Choroidal neovascularization (CNV) is a disease in which new blood vessels originating from the choroid preferentially occur in the macula. The new vessels proliferate beneath the retinal pigment epithelium (RPE) (type 1/classic) or above the RPE (type 2/occult). In cases of choroiditis or idiopathic CNV, inflammation plays a major role, and CNV is considered a reactive change or wound healing process in response to damage to the RPE-Bruch’s membrane-choriocapillaris complex.
Inflammatory choroidal neovascularization (I-CNV) is a severe complication of posterior uveitis caused by chorioretinal inflammation. It can occur in both infectious and non-infectious uveitis1). I-CNV is considered the third most common cause of CNV after AMD and pathologic myopia1).
In patients with posterior uveitis, CNV occurs in 2.7%, and in patients with panuveitis, 0.8%, which is more frequent than in anterior or intermediate uveitis (0.1%)1). In idiopathic uveitis, CNV occurs as a complication in 13–20% of cases3). Most I-CNV presents as type 2 (classic) CNV, forming beneath the RPE (type 1) or above the RPE (type 2) after breaking through Bruch’s membrane1).
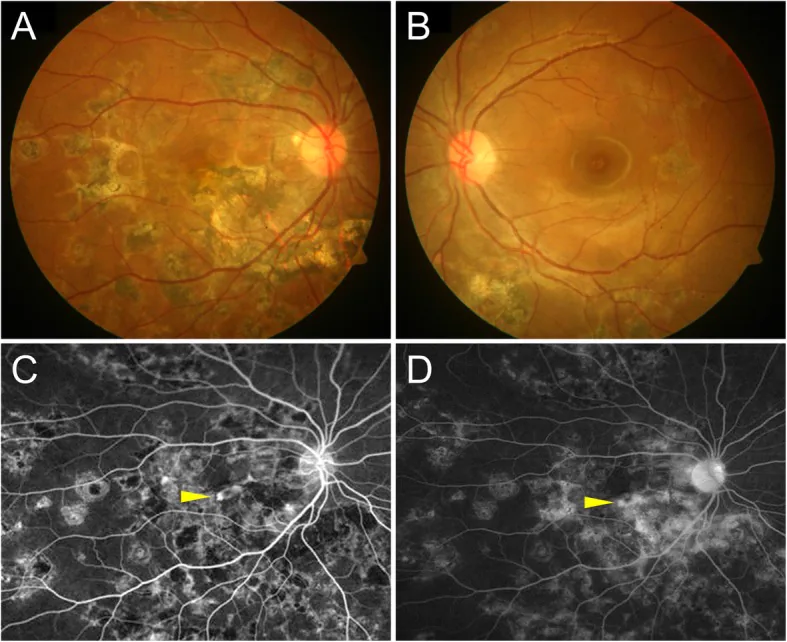
Agarwal A, et al. An update on inflammatory choroidal neovascularization: epidemiology, multimodal imaging, and management. J Ophthalmic Inflamm Infect. 2018. Figure 1. PMCID: PMC6135736. License: CC BY.
The upper fundus photographs show multiple chorioretinal scars in both eyes. In the lower fluorescein angiography images, small lesions in the macula exhibit early hyperfluorescence that intensifies in the late phase, supporting the presence of inflammatory choroidal neovascularization.
Active lesions located outside the fovea may be asymptomatic and can be missed due to inflammatory lesions, scars, pigmentation, or accumulation of intraretinal or subretinal fluid1).
Fundus examination reveals yellowish-white subretinal lesions around the macula.
Sub-RPECNV (Classic type): Depicted as an orange-red elevated lesion
Subretinal pigment epithelium CNV (Occult type): Seen as a gray-white plaque, often with marginal subretinal hemorrhage and retinal detachment
Macular distribution of I-CNV: Subfoveal 60%, juxtafoveal 35%, peripapillary 5%
Fibrovascular scar (remnant of past CNV activity) may persist
After CNV involutes, atrophic lesions of the retinal pigment epithelium-choriocapillaris complex may form. In sub-RPECNV, fibrous tissue forms under the retina, which may lead to permanent vision loss, central scotoma, and metamorphopsia.
Inflammatory damage: Inflammation damages the RPE-Bruch’s membrane complex → disruption of the outer blood-retinal barrier → neovascular proliferation from the choroid
Ischemia/hypoxia: Inflammation-induced perfusion impairment → hypoxia gradient in the retina and choroid → promotion of CNV formation
Activated inflammatory cells secrete cytotoxic enzymes that degrade Bruch’s membrane. Released pro-angiogenic cytokines (IL-6, IL-8, TNF-α) promote VEGF expression and CNV growth 2). In uveitis, cytokines such as TNF-α, IL-6, and IL-1 damage RPE, further amplifying VEGF expression and promoting I-CNV formation 3).
According to the Uveitis Clinical Practice Guidelines (2019), caution is needed for CNV complications in posterior uveitis such as PIC, multifocal choroiditis, sarcoidosis, Harada disease, and serpiginous choroiditis, and a combination of inflammation control and anti-VEGF therapy is recommended 3).
Risk factors5):
Risk factor
Details
Presence of subretinal neovascularization
Risk of I-CNV development increases by 3 times or more
Active inflammation
Significantly higher CNV risk compared to inactive phase
Diagnosis of I-CNV is challenging, and multimodal imaging is recommended1).
Fluorescein angiography (FA): Most I-CNVs appear as classic (type 2) CNV. CNV lesions show early isofluorescence to hyperfluorescence with late leakage. However, active inflammatory lesions also show similar FA findings, so FA alone has limitations in diagnosis 1). Characteristic features include well-defined hyperfluorescence in the early phase (classic type) or diffuse pigment leakage in the late phase (occult type).
Indocyanine green angiography (ICGA): Allows more detailed evaluation of choroidal vascular structures than FA. I-CNV shows early hyperfluorescence, enabling differentiation from active inflammatory foci (early hypofluorescence) 1). ICGA is essential for differentiating sub-RPECNV, and in multifocal choroiditis, it is useful for assessing non-perfusion areas of the choriocapillaris and evaluating CNV risk 1).
“Pitchfork sign”: A hyperreflective lesion extending finger-like from I-CNV to the outer retinal layers. This is an OCT finding characteristic of I-CNV reported in multifocal choroiditis/PIC, intraocular tuberculosis, and acute syphilitic posterior polymorphous choroiditis 1)
“Sponge sign”: Increased choroidal thickness beneath I-CNV (decreases after treatment). An auxiliary finding to differentiate inflammatory from myopic CNV1)
Central retinal thickness is useful as an objective indicator of I-CNV activity 1)
OCT angiography (OCTA): Non-invasively visualizes the vascular structure of CNV. It has higher accuracy than FA alone in differentiating CNV from inflammatory lesions and is particularly useful for identifying type 1 neovascular networks8).
Fundus autofluorescence (FAF): Active I-CNV shows normal fluorescence or hyperautofluorescence. Hypoautofluorescent areas correlate with photoreceptor and RPE loss and are useful for detecting peripheral I-CNV1).
QCan I-CNV be diagnosed with OCT alone?
A
OCT is very useful for evaluating I-CNV, but definitive diagnosis alone is often difficult. OCT findings characteristic of I-CNV, such as the “pitchfork sign,” have ancillary value, but multimodal imaging combining FA, ICGA, OCTA, and FAF is essential for accurate diagnosis and differentiation from inflammatory lesions1).
First, rule out infectious diseases (e.g., toxoplasmosis, tuberculosis, Bartonella henselae) and provide appropriate anti-infective therapy. For underlying uveitis after exclusion:
Regardless of the underlying disease, intravitreal injection of VEGF inhibitors is performed for foveal CNV. Since VEGF is closely involved in the development and growth of CNV, drugs that inhibit it are useful for inducing CNV regression and preventing hemorrhage and exudation.
Not covered by insurance (covered for AMD and myopic maculopathy)
Ranibizumab (Lucentis)
Anti-VEGF-A monoclonal antibody fragment
Not covered by insurance (covered for AMD and myopic maculopathy)
Bevacizumab (Avastin)
Anti-VEGF-A full-length monoclonal antibody
Not covered by insurance (off-label), used for inflammatory CNV
Aflibercept and ranibizumab are covered by insurance only for age-related macular degeneration and myopic maculopathy. For inflammatory CNV, bevacizumab (1.25 mg/0.05 mL intravitreal injection) is used off-label 3).
Combination of anti-inflammatory therapy and anti-VEGF drugs results in improvement in 80% of patients and stabilization in 15% 4). Anti-VEGF monotherapy in PIC patients has a reported recurrence rate of 50%, indicating the need for systemic treatment of underlying uveitis7).
Comparison between an induction phase (monthly injections for 3 months) and pro re nata (PRN) dosing shows that an induction phase does not lead to superior outcomes 1). Randomized controlled trials have confirmed that anti-VEGF drugs (ranibizumab 0.5 mg intravitreal injection) are effective in improving visual acuity and regressing neovascularization in I-CNV 6).
QWhich anti-VEGF drugs are available for inflammatory CNV in Japan?
A
Aflibercept (Eylea) and ranibizumab (Lucentis) are only covered by insurance for age-related macular degeneration and myopic maculopathy. For inflammatory CNV, bevacizumab (Avastin, off-label) may be used at some ophthalmology facilities. Treatment choice should be decided after thorough consultation with the attending physician.
For extrafoveal CNV, photocoagulation with a thermal laser is performed. Photocoagulation directly occludes the CNV, but the irradiated area results in permanent retinal damage, so the distance from the fovea must be carefully evaluated to determine the indication.
The pathophysiology of I-CNV is similar to that of CNV in AMD and pathologic myopia, but is characterized by the addition of inflammatory factors 1).
Chronic inflammation, oxidative stress, and ischemia are involved, and CNV occurs as a reactive change or wound healing process in response to damage to the RPE-Bruch membrane-choriocapillaris complex.
Molecular mechanisms:
Increased VEGF expression promotes neovascular proliferation (common to AMD and myopic CNV)
The extravascular component of CNV contains fibroblasts and leukocytes expressing CXCR4
RPE cells produce TNF-α, IL-1, IL-2, IL-6, and IL-10, functioning as inflammatory components 1)
Imbalance with anti-angiogenic factors (angiostatin, endostatin, PEDF) triggers the process 1)
In uveitis, cytokines such as TNF-α, IL-6, and IL-1 are secreted by inflammatory cells, damaging the RPE and further amplifying VEGF expression 3). The interaction between these cytokines and VEGF promotes I-CNV formation.
Differences between I-CNV and AMD-related CNV:
Immunohistochemical studies have reported that the CXCR4 staining pattern of the vascular mesh in I-CNV differs from that in AMD-related CNV, suggesting that capillaries may play different roles in membrane formation 9).
Some “idiopathic” CNV may appear as a preceding symptom of posterior uveitis1). New blood vessels often grow from the edge of the inflammatory lesion (the edge of post-inflammatory atrophic chorioretinal scar).
OCTA plays an important role in the diagnosis and follow-up of I-CNV. Evidence of the superiority of OCTA over FA/ICGA alone is accumulating, and it has been shown to be essential for identifying type 1 neovascular networks even when FA/ICGA results are inconclusive8). OCTA is also useful as a monitoring indicator for active CNV, allowing quantitative assessment of neovascular regression after treatment8).
Clinical significance of the “sponge sign”:
Increased choroidal thickness under I-CNV on OCT (the “sponge sign,” which decreases after treatment) is attracting attention as a new auxiliary indicator for monitoring I-CNV activity. It may also be applicable for differentiating inflammatory CNV from myopic CNV1).
Long-term outcomes of anti-VEGF therapy:
Medium- to long-term data have accumulated showing an improvement of approximately 0.3 logMAR units in visual acuity after anti-VEGF therapy (1–5 injections) for posterior uveitis of various causes4). A recurrence rate of 50% has been reported with anti-VEGF monotherapy in PIC patients, and management of the underlying disease determines long-term prognosis7).
Treat and Extend (T&E) regimen:
The T&E regimen (gradually extending treatment intervals), established for AMD and myopic CNV, is being investigated for application to I-CNV. It may reduce treatment burden while maintaining vision, but evidence specific to inflammatory CNV is awaited.
Faricimab (anti-VEGF-A/Ang-2 dual inhibitor):
Faricimab, which simultaneously inhibits VEGF-A and angiopoietin-2 (Ang-2), is approved for AMD and diabetic macular edema, and its application to inflammatory CNV is under research. Since Ang-2 is involved in both angiogenesis and inflammation, a specific effect on I-CNV is expected.
Standardization of multimodal approach:
A multimodal approach including FAF, OCTA, and near-infrared autofluorescence imaging is promising for diagnosing I-CNV, and FAF is particularly useful for detecting and monitoring peripheral I-CNV 1).
QWhat is the visual prognosis for I-CNV?
A
Control of underlying uveitis and early treatment with anti-VEGF agents can help maintain or improve visual acuity. However, a 50% recurrence rate with anti-VEGF monotherapy has been reported in PIC, and management of the underlying disease determines long-term prognosis 7). Regular OCT and OCTA monitoring is useful for early detection of recurrence.
Karska-Basta I, Pociej-Marciak W, Żuber-Łaskawiec K, Markiewicz A, Chrząszcz M, Romanowska-Dixon B, Kubicka-Trząska A.. Diagnostic Challenges in Inflammatory Choroidal Neovascularization. Medicina (Kaunas). 2024;60(3):465. doi:10.3390/medicina60030465. PMID:38541191; PMCID:PMC10972505.
Cheung CMG, Arnold JJ, Holz FG, Park KH, Lai TYY, Larsen M, Mitchell P, Ohno-Matsui K, Chen SJ, Wolf S, Wong TY. Myopic Choroidal Neovascularization: Review, Guidance, and Consensus Statement on Management. Ophthalmology. 2017;124(11):1690-1711. doi:10.1016/j.ophtha.2017.04.028. PMID:28655539.
D’Souza Y, Balasubramaniam S, Nair U. Anti-VEGF treatment for inflammatory choroidal neovascularization: a comprehensive review. Surv Ophthalmol. 2023;68(3):435-461.
Baxter SL, Pistilli M, Pujari SS, Liesegang TL, Suhler EB, Thorne JE, Foster CS, Jabs DA, Levy-Clarke GA, Nussenblatt RB, Rosenbaum JT, Kempen JH.. Risk of choroidal neovascularization among the uveitides. Am J Ophthalmol. 2013;156(3):468-477.e2. doi:10.1016/j.ajo.2013.04.040. PMID:23795984; PMCID:PMC3748230.
Rouvas A, Petrou P, Douvali M, Ntouraki A, Vergados I, Georgalas I, Markomichelakis N.. Intravitreal ranibizumab for the treatment of inflammatory choroidal neovascularization. Retina. 2011;31(5):871-879. doi:10.1097/iae.0b013e3182003ca8. PMID:21358461.