Crunch syndrome is a condition in which tractional retinal detachment (TRD) newly develops or rapidly progresses in eyes with proliferative retinopathy after intravitreal injection of anti-VEGF (vascular endothelial growth factor) drugs. 1, 2, 3)
The name “crunch” comes from the way the retinal detachment closes toward the macula like a jaw crunching. 3)
The incidence varies from 1.5% to 18.4% depending on the report, with the most common being about 5%. 1) Onset occurs 1 to 6 weeks after anti-VEGF injection, with an average of 13 days (range 3 to 31 days). 1, 2) More than 80% of cases develop within 5 days after the first injection. 1)
Patients with severe proliferative diabetic retinopathy, pre-existing TRD, or extensive fibrosis have a higher incidence. The combination of tractional and rhegmatogenous retinal detachment is usually limited to 0.05-0.5%, but can reach up to 43% when circumferential fibrovascular proliferative membranes are present.
QHow often does crunch syndrome occur?
A
The incidence varies from 1.5% to 18.4% depending on the report, with the most common being about 5%. 1) The risk increases in cases of severe proliferative diabetic retinopathy, pre-existing TRD, or extensive fibrosis. It often develops within 1 to 6 weeks after injection (average 13 days), and more than 80% of cases develop within 5 days after the first injection.
Acute vision loss: Occurs within 1 to 6 weeks after injection. In a case by Li, vision dropped from 20/25 to hand motion in 3 days. 2) In a case by Bromeo, a drop from 20/30-2 to hand motion was recorded. 3)
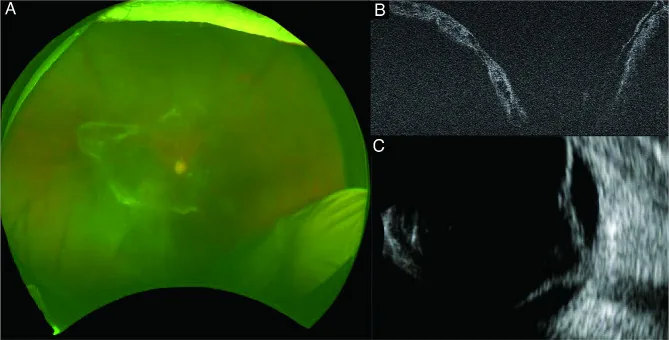
OCT is useful for assessing the extent of TRD, macular involvement, and retinal edema. 1, 3)OCTA is used for quantitative evaluation of neovascularization and ischemic areas. 2) When the fundus is difficult to observe due to vitreous hemorrhage, ultrasound examination is performed to evaluate TRD. 4, 5)
Intravitreal injection of anti-VEGF agents can trigger crunch syndrome. 1, 2, 3) The most common causative agent is bevacizumab, 1, 2) and cases have also been reported with pegaptanib and ranibizumab. 2) The first report of onset due to conbercept was by Li & Zhang (2025). 2) There are currently no reports of an association with aflibercept. 2)
In addition to anti-VEGF agents, panretinal photocoagulation (PRP) alone or in combination with anti-VEGF can also induce crunch. The mechanism is thought to involve collagen contraction due to inflammation and heat, and the combination of anti-VEGF with panretinal photocoagulation/cryocoagulation may synergistically worsen traction. 3)
The following table shows the status of crunch reports by anti-VEGF agent.
QWhen does crunch syndrome occur after anti-VEGF injection?
A
It usually occurs within 1 to 6 weeks after injection, with an average of 13 days (range 3 to 31 days). 1, 2) More than 80% of cases develop within 5 days after the first injection, and the shortest reported onset is 3 days after injection. In patients at high risk, strict follow-up from early after injection is necessary.
Intraocular tamponade: Maintain retinal reattachment with silicone oil or gas 2, 3)
In Li’s case, silicone oil tamponade was performed, 2) and in Bromeo’s case, silicone oil tamponade was removed and cataract surgery was performed simultaneously at 6 months. 3)
Emergency Surgery (Standard Treatment)
Vitrectomy + Membranectomy: Release traction by careful dissection of the fibrovascular membrane
There is evidence that preoperative anti-VEGF administration contributes to shorter surgical time, fewer retinal breaks, and reduced intraoperative bleeding.4, 5) A Cochrane systematic review showed that preoperative or intraoperative bevacizumab reduces postoperative vitreous hemorrhage.4, 5)
In cases with extremely high surgical risk due to heart disease, anti-VEGF monotherapy is exceptionally selected. In the Yuan case, a patient inoperable due to heart disease received regular bevacizumab injections every 8–12 weeks for over 1.5 years, achieving stable TRD and maintained foveal attachment.1)
QIf crunch syndrome develops, can vision recovery be expected?
A
Early detection and early surgical intervention are important, but visual prognosis is not always favorable. In Li’s case, visual acuity after vitrectomy remained at counting fingers, 2) and in Bromeo’s case, it was reported as 20/400 after 6 months. 3) Even in inoperable cases, there are reports of TRD stabilization and foveal attachment maintenance with anti-VEGF monotherapy, 1) but early intervention is key to improving prognosis.
In proliferative diabetic retinopathy, upregulation of VEGF leads to angiogenesis and vascular proliferation into the posterior vitreous cortex. Subsequently, fibrous tissue forms and contracts, progressing to TRD. 1)Proliferative diabetic retinopathy transitions over time from a predominantly angiogenic phase to a predominantly fibrotic phase, and anti-VEGF administration may accelerate this progression. 2)
Mechanism of Crunch Induction by Anti-VEGF Administration
Li & Zhang (2025) proposed that the mechanism of crunch induction after anti-VEGF administration involves rapid regression of new vessels causing abrupt changes in traction, as well as fibrosis promotion and retinal stiffening due to the interplay of decreased VEGF and increased TGF-β (transforming growth factor-β). Potent VEGF inhibitors may induce a more pronounced fibrotic response. 2)
Bromeo et al. (2021) reported in vitro experiments that bevacizumab upregulates TGF-β2, CTGF (connective tissue growth factor), and CNTF (ciliary neurotrophic factor) in RPE cells and glial cells, accelerating fibrosis. 3)
Pre-existing vitreoretinal adhesion patterns and biomechanical stress from long-standing fibrovascular proliferation are thought to contribute to acute decompensation after anti-VEGF administration. 2)
Mechanism of Action of Panretinal Photocoagulation
Panretinal photocoagulation destroys peripheral RPE cells and photoreceptors, reducing oxygen consumption in the outer layers. This increases oxygen diffusion to the inner layers, decreasing VEGF production stimuli and further suppressing angiogenesis. 6) On the other hand, inflammation and heat from panretinal photocoagulation may induce collagen contraction and worsen traction. 3)
In proliferative diabetic retinopathy, fragile new vessels cause leakage of fluid and protein, leading to macular edema and hemorrhage. When abnormal vessels fibrose and pull on the retina, TRD occurs. 6)
In some cases, after anti-VEGF injection, new vessels regress, vitreoretinal traction is released, and TRD improves. This phenomenon is known as “favorable crunch.”
Lee et al. reported that TRD flattened or resolved in 3 of 4 eyes. 1)
QWhat is "favorable crunch"?
A
It refers to the phenomenon where neovascularization regresses after anti-VEGF injection, releasing vitreoretinal traction and improving TRD. This follows the opposite outcome of the usual crunch (traction worsening type). In the report by Lee et al., TRD was flattened or resolved in 3 out of 4 eyes, 1) indicating that not all cases worsen due to crunch.
DRCR.net Protocol S compared ranibizumab and panretinal photocoagulation and found no statistically significant difference in the incidence of TRD in proliferative diabetic retinopathy. However, when patients with proliferative diabetic retinopathy dropped out of follow-up during anti-VEGF injections, visual and anatomical outcomes were worse compared to those who received panretinal photocoagulation. 4, 5)
This result suggests that anti-VEGF monotherapy may be considered only for patients who can reliably continue follow-up. 4, 5)
The first report of crunch syndrome due to conbercept was published in 2025. 2) Whether potent VEGF inhibitors such as aflibercept and conbercept induce more pronounced fibrotic reactions remains a topic for future research. 2)
Changes in cytokine profiles, including TGF-β, have been suggested to be involved in the development of crunch syndrome, 2) and elucidation of the molecular mechanisms is expected to lead to future treatment strategies.
Regarding the risk of systemic arterial thromboembolic events associated with intravitreal injection of anti-VEGF drugs, no definitive conclusions have been reached in current clinical trials. 7)
Yuan M, Hoyek S, Kim LA, Chaaya C, Patel N. Antivascular Endothelial Growth Factor Injections for the Chronic Treatment of Macula-off, Fovea-on Diabetic Tractional Retinal Detachment With Vitreous Hemorrhage. Journal of vitreoretinal diseases. 2025;9(2):236-240. doi:10.1177/24741264241297684. PMID:39544710; PMCID:PMC11558646.
Li Z, Zhang Y. Anti-Vascular Endothelial Growth Factor Crunch Syndrome in Proliferative Diabetic Retinopathy. JCEM case reports. 2025;3(6):luaf083. doi:10.1210/jcemcr/luaf083. PMID:40255438; PMCID:PMC12006834.
Bromeo AJ, Veloso A, Lerit SJ, Gomez MC. Tractional retinal detachment (‘crunch’ phenomenon) from intravitreal anti-vascular endothelial growth factor injection in central retinal vein occlusion. BMJ case reports. 2021;14(4). doi:10.1136/bcr-2020-240506. PMID:33910794; PMCID:PMC8094377.
Lim JI, Kim SJ, Bailey ST, et al. Diabetic Retinopathy Preferred Practice Pattern. Ophthalmology. 2025 Apr;132(4):P75-P162. doi:10.1016/j.ophtha.2024.12.020. PMID:39918521.
Lim JI, Kim SJ, Bailey ST, et al. Diabetic Retinopathy Preferred Practice Pattern. Ophthalmology. 2025 Apr;132(4):P75-P162. doi:10.1016/j.ophtha.2024.12.020. PMID:39918521.
O’Leary F, Campbell M. The blood-retina barrier in health and disease. The FEBS journal. 2023;290(4):878-891. doi:10.1111/febs.16330. PMID:34923749.
Kovach JL, Bailey ST, Kim SJ, Lim JI, Vemulakonda GA, Ying GS, et al. Retinal Vein Occlusions Preferred Practice Pattern®. Ophthalmology. 2025;132(4):P303-P343. doi:10.1016/j.ophtha.2024.12.025. PMID:39918523.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.