Leukemic retinopathy is a general term for fundus lesions associated with leukemia. It is a malignant tumor caused by clonal proliferation of leukocytes or upstream hematopoietic stem cells, leading to systemic infiltrative lesions. Leukemic retinopathy is the most common ocular complication seen ophthalmologically, occurring in approximately 70% of all leukemia patients. It is observed in both acute and chronic leukemia, but is particularly frequent during relapse of acute leukemia. Intraocular infiltration of leukemic cells can reach over 80% in some cases 4).
Leukemia is clinically classified into non-lymphocytic and lymphocytic types, each further divided into acute and chronic forms. Ocular findings are more common in acute leukemia. It can occur in any type of leukemia, including chronic myeloid leukemia (CML), acute myeloid leukemia (AML), acute lymphoblastic leukemia (ALL), and chronic eosinophilic leukemia (CEL). Fundus findings may appear as the first sign of leukemia and serve as a diagnostic indicator reflecting systemic disease activity 3).
QDoes leukemic retinopathy occur only in advanced stages of leukemia?
A
Not necessarily. Cases have been reported where fundus findings appear at the same time as the onset of leukemia or as the initial sign 3). Unexplained retinal hemorrhage or sudden vision loss may lead to the discovery of a hematologic disorder. Since fundus findings can also indicate relapse, regular ophthalmologic follow-up is important.
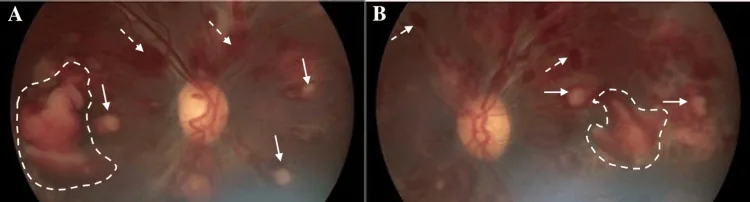
Beketova T, et al. Leukemic Retinopathy: A Diagnostic Clue for Initial Detection and Prognosis of Leukemia. Cureus. 2023. Figure 1. PMCID: PMC10788118. License: CC BY.
A is a color fundus photograph of the right eye at initial visit, B is of the left eye, showing Roth spots, extensive intraretinal hemorrhages, and chronic preretinal hemorrhages. This corresponds to the retinal hemorrhages discussed in the section “2. Main Symptoms and Clinical Findings”.
In extreme leukocytosis with WBC ≥200,000/μL, peripheral retinal ischemia and neovascularization may be observed 1). Cases presenting with a CRVO-like appearance have also been reported 1).
Primary lesions
Definition: Changes due to direct infiltration of the retina and vitreous by leukemic cells.
Main findings: Retinal infiltrates, vitreous cell infiltration, optic nerve infiltration.
Features: Can occur even with relatively mild blood abnormalities.
Secondary lesions
Definition: Changes resulting from blood abnormalities such as anemia, thrombocytopenia, and hyperviscosity.
Main findings: Retinal hemorrhages, Roth spots, venous dilation and tortuosity, cotton-wool spots.
Features: Often correlate with abnormal blood test results.
Ocular complications of leukemia are not limited to the retina. The following findings due to leukemic cell infiltration of the anterior segment may be observed.
Conjunctival hemorrhage, thickening, edema: Caused by leukemic cell infiltration of the eyelids and conjunctiva.
Corkscrew vessels: Characteristic finding where conjunctival vessels near the corneal limbus become tortuous in a corkscrew pattern.
Infiltrative lesions at the corneal limbus: Infiltrates may be observed at the corneal limbus.
Pseudo-hypopyon: When cellular infiltration occurs in the anterior chamber, a pseudo-hypopyon resembling inflammatory hypopyon may develop. Differentiation from iritis and uveitis is necessary.
Posterior synechiae: May occur due to diffuse infiltration of the iris.
Secondary glaucoma: Infiltration of the trabecular meshwork may lead to secondary glaucoma.
Choked disc: Increased intracranial pressure due to cellular infiltration into the cranium leads to papilledema.
Ocular motor disturbances: Paralysis of cranial nerves results in diplopia and impaired eye movements.
Optic nerve infiltration (especially in pediatric acute leukemia): Direct cellular infiltration of the optic nerve causes decreased visual acuity, papilledema, and pupillary abnormalities.
In chronic leukemia, retinal microaneurysms, retinal ischemia, retinal hemorrhages, retinal elevation lesions, retinal neovascularization, and papilledema may also occur.
Subretinal fluid (SRF) and intraretinal fluid (IRF): Detected as exudative changes on OCT2).
Decreased vessel density: OCTA shows reduced density in the superficial and deep capillary plexuses (SCP and DCP) 2)4).
Outer retinal damage (EZ loss): Cases showing loss of the ellipsoid zone have been reported 4).
QWhat visual changes occur in leukemic retinopathy?
A
When hemorrhage or edema involves the macula, central visual acuity decreases rapidly. If peripheral lesions are predominant, subjective symptoms may be minimal. When papilledema is present, the central visual field may become dark (central scotoma). If pseudohypopyon or proptosis occurs, eye pain and photophobia may appear.
Ocular findings can serve as indicators for initiating systemic treatment and prognosis, so the diagnostic role of ophthalmology is important. If recurrence in organ tissues is suspected, bone marrow recurrence is predicted within weeks to months, requiring re-evaluation by hematology.
Complete blood count (CBC): Assesses white blood cell count, anemia, and thrombocytopenia. Evaluates the correlation between fundus findings and blood test values3).
Bone marrow biopsy and flow cytometry: Essential for definitive diagnosis and classification of leukemia1)3).
OCT: Useful for quantifying SRF and IRF, and evaluating outer retinal damage2)4).
Ultra-widefield fluorescein angiography (UWFA): Detects peripheral retinal non-perfusion areas and neovascularization2).
OCTA: Non-invasively evaluates vessel density in superficial and deep capillary plexuses2)4). Also useful for detecting early changes before symptom onset.
MRI: Used to evaluate orbital and optic nerve infiltration.
B-mode ultrasound: Used when fundus observation is difficult due to vitreous hemorrhage, etc. 4).
Ocular findings can be an indicator for initiating systemic treatment and determining prognosis in leukemia. Fundus findings may be the first sign of the disease or suggest relapse in organs and tissues, and can provide clues to predict bone marrow relapse within weeks to months. When an ophthalmologist detects abnormalities, it is important to promptly inform the hematology department and proceed with further evaluation.
Pseudohypopyon: Differentiation from iritis/uveitis is necessary. History and activity of systemic leukemia are key to differentiation.
Roth spots: Also appear in infective endocarditis, anemia, and diabetes, so differentiation of the underlying disease is necessary.
Secondary glaucoma: Differentiation between glaucoma due to trabecular meshwork infiltration and other secondary glaucomas is required.
QIf there is unexplained retinal hemorrhage, what tests should be performed?
A
If bilateral multiple retinal hemorrhages or Roth spots are observed, referral to hematology is necessary. CBC (complete blood count) and peripheral blood smear examination are the first steps 3). If pseudohypopyon is present, anterior segment infiltration due to leukemia should be suspected, and systemic evaluation is needed. Collaboration between ophthalmology and hematology prevents delays in diagnosis.
Treatment is selected according to the type and severity of leukemia and the degree of ocular symptoms. Systemic chemotherapy is the mainstay, and fundus findings often improve in response to systemic treatment. Systemic chemotherapy may not adequately reach the ocular region, and radiation therapy may be combined.
Systemic Chemotherapy
CML: Tyrosine kinase inhibitors (TKIs) are first-line. Dasatinib has been reported to improve retinopathy 2).
AML: Daunorubicin + cytarabine (DA therapy) is standard.
CEL: Imatinib is considered effective 3).
Adjunctive cytoreduction: Rapid reduction of WBC with hydroxyurea is effective1)3).
Leukapheresis
Leukapheresis: Selective removal of white blood cells via extracorporeal circulation.
Recommendation grade: ASFA (American Society for Apheresis) grade 2B1).
Indications: Acute visual impairment due to extreme leukocytosis (WBC >200K).
Effect: Rapid visual recovery can be expected1).
Ophthalmic Treatment
Radiation therapy: For iris infiltration, leukemic retinopathy, and secondary glaucoma, 2.5 Gy × 5 days is reported to induce remission. For optic nerve infiltration causing vision loss, higher doses of 7–20 Gy are used.
Photocoagulation: Performed for significant retinal ischemia.
Vitrectomy (PPV): Performed in stages for non-absorbing massive hemorrhage4).
Perform regular fundus examinations at the time of leukemia diagnosis or when recurrence is suspected.
If leukemic retinopathy is observed, contact the hematology department to coordinate systemic treatment.
If iris or orbital infiltration is suspected, consider local radiation therapy.
If there is vision loss due to optic nerve infiltration, consider high-dose radiation therapy.
Consider photocoagulation for significant retinal ischemia and vitrectomy for non-absorbing vitreous hemorrhage.
When accompanied by GVHD after hematopoietic stem cell transplantation, dry eye management should be performed concurrently.
QWill vision recover with treatment?
A
As leukemia goes into remission with systemic chemotherapy, retinal hemorrhages and edema often improve, and vision recovers in many cases. However, it has been reported that decreased vascular density in the deep capillary plexus (DCP) is difficult to recover even after treatment 2). If outer retinal damage (EZ loss) is extensive, visual prognosis may be poor. Radiation therapy for optic nerve infiltration may be effective for vision loss.
QWhat is leukapheresis (leukocyte removal therapy)?
A
It is a treatment that selectively removes leukocytes by circulating blood outside the body. It is used as a bridge until chemotherapy takes effect for emergency visual impairment due to hyperleukocytosis (WBC >200,000/μL) 1). ASFA recommends it as grade 2B.
Leukemic cells directly infiltrate the retinal vessels, parenchyma, and vitreous, causing local tissue damage. A characteristic feature is that it can occur even when blood abnormalities are relatively mild. Infiltration of leukemic cells around retinal vessels leads to vascular occlusion, resulting in dilation, tortuosity, and ischemia of retinal veins.
Anemia, thrombocytopenia, and hyperviscosity act in combination.
Leukostasis: When WBC exceeds 200,000/μL, leukocytes physically occlude retinal capillaries, leading to retinal ischemia and hemorrhage 2).
Anemia and thrombocytopenia: The combination of reduced oxygen supply and bleeding tendency causes multiple hemorrhages and Roth spots.
The deep capillary plexus (DCP) has lower perfusion pressure than the superficial capillary plexus (SCP) and is more susceptible to leukostasis. After treatment, vascular density in the DCP is difficult to restore 2), which affects long-term visual prognosis. Outer retinal damage (EZ loss) is thought to reflect photoreceptor damage due to chronic ischemia 4).
In recent years, the number of long-term survivors after hematopoietic stem cell transplantation has increased, and management of post-transplant ocular complications has become more important.
Among ocular complications associated with graft-versus-host disease (GVHD), dry eye is the most common. In refractory cases, it can lead to corneal melting and perforation, requiring strict dry eye management.
The following complications are observed:
Dry eye: The most common complication. It involves a combination of decreased tear secretion and increased tear evaporation.
Meibomian gland dysfunction: Inflammation and obstruction of the meibomian glands impair the lipid layer of the tear film.
Spontaneous punctal closure: Fibrosis due to GVHD may affect the puncta.
Conjunctival pseudomembrane formation: Inflammatory reaction of the conjunctival epithelium leads to pseudomembrane formation.
Corneal calcification, thinning, and perforation: In severe GVHD, the corneal stroma is affected.
For GVHD-related dry eye, artificial tears, steroid eye drops, cyclosporine eye drops, and tacrolimus eye drops are used in combination. It is important to concurrently evaluate meibomian gland dysfunction, punctal occlusion, and conjunctival pseudomembrane formation, and in severe cases, not to miss signs of corneal melting or perforation.
Jamshidi et al. (2025) reported that in cases of leukemic retinopathy, OCTA can detect decreased vessel density in the deep capillary plexus before clinically apparent retinopathy appears 4). OCTA has potential as a tool for early detection of asymptomatic retinal lesions in leukemia patients.
Jamshidi et al. (2025) reported a case of severe leukemic retinopathy treated with staged vitrectomy4). The effectiveness of a dexamethasone implant (Ozurdex) for residual cystoid macular edema (CME) after surgery was also demonstrated, leading to visual improvement 4). The combination of ophthalmic intervention and systemic treatment may contribute to improved prognosis.
Leong S, Do T, Shodiya M, Lee J. Acute vision loss due to CML leukemic retinopathy reversed with leukapheresis. Clinical case reports. 2023;11(6):e7441. doi:10.1002/ccr3.7441. PMID:37273676; PMCID:PMC10238709.
Lim J, Kim I, Sagong M. Leukostasis retinopathy as the first sign of CML with severe hyperleukocytosis. Korean J Ophthalmol. 2023;37(3):266-269.
Beketova T, Mordechaev E, Murillo B, Schlesinger MD. Leukemic Retinopathy: A Diagnostic Clue for Initial Detection and Prognosis of Leukemia. Cureus. 2023;15(12):e50587. doi:10.7759/cureus.50587. PMID:38222198; PMCID:PMC10788118.
Jamshidi F, Boyce TM, Christopher Bowen R, Culver Boldt H, Binkley EM. Surgical management of a case of severe leukemic retinopathy. American journal of ophthalmology case reports. 2025;39:102417. doi:10.1016/j.ajoc.2025.102417. PMID:40955320; PMCID:PMC12433482.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.