Ophthalmia nodosa is a disease in which setae (hairs) from animals or plants penetrate ocular tissues and cause granulomatous inflammation. The term “nodosa” is Latin for “nodular,” referring to the granulomatous nodules that form around the setae.
The most common cause is caterpillar setae. The pine processionary caterpillar and tussock moth larvae are well-known causative organisms. Additionally, tarantula urticating hairs and plant spines (e.g., cactus) can also be causes.
Based on the depth of ocular penetration and clinical presentation, it is classified into five types (Type I to V). This classification is directly linked to treatment decisions and is therefore clinically very important1).
Cases have been reported worldwide, showing seasonality consistent with the habitat of caterpillars. Onset is concentrated in the spring to summer caterpillar activity period. In Nepal, seasonal hyperacute panuveitis (SHAPU) occurs epidemically due to moth setae 1).
QCan the eyes be affected without direct contact with a caterpillar?
A
Setae can be dispersed by wind, so they can reach the eyes even without direct contact with a caterpillar. The setae of the pine processionary caterpillar are fine and lightweight, and cases of airborne exposure are known. Wearing protective glasses is recommended in environments where caterpillars are present.
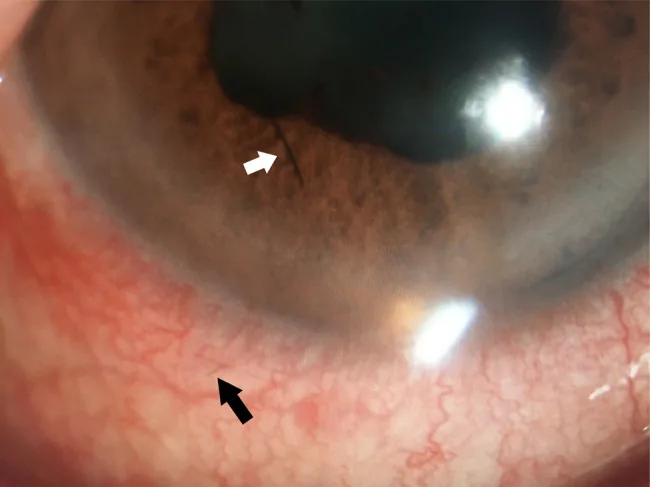
Mingzhe Shi, Shounan Qi, Chenming Wang, Chenguang Wang Case report: Type V ophthalmia nodosa induced by pine processionary caterpillar setae with long-term complications 2025 Nov 28 J Ophthalmic Inflamm Infect. 2025 Nov 28; 16:2 Figure 1. PMCID: PMC12796073. License: CC BY.
White arrows indicate black linear foreign bodies on the iris surface, black arrows indicate subconjunctival black linear foreign bodies. Findings show seta-like foreign bodies penetrating the anterior ocular tissues.
Tamilarsan et al. (2022) reported 4 cases (males aged 18–24) of corneal hair insertion due to insect collision while riding a motorcycle. All cases showed Type III–IV findings, and visual acuity ranged from 6/6 to 6/602).
Zou et al. (2025) reported a severe case in a 12-year-old boy caused by hairs from a tussock moth cocoon. He developed vitreous hemorrhage and tractional retinal detachment 13 months after injury, the most severe Type V case5).
Motorcycle and bicycle riding: Flying insects may collide with the eye during high-speed travel, and setae can become embedded in the cornea. The risk is higher for those not wearing a visor or goggles2)
Children: Direct contact with caterpillars during outdoor play. Cases have been reported in children as young as 2 years old4)
Occupational exposure: Agricultural and forestry workers, gardeners, park maintenance staff
Seasonality: Onset is concentrated during the active period of caterpillars (spring to summer)
QHow should I protect my eyes when riding a motorcycle?
A
The most effective method is to ride with the visor of a full-face helmet closed. Wearing goggles or protective glasses is also recommended. Insect activity is particularly high in the evening and at night, so caution is needed2).
Confirming a history of exposure to caterpillars or insects is most important. Inquire about occupation, outdoor activities, season, and the presence of pets (tarantulas). In children, the exposure history is often unclear4).
The gold standard for diagnosis is direct observation of the hair under a slit-lamp microscope. Multimodal imaging is useful for evaluating deep hairs 1).
SD-OCT: Detailed evaluation of retinal structure. Useful for detecting tractional changes 1)5)
Scheimpflug imaging (Pentacam): Quantitative assessment of corneal shape and opacity
Ashkenazy et al. (2022) performed multimodal imaging combining AS-OCT, B-scan, FA, fundus autofluorescence, and SD-OCT in a Type V case caused by caterpillar setae, demonstrating that the localization of setae and the extent of intraocular inflammation can be assessed noninvasively 1).
Treatment is determined based on the Cadera classification.
Conservative Treatment
Type I (acute conjunctivitis): Removal of setae by irrigation. Combined with topical steroid and antibiotic eye drops.
Type II (chronic granuloma): Removal of setae within the granuloma using forceps. Anti-inflammatory treatment with topical steroids.
Type III (corneal setae): Superficial setae are removed with forceps. Deep setae are observed, and steroid eye drops are used when inflammation occurs 2).
Invasive Treatment
Type IV (anterior chamber setae): Removal of setae by anterior chamber wash 4). Combined with mydriatic and steroid eye drops.
Type V (vitreous/retina): Vitrectomy (PPV) + intraocular foreign body removal. Endolaser or gas tamponade is added as needed 5).
Bandage contact lens: Used to promote epithelial healing after removal of corneal setae 3)
High-dose oral steroids: Even in Type V, some cases can avoid surgery with 2 weeks of oral prednisolone (tapering) 1)
Surgery under general anesthesia: In pediatric cases, anterior chamber irrigation under general anesthesia is required 4)
Levy et al. (2023) reported a 15-year-old girl whose cornea and conjunctiva were penetrated by setae from a white-marked tussock caterpillar. Setae removal and bandage contact lens placement were performed in the operating room, and she healed within 2 weeks 3).
Al Somali et al. (2021) reported a case of a 2-year-old girl with caterpillar setae found in the conjunctiva, cornea, and anterior chamber. Anterior chamber irrigation was performed under general anesthesia, but recurrence occurred 4 months later requiring reoperation. This was the first reported case in the Middle East 4).
QDo setae come out of the body naturally?
A
Due to their barbed structure, setae are not naturally expelled from the body. They tend to migrate deeper into the eye due to body temperature and contraction of surrounding tissues. Even setae on the conjunctival surface may progress into the cornea or anterior chamber over time.
QCan recurrence occur after surgery?
A
Recurrence can occur if tiny setae remain or if setae migrate deeper. In the report by Al Somali et al., recurrence occurred 4 months after initial anterior chamber irrigation, requiring reoperation 4). Regular follow-up is important.
Caterpillar setae are tiny structures about 100–200 μm in length, with barbs on their surface. Due to this barbed structure, they only move in one direction after penetration and do not fall off naturally. Microscopic expansion and contraction of tissues due to body temperature, along with mechanical forces from eyelid and eye movements, gradually push the setae deeper into the eye.
Setae from moth cocoons also have a similar barbed structure and cause intraocular inflammation equivalent to that from larval setae 5).
Inflammation in ocular tissues involves a complex interplay of three mechanisms.
Mechanical irritation: Physical tissue damage caused by the barbed structure of the setae.
Direct toxicity: Pine processionary caterpillars secrete a toxin called thaumetopoein. This toxin induces degranulation of mast cells, triggering an immediate hypersensitivity reaction.
Granulomatous inflammation: Setae are not degraded in the body, leading to a persistent chronic granulomatous reaction centered on foreign body giant cells. This reaction is clinically observed as conjunctival granulomas and iris nodules.
Setae can migrate stepwise from the conjunctiva to the cornea, from the cornea to the anterior chamber, and from the anterior chamber through the iris and ciliary body to the vitreous. This migration occurs over a period of weeks to months4)5).
Zou et al. (2025) reported that tussock moth cocoon setae caused vitreous hemorrhage and tractional retinal detachment 13 months after injury. The lesion, initially Type III, progressed to Type V, representing the most severe course5).
7. Latest Research and Future Perspectives (Investigational Reports)
Ashkenazy et al. (2022) evaluated a Type V moth setae case using an integrated approach with AS-OCT, B-scan, FA, fundus autofluorescence, and SD-OCT. A 45-year-old male maintained visual acuity of 20/25 and avoided vitrectomy with only two weeks of high-dose oral prednisolone1). Multimodal imaging enables non-invasive follow-up and is expected to improve the accuracy of surgical indication decisions.
Zou et al. (2025) performed staged procedures for a most severe case (vitreous hemorrhage + tractional retinal detachment) caused by cocoon setae: vitrectomy + intraocular foreign body removal + endolaser + C3F8 gas tamponade, followed by lens extraction + intraocular lens implantation + YAG laser posterior capsulotomy. Final visual acuity recovered to 20/20, reported as a case of complete recovery from the most severe outcome5).
Tamilarsan et al. (2022) reported four cases of Ophthalmia Nodosa in motorcycle riders, showing that insect collisions during high-speed riding are an occupational risk. The importance of prevention through wearing protective glasses or visors is emphasized 2).
Ashkenazy N, Treister AD, Enghelberg S, et al. Type V ophthalmia nodosa caused by moth setae: multimodal imaging and conservative management with systemic corticosteroids. Am J Ophthalmol Case Rep. 2022;28:101734.
Tamilarsan K, Pugalenthi LS, Sankar DS, et al. Ophthalmia nodosa in motorcyclists: a case series. Indian J Ophthalmol. 2022;70(5):1813-1815.
Levy JA, Feinstein M, Enghelberg S, et al. White-marked tussock caterpillar ophthalmia nodosa requiring operative intervention: a case report. Am J Ophthalmol Case Rep. 2023;30:101850.
Al Somali AI, Al Masmali A, Alkatan HM, et al. Caterpillar hair-induced ophthalmia nodosa in a child: the first case reported in the Middle East. Saudi J Ophthalmol. 2021;35(1):86-89.
Zou Y, Zhang C, Li X, et al. Severe vitreoretinal complications secondary to tussock moth cocoon setae: a case report. BMC Ophthalmol. 2025;25:142.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.