OCT is a non-invasive imaging technique that uses optical interference to provide high-resolution cross-sectional images of the retina and optic nerve1). Originally used for managing retinal diseases and glaucoma, its application to neuro-ophthalmic disorders is rapidly expanding 1).
It is particularly useful for evaluating optic neuropathies and retrochiasmal visual pathway disorders. It can objectively quantify edema and atrophy of the RNFL and GCIPL, and may detect changes before the onset of obvious clinical signs or visual dysfunction 1).
In Japan, the first OCT device was installed at Gunma University in 1997, and insurance coverage began in 2008. It is now an important part of neuro-ophthalmic evaluation, and its use is expected to increase further 1).
In evaluating visual pathway disorders, cpRNFL thickness and macular inner retinal layer thickness are key assessment parameters.
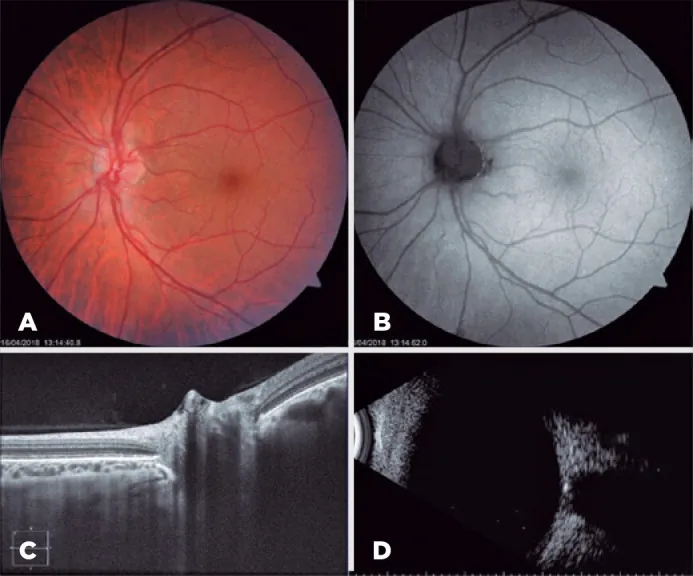
Iridochorioretinal coloboma associated with buried optic nervedrusen: a case report. Arq Bras Oftalmol. 2022 May-Jun; 85(3):294-296. Figure 3. PMCID: PMC11826757. License: CC BY.
Abnormalities detected by OCT are broadly classified into “thickening” and “thinning”.
RNFL thickening: Reflects axonal edema. Observed in the acute phase of optic neuritis, acute ischemia, and short-term increased intracranial pressure.
RNFL thinning: Reflects loss of ganglion cell axons. Observed in neurodegenerative diseases, toxic/nutritional optic neuropathies, and the chronic phase of inflammatory/ischemic processes, ultimately leading to optic atrophy.
Peripapillary retinal nerve fiber layer (RNFL) thickness: The most valuable structural parameter in neuro-ophthalmology. A ring scan around the optic disc indirectly assesses all RGCs 1).
Sector evaluation: Thickness is measured for the superior, inferior, nasal, and temporal sectors and compared with visual field findings (e.g., inferotemporal RNFL atrophy → superotemporal arcuate scotoma).
Normal database comparison: Compared with a race- and age-matched normal eye database using probability displays. Due to large individual variability, even mild thinning may not be flagged as abnormal, so actual measurement evaluation and inter-eye comparison are necessary.
Macular GCIPL
GCL + IPL (GCIPL): Because most retinal ganglion cells (RGCs) are located in the macula, this measurement is useful for detecting optic nerve damage 1). Depending on the device, it may be reported as GCIPL (GCL+IPL) or GCC (NFL+GCL+IPL).
Advantage in optic disc swelling: In acute stages with optic disc swelling, cpRNFL analysis is difficult, but macular inner retinal layer analysis is less affected by disc swelling and can detect thinning earlier than cpRNFL.
Preceding changes: GCIPL thinning is often detected before RNFL changes (reported in optic neuritis, non-arteritic anterior ischemic optic neuropathy, and compressive optic neuropathy) 1).
OCTA
OCT angiography: Non-invasively visualizes the fine structure of retinal and choroidal blood vessels without the need for contrast agents.
Radial peripapillary capillary (RPC) assessment: Detects vasodilation, tortuosity, and decreased vessel density. Decreased vessel density is observed in areas corresponding to nerve fiber layer defects (NFLD).
Application in neuro-ophthalmology: Used for differential diagnosis and follow-up of non-arteritic anterior ischemic optic neuropathy, papilledema, and optic neuritis1).
QWhat are the differences between RNFL and GCIPL?
A
RNFL contains the axons of retinal ganglion cells (RGCs), while GCIPL includes the cell bodies (GCL) and dendritic synapses (IPL) of RGCs. Both provide complementary information, and which changes first depends on the location and timing of the lesion. In the acute phase with optic disc swelling, GCIPL assessment is more reliable than cpRNFL.
ODD definition: hyporeflective structures located above the lamina cribrosa with hyperreflective margins (recommended by the ODDS Consortium) 1).
Detection of buried ODD: superior to B-scan ultrasound, autofluorescence, and CT, particularly useful in populations with a high prevalence of buried ODD in younger individuals 1).
Correlation with severity: Larger ODD volume correlates with RNFL thinning and visual field defects1).
PHOMS (peripapillary hyperreflective ovoid mass-like structures) should be distinguished from ODD as a separate phenomenon1).
Optic Neuritis, Multiple Sclerosis (MS), and NMOSD
RNFL and GCIPL thinning are established biomarkers in MS and optic neuritis1).
Even MS patients without ocular symptoms show cpRNFL reduction, and postmortem studies have confirmed optic nerve demyelination in 99% of MS patients.
Acute retrobulbar optic neuritis: RNFL thickness may be normal, decreased, or increased (axonal edema). cpRNFL thinning is detected approximately 6 months later.
cpRNFL thickness correlates with best-corrected visual acuity, contrast sensitivity, color vision, EDSS (disability scale), and brain atrophy.
Progressive MS: The rate of RNFL and GCIPL atrophy is faster than in relapsing-remitting MS1).
Inner nuclear layer (INL) volume: It is attracting attention as a marker of CNS inflammatory disease activity1).
NMOSD: Characterized by severe optic atrophy (retinal nerve fiber layer <30 μm), known as the “flooring effect”1). The frequency of microcystic macular edema is higher (20–26%, 40% in AQP4-positive) than in MS (5%)1).
MOG-IgG-related vs AQP4-IgG-related: In MOG-IgG-related optic neuritis, GCIPL is relatively preserved, whereas in AQP4-IgG-related, GCIPL is markedly lost1).
Differentiation between MS and MOGAD: After the first optic neuritis episode, MOGAD patients show worse visual acuity and pRNFL atrophy. The incidence of simultaneous bilateral optic neuritis is 46.9% in MOGAD vs 11.8% in MS (p < .001). Nasal <58.5 μm and superotemporal <105.5 μm are considered independent predictors of MOGAD2).
QIs OCT included in the diagnostic criteria for multiple sclerosis?
A
In the current McDonald criteria (2017 revision), the optic nerve is not included as a DIS (dissemination in space) site, but improved sensitivity by incorporating asymptomatic optic nerve lesions has been reported, and research is ongoing to expand its use for proving DIS and DIT (dissemination in time) in future revisions 1).
Acute phase evaluation: RNFL assessment is limited by optic disc edema, but GCIPL thinning is detected within 1 month of onset and precedes RNFL changes 1).
Altitudinal pattern: GCIPL changes with a “high difference” (one horizontal hemisphere thinner than the other) are characteristic of nonarteritic anterior ischemic optic neuropathy and are useful for differentiating from optic neuritis at 2 weeks after onset 1).
Chronic phase findings: Thinning consistent with horizontal inferonasal defect and horizontal inferior hemianopia is observed.
OCTA findings: Peripapillary vessel density is significantly reduced in non-arteritic anterior ischemic optic neuropathy, and a correlation between changes in vessel flow density and visual acuity improvement has been reported1).
Differentiation of papilledema and pseudopapilledema
Papilledema: cpRNFL elevation is observed. OCT is useful for differentiation from pseudopapilledema (optic disc drusen/crowded disc).
IIH (idiopathic intracranial hypertension): If GCIPL thinning >10 μm is observed 2–3 weeks after diagnosis, it correlates with poor visual function at 1 year1).
Anterior displacement of pRPE/BM: Reflects increased intracranial pressure (ICP) and is also used to evaluate treatment response1).
A decrease in RNFL thickness may indicate a good response to treatment or may indicate neuroatrophy due to axonal damage.
Bowtie atrophy: Observed as RNFL loss when bitemporal hemianopia occurs due to chiasmal compression 1).
GCIPL changes: Show an atrophy pattern respecting the vertical meridian, making correlation with visual field defects straightforward 1).
Early detection: Nasal double thinning of the GCIPL can be detected before RNFL changes, useful for early/mild compression 1).
Postoperative prognosis: Preoperative RNFL thickness ≥70 μm is the only significant predictor of postoperative visual acuity and field improvement (multivariate analysis) 1).
Chiasmal lesions: Selective thinning nasal to the foveal vertical meridian in the macula, and thinning of the temporal and nasal quadrants on cpRNFL are typical findings.
Optic tract syndrome: Presents with hourglass atrophy in the ipsilateral eye and band atrophy in the contralateral eye.
Meta-analyses have shown that GCIPL, RNFL, and choroid are thinner in AD patients1).
Compared to age-matched healthy controls, RNFL thinning in the superior and inferior quadrants is significant, while nasal and temporal quadrants show no difference.
The cup-to-disc (C/D) ratio in AD patients has been reported to be three times that of the control group.
GCIPL changes are associated with cognitive decline and may serve as an early marker of AD progression1).
The degree of RNFL thinning correlates with disease severity and serves as an indicator of progression. A meta-analysis of 13 studies showed that RNFL thickness in PD patients is significantly reduced compared to controls.
REM sleep behavior disorder (RBD)-associated RNFL and GCIPL thinning is attracting attention as a surrogate marker for prodromal PD1).
Ethambutol optic neuropathy: GCIPL changes precede RNFL abnormalities even with a normal fundus1). Changes in GCIPL after ethambutol discontinuation can predict recovery at 12 months1).
Typical pattern: temporal RNFL thinning + diffuse GCIPL thinning + central visual field loss. The same pattern is also seen in vitamin B12 deficiency optic neuropathy1).
LHON (Leber hereditary optic neuropathy): RNFL thickening occurs in the acute phase, followed by thinning. GCIPL thinning precedes RNFL swelling 1).
DOA (dominant optic atrophy): RNFL thinning is seen in the superior and inferior quadrants, differing from the acute thickening in LHON1).
In optic nerve diseases causing central scotoma or cecocentral scotoma, a thinning pattern reflecting damage to the papillomacular bundle (PMB) is observed.
Homonymous hemiatrophy: Observed as a GCIPL thinning pattern 1).
Pre-geniculate lesion vs post-geniculate lesion: In the former, RNFL thinning is detectable immediately. In the latter, it is detected approximately 5 months later due to retrograde trans-synaptic degeneration (RTSD) 1).
There are case reports of GCIPL homonymous hemiatrophy detected even without visual field defects 1).
QCan OCT differentiate between papilledema and optic disc drusen?
A
EDI-OCT can visualize deep ODD and is useful for differentiating papilledema (cpRNFL elevation) from pseudopapilledema (ODD, crowded disc). However, differentiation from crowded disc may be difficult in some cases, and comprehensive judgment with clinical findings is necessary.
Measurement sites: The optic disc and macula are the two basic sites.
cpRNFL thickness program: A ring scan around the optic disc calculates thickness in each sector (superior, inferior, nasal, temporal).
Macular analysis program: Outputs GCC thickness (NFL+GCL+IPL) or GCIPL thickness (GCL+IPL). Names and measurement ranges vary by device.
Normal database comparison: Compared with normal eye databases by race and age, probability is displayed in a color map.
No inter-device compatibility: Since segmentation algorithms and measurement ranges differ between devices, numerical comparison between different devices is not possible. Use of the same device is recommended for longitudinal evaluation.
Supplementary role: OCT is used as an adjunct to visual field testing and clinical examination; diagnosis should not be based solely on OCT.
Types of OCT and Their Uses in Neuro-Ophthalmology
Papilledema vs Pseudopapilledema (ODD, Crowded Disc): EDI-OCT is useful.
Optic Neuritis vs Nonarteritic Anterior Ischemic Optic Neuropathy: Differentiated by GCIPL change patterns (altitudinal vs diffuse)1).
MOGAD vs MS: Differentiated by nasal and superotemporal pRNFL atrophy patterns2).
Preoperative Prognosis Prediction for Compressive Optic Neuropathy: Preoperative RNFL thickness is used for prognosis prediction1).
QCan OCT results be compared between different devices?
A
Because segmentation algorithms and normal databases differ between devices, numerical comparisons between different devices are not possible. Use of the same device is recommended for longitudinal evaluation. For details, refer to the “Diagnosis and Examination Methods” section.
OCT is a technique that detects the optical path difference between the measurement light and the reflected light from the fundus using optical interference, obtaining signal intensity distribution in the depth direction (A-mode). By scanning in the X-Y direction, tomographic images (B-mode) are acquired.
The retinal layers that are preferentially evaluated in neuro-ophthalmology are as follows. In glaucoma and optic nerve diseases, these three layers are preferentially damaged1).
In the McDonald criteria (2017 revision), the optic nerve is not listed as a DIS site, but there are reports that incorporating asymptomatic optic nerve lesions improves sensitivity 1). The expanded use of OCT to demonstrate DIS and DIT is being studied as a future direction 1).
Potential as an early detection tool for neurodegenerative diseases
The association between RNFL thinning and the preclinical stage of AD (amyloid pathology present, normal cognition) is currently considered unclear, and longitudinal studies are needed to establish the utility of OCT as a screening and monitoring tool for AD and PD 1). Its potential as a tool for predicting prodromal PD in patients with RBD is also attracting attention 1).
Although OCT is a very useful examination tool, the following limitations are known.
No pediatric reference data: The normative database is derived from subjects aged 18 years and older.
Anatomical variations: Conditions such as myopia can present with RNFL thinning.
Factors reducing image quality: Opacities of the ocular media, such as corneal disease, cataracts, and vitreous floaters, degrade image quality.
Segmentation errors: These can lead to inaccurate readings and are particularly frequent in highly myopic eyes and tilted optic discs.
Patient cooperation required: Image quality decreases in patients who cannot maintain fixation.
Impact of comorbidities: In elderly patients, interpreting the cause of RNFL thinning becomes difficult due to comorbidities such as glaucoma and Parkinson’s disease.
Floor effect: As thinning progresses, further changes in thickness become undetectable, limiting monitoring in advanced disease 1).
Inter-device incompatibility: The same device must be used for longitudinal comparisons.
Need for comprehensive assessment: Diagnosis should not be based solely on OCT; it should be integrated with clinical examinations and visual field tests.
Lo C, Vuong LN, Micieli JA. Recent advances and future directions on the use of optical coherence tomography in neuro-ophthalmology. Taiwan journal of ophthalmology. 2021;11(1):3-15. doi:10.4103/tjo.tjo_76_20. PMID:33767951; PMCID:PMC7971436.
Pakeerathan T, et al. December 2024 Journal Highlights: differentiation of MS and MOGAD using OCT parameters. 2024.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.