Optical coherence tomography angiography (OCTA) is a non-invasive imaging technique that visualizes blood vessels by applying the principle of optical coherence tomography (OCT). OCT was invented in the 1990s and generates high-resolution cross-sectional images based on low-coherence interferometry. It has become one of the most important diagnostic imaging methods in ophthalmology.
Conventional OCT has low contrast between capillaries and retinal tissue, limiting its ability to monitor vascular changes. Fluorescein angiography (FA) and indocyanine green angiography (ICGA) require intravenous administration of contrast agents, which carries a risk of anaphylactic shock. Additionally, they only provide two-dimensional images without depth information of lesions.
OCTA overcomes these limitations by three-dimensionally visualizing blood vessels at different depths without the use of contrast agents. It is useful for diseases causing retinal circulation abnormalities (e.g., diabetic retinopathy, retinal vein occlusion), optic nerve circulation abnormalities (e.g., glaucoma, ischemic optic neuropathy), and conditions involving choroidal neovascularization.
In neuro-ophthalmology, evaluation of the radial peripapillary capillaries (RPC) around the optic disc is particularly important. A decrease in vessel density is observed in areas corresponding to retinal nerve fiber layer defects (NFLD) seen on fundus examination.
QWhat is the biggest difference between OCTA and conventional fluorescein angiography (FA/ICGA)?
A
OCTA does not require contrast agents, is non-invasive, and allows three-dimensional, layer-specific evaluation of the vascular network. FA/ICGA can detect fluorescein leakage and filling defects, but carries a risk of anaphylaxis due to contrast administration, and the images obtained are only two-dimensional. The two are complementary; OCTA cannot evaluate fluorescein leakage.
2. OCTA Findings and Clinical Applications in Neuro-Ophthalmology
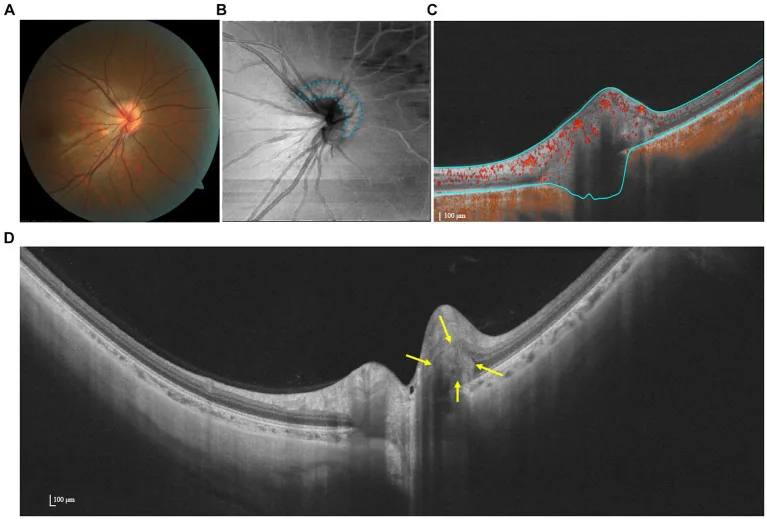
Ruihan Hu, Qiuyan Wu, Zuohuizi Yi et al. Multimodal imaging of optic nerve head abnormalities in high myopia. Frontiers in Neurology. 2024 Apr 23; 15:1366593. Figure 3. PMCID: PMC11075756. License: CC BY.
En face OCTA and SS-OCT images showing PHOMS. The OCT-Angiography image shows…
In neuro-ophthalmic diseases, the main vascular changes observed on OCTA are as follows.
Decreased vessel density (capillary dropout): Seen in optic atrophy, glaucoma, and after optic neuritis. It is distributed in areas corresponding to the NFLD.
Vessel dilation and tortuosity: Observed in the acute phase of papilledema and in some cases of optic neuritis.
Flow void (signal loss): Areas of absent blood flow detected at the level of the choriocapillaris (CC). Useful for evaluating choroidal lesions in systemic inflammatory diseases such as Vogt-Koyanagi-Harada disease and granulomatosis with polyangiitis.
Tangled ball of vessels: A characteristic pattern formed by dilated and tortuous capillaries on the surface of the optic disc in papilledema.
Multiple sclerosis (MS): RNFL thinning is observed regardless of the presence of optic neuritis. The ONH blood flow index (ONH-FI) is significantly reduced in eyes with a history of optic neuritis. Combined use with structural OCT parameters improves detection accuracy.
Optic disc edema (papillitis): Inflammatory disc edema does not show vascular dropout. The radial distribution of peripapillary capillaries is preserved.
Ischemic Optic Neuropathy
Non-arteritic anterior ischemic optic neuropathy (non-arteritic): Peripapillary capillary blood flow impairment is observed in both acute and chronic phases. The temporal sector has the highest blood flow density and is most affected in non-arteritic anterior ischemic optic neuropathy eyes. In the chronic phase, ONH and peripapillary vessel density are directly associated with RNFL damage and visual field defects.
AAION (arteritic): Features include dilation of superficial peripapillary capillaries and focal non-perfusion of superficial and deep retinal capillaries.
Hereditary and Degenerative Diseases
LHON (Leber Hereditary Optic Neuropathy): Capillary dilation is observed during the pseudoedematous phase. A pattern of choriocapillaris loss by disease stage has been described: in the early subacute phase, it decreases from the temporal side, and in the chronic phase, it decreases in all sectors.
Optic Atrophy: Decreased peripapillary microvasculature. Blood flow decreases via autoregulatory mechanisms due to reduced metabolic activity.
Glaucoma
POAG (Primary Open-Angle Glaucoma): Decreased vessel density and blood flow index in the intraoptic, macular, and peripapillary regions.
NTG (Normal-Tension Glaucoma): Decreased peripapillary capillary density is observed similarly to primary open-angle glaucoma but is milder. In suspected glaucoma cases, a decrease in blood flow index may be detectable even before visual acuity loss.
Differentiation between Papilledema and Pseudopapilledema
OCTA is useful for differentiating between papilledema and pseudopapilledema.
Papilledema: Capillaries on the optic disc surface are dilated and tortuous, forming a “tangled ball of vessels.” The peripapillary capillary vessel density is maintained at the same level as the control eye. No vascular dropout is observed.
Pseudopapilledema: Peripapillary capillary vessel density is reduced.
QWhy can OCTA differentiate between papilledema and pseudopapilledema?
A
In papilledema, the edema obscures the underlying capillaries, but capillaries can be visualized on the edema, and the peripapillary vessel density is maintained at the same level as the control eye. In contrast, pseudopapilledema (e.g., optic disc drusen) shows reduced vessel density, and this difference serves as the basis for differentiation.
In optic neuritis or AION with optic disc swelling, detection of acute axonal damage is difficult due to increased cpRNFL thickness from impaired axonal transport. Macular inner retinal layer analysis, such as the ganglion cell complex (GCC), can detect thinning earlier than cpRNFL analysis.
In optic nerve diseases causing central scotoma or cecocentral scotoma, a thinning pattern reflecting damage to the papillomacular bundle (PMB) is observed. OCTA shows decreased RPC density corresponding to the PMB thinning area.
3. Principles, technical features, and limitations of OCTA
OCTA repeatedly images the same location on the fundus and detects only moving parts (red blood cells) as random signal changes. It utilizes the fact that flowing red blood cells produce greater signal variation between scans than stationary tissue.
There are mainly two types of detection methods.
Amplitude decorrelation method: Detects the amplitude difference between two B-scans.
Phase variance method: Detects phase changes of light waves.
A representative algorithm is SSADA (Split-Spectrum Amplitude Decorrelation Angiography). It splits the OCT spectrum into narrower bands and averages the intensity decorrelation of each band, significantly improving the signal-to-noise ratio (SNR).
OCTA automatically generates en face images of four layers.
Layer
Name
Main evaluation target
Superficial
Superficial capillary plexus (SCP)
Retinal nerve fiber layer to ganglion cell layer
Deep layer
Deep retinal capillary plexus (DCP)
Around inner nuclear layer
Outer retina
Outer retinal layers
Normally avascular
Deep
Choriocapillaris (CC)
10–30 μm outside Bruch’s membrane
Segmentation settings vary by device. The RPC and SCP are often combined and displayed as SCP. Some opinions suggest that SS-OCT is superior to SD-OCT for visualizing the choriocapillaris.
No contrast agent required: No risk of anaphylaxis, and can be performed repeatedly.
Short acquisition time: Less burden on the patient.
Three-dimensional evaluation: Enables layer-specific and stereoscopic observation of vascular networks.
Quantitative analysis: Can output quantitative parameters such as vessel density and blood flow index.
On the other hand, attention must be paid to the following limitations and artifacts.
Image quality degradation: In eyes with cataract or vitreous opacity, capillary networks are difficult to visualize. Be careful not to mistake them for non-perfusion areas.
Eye and face motion artifacts: White lines or distortion caused by movement during imaging.
Non-detection of fluorescein leakage: Cannot detect fluorescein leakage, so it cannot fully replace angiography.
Limited scan area: Selectable from 3mm×3mm to 12mm×12mm, but scan area and image quality are inversely proportional.
QWhat artifacts should be noted in OCTA examination?
A
The main artifacts include: decreased signal intensity due to cataract or vitreous opacity (caution: may be confused with non-perfusion areas), white lines or distortion caused by eye or head movement, and projection of superficial signals onto deeper layers (projection artifact). It is important to confirm correspondence with B-scan images during interpretation.
The procedure and key points for OCTA evaluation are described below.
Setting the scan area: Adjust according to the evaluation purpose. For detailed assessment of capillary level, a narrow field of view such as 3×3 mm is desirable. For wide-angle evaluation, select 12×12 mm.
Confirmation of automatic segmentation: En face images of four layers (SCP, DCP, outer retina, CC) are automatically generated, but settings vary by device, so always check correspondence with B-scans.
Evaluation of quantitative parameters: Measure peripapillary vessel density, RPC density, ONH blood flow index (ONH-FI), etc.
The following are representative evaluation indices when using OCTA in neuro-ophthalmology.
Peripapillary vessel density: Correlations with severity and visual field defects in non-arteritic anterior ischemic optic neuropathy and glaucoma have been reported.
RPC density (radial peripapillary capillary density): Can be evaluated sector by sector, confirming correspondence with lesion sites1).
ONH blood flow index (ONH-FI): An index quantifying overall ONH blood flow. Decreases have been reported in MS and glaucoma.
Flow voids in the choriocapillaris plate: Quantifies non-perfused areas of the CC, used to evaluate choroidal lesions in uveitis and systemic vasculitis2).
OCTA plays a complementary role with laser speckle flowgraphy (LSFG). While OCTA evaluates vascular structure (density and morphology), LSFG quantifies blood flow velocity. Combining both enables a more comprehensive circulatory assessment4).
6. Detailed Principles of OCTA and Optic Nerve Vascular Supply
Repeated scans of the same area separate moving components (red blood cells) from static components (tissue). The SSADA algorithm reduces background noise caused by subtle eye movements using an averaging method (volume averaging).
Imaging of the choriocapillaris (CC) is performed at a depth of 10–30 μm outside Bruch’s membrane. The appearance of en face images is granular rather than mesh-like. This is attributed to limitations in lateral resolution, background noise, and vascular discontinuity.
The optic nerve head (ONH) receives blood supply from the short posterior ciliary arteries (SPC arteries), which are terminal branches of the ophthalmic artery. The SPC arteries branch off from the ophthalmic artery and divide into 10–20 branches.
The vascular supply of each region is as follows.
Prelaminar region: Supplied by a mixture of SPC arteries and capillaries from the retinal circulation.
Lamina cribrosa: Supplied by the SPC arteries (directly or via the Zinn-Haller arterial circle).
ONH blood flow depends on ocular perfusion pressure (OPP = mean arterial pressure − intraocular pressure). Regulation involves endothelin-1 and nitric oxide from the vascular endothelium, and animal studies indicate that autoregulation is effective when OPP ≥ 30 mmHg.
In optic atrophy, as the number of peripapillary nerve fibers decreases, metabolic activity declines, leading to reduced blood flow via autoregulation. This is observed as a decrease in vascular density.
7. Latest Research and Future Perspectives (Research-stage Reports)
Yoshimura et al. (2024) reported a case of congenital nasal optic nerve hypoplasia (NOH) in a 20-year-old woman 1). Quantitative evaluation of RPC density using OCTA (Nidek RS-3000 Advance 2, 4.5mm×4.5mm) showed a marked decrease in RPC density on the nasal side of the affected eye to 19% (superior 51%, temporal 58%, inferior 38%). This corresponded to areas of cpRNFL thinning and wedge-shaped visual field defects on Humphrey perimetry, demonstrating the utility of OCTA in elucidating the clinical features and pathophysiology of NOH.
Erba et al. (2021) reported a case of acute VKH in a 24-year-old man 2). OCTA (Topcon DRI OCT Triton Plus) detected flow void spots in the choriocapillaris, which correlated with hypofluorescent areas on ICGA. After treatment with prednisolone 60 mg/day tapered plus cyclosporine A 100 mg twice daily, best-corrected visual acuity recovered to 20/20 in both eyes, and choroidal thickness decreased from RE 712 μm and LE 750 μm at initial visit to RE 538 μm and LE 548 μm at 3 months. Flow voids also markedly decreased after treatment, indicating the usefulness of OCTA for monitoring disease activity.
Mehta et al. (2022) reported a case of granulomatosis with polyangiitis in a 61-year-old man 3). The right eye showed superficial capillary dropout and the left eye showed AION, with OCTA noninvasively detecting capillary dropout in the superficial capillary plexus and flow voids in the choriocapillaris. After immunosuppressive therapy with methylprednisolone 500 mg for 3 days plus a single dose of cyclophosphamide 500 mg, OCTA findings markedly improved at 1 month. OCTA was shown to detect clinically invisible choroidal lesions.
Tsai et al. (2023) evaluated circulation in a 50-year-old woman with optic disc melanocytoma using OCTA and LSFG 4). OCTA detected deep retinal vascular networks within the tumor, and the LSFG MBR (mean vessel density ratio) of the optic disc and macula in the affected eye was lower than in the healthy eye (disc MBR: affected eye 23.0±0.8 vs. healthy eye 26.5±1.9). FA could only assess via dye blockage, but OCTA overcame this limitation. Combined use with LSFG enabled more comprehensive circulation assessment.
In MOG-ON, decreased peripapillary and parafoveal vessel density has been confirmed compared to healthy controls. Vessel density reduction correlated with number of ON episodes, pRNFL thickness, and visual acuity, suggesting that retinal vessel loss may be due to decreased metabolic demand associated with retinal degeneration.
OCTA, being non-invasive and repeatable, is expected to have clinical applications in the following areas.
Early detection of glaucoma: It may detect blood flow changes even before visual acuity decline.
Monitoring progression of optic nerve diseases: Quantitative tracking of changes in vascular density over time.
Assessment of treatment efficacy: Can be used for objective evaluation of treatment response, such as improvement in flow voids after immunosuppressive therapy.
Neurodegenerative diseases (e.g., Alzheimer’s disease): Research is underway on its application to evaluate retinal neural structure and microvasculature.
QFor which diseases is OCTA expected to have clinical applications in the future?
A
Promising areas include early detection of glaucoma (detecting blood flow changes before vision loss), monitoring progression of optic nerve diseases (quantitative assessment of vascular density over time), and noninvasive evaluation of retinal and choroidal lesions in systemic vasculitis. Application to evaluating the efficacy of immunosuppressive therapy using changes in flow voids after treatment as an indicator is also advancing.
Yoshimura M, Hashimoto Y, Hatanaka A, Yoshitomi T. Findings of optical coherence tomography angiography of nasal optic disc hypoplasia. American journal of ophthalmology case reports. 2024;36:102198. doi:10.1016/j.ajoc.2024.102198. PMID:39507852; PMCID:PMC11539110.
Erba S, Govetto A, Scialdone A, Casalino G.. Role of optical coherence tomography angiography in Vogt-Koyanagi-Harada disease. GMS Ophthalmol Cases. 2021;11:Doc06. doi:10.3205/oc000179. PMID:33796433; PMCID:PMC7982992.
Tsai TY, Tsai YJ, Chu YC, Hwang YS, Liao YL. Ocular circulation change in optic disc melanocytoma — a case report and a review of the literature. BMC Ophthalmol. 2023;23:33. doi:10.1186/s12886-023-02785-9.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.