised Patients
PORN is not exclusive to AIDS patients; it has been recognized to occur in post-transplant, lymphoma, diabetes, and even immunocompetent individuals. 9)10) Establishing optimal treatment strategies for PORN in non-HIV patients is a future challenge.
Forster DJ, Dugel PU, Frangieh GT, Liggett PE, Rao NA.. Rapidly progressive outer retinal necrosis in the acquired immunodeficiency syndrome. Am J Ophthalmol. 1990;110(4):341-348. doi:10.1016/s0002-9394(14)77012-6. PMID:2220967.
Robert E. Engstrom, Gary N. Holland, Todd P. Margolis, Cristina Muccioli, Janette I. Lindley, Rubens Belfort, Simon P. Holland, William H. Johnston, et al. The Progressive Outer Retinal Necrosis Syndrome. Ophthalmology. 1994;101(9):1488-1502. doi:10.1016/s0161-6420(94)31142-0.
Moshfeghi DM, Dugel PU, Marx JL, et al. Pathogenesis of the progressive outer retinal necrosis syndrome. Am J Ophthalmol. 1996;121(1):101-104.
Spaide RF, Martin DF, Teich SA, Katz A, Toth I.. Successful treatment of progressive outer retinal necrosis syndrome. Retina. 1996;16(6):479-487. doi:10.1097/00006982-199616060-00003. PMID:9002130.
Scott IU, Luu KM, Davis JL.. Intravitreal antivirals in the management of patients with acquired immunodeficiency syndrome with progressive outer retinal necrosis. Arch Ophthalmol. 2002;120(9):1219-1222. PMID:12215102.
Purdy KW, Heckenlively JR, Church JA, Keller MA.. Progressive outer retinal necrosis caused by varicella-zoster virus in children with acquired immunodeficiency syndrome. Pediatr Infect Dis J. 2003;22(4):384-386. doi:10.1097/00006454-200304000-00025. PMID:12712978.
Broyles HV, Chau FY, Drenser KA, et al. Two cases of progressive outer retinal necrosis–spectrum disease in immunocompetent patients. Am J Ophthalmol Case Rep. 2021;23:101119.
Sachan A, Arora R, Singh R, et al. Progressive outer retinal necrosis in a 10-year-old child post allogeneic hematopoietic stem cell transplantation for Hodgkin lymphoma. BMJ Case Rep. 2021;14:e238697.
Riazi-Esfahani H, Jafari M, Ahmadraji A, et al. Early pars plana vitrectomy and silicone oil tamponade for progressive outer retinal necrosis: a case report. Case Rep Ophthalmol Med. 2022;2022:7636052.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.