Terson syndrome refers to a condition in which intraocular hemorrhage develops after subarachnoid hemorrhage (SAH), subdural hemorrhage, or intracerebral hemorrhage. The intraocular bleeding often takes the form of vitreous hemorrhage or subinternal limiting membrane hemorrhage, and bleeding can also occur around the optic disc and in various retinal layers of the macula (preretinal, intraretinal, subretinal).1)
In 1900, French ophthalmologist Albert Terson first reported vitreous hemorrhage associated with subarachnoid hemorrhage. Since then, intraocular hemorrhage associated with intracranial hemorrhage has been known as Terson syndrome.
The incidence after traumatic brain injury (TBI) has been reported at about 3.1%. It is lower than SAH (19.3%) and intracerebral hemorrhage (9.1%), but the absolute number cannot be ignored because many patients have TBI.1)
Frequency: about 3-20% of subarachnoid hemorrhage cases. About 3.1% in TBI.1)
Incidence in acute SAH: about 20%
Timing of onset: 2-3 days after intracranial hemorrhage, usually within 2 weeks
In the early stage, it often causes pre-retinal hemorrhage (subinternal limiting membrane hematoma). After that, physical rupture of the internal limiting membrane triggers progression to vitreous hemorrhage. The amount and location of bleeding vary by patient, ranging from mild pre-retinal hemorrhage alone to massive vitreous hemorrhage that prevents a view of the fundus.
QDoes every patient with subarachnoid hemorrhage develop Terson syndrome?
A
No. It is said to occur in 3–20% of subarachnoid hemorrhage cases and in about 20% of acute SAH. Most SAH patients do not develop intraocular bleeding, but it is thought to be more likely when the sudden rise in intracranial pressure is large or when certain anatomical pathways are involved. If vision loss or floaters appear after SAH, prompt ophthalmic evaluation is important.
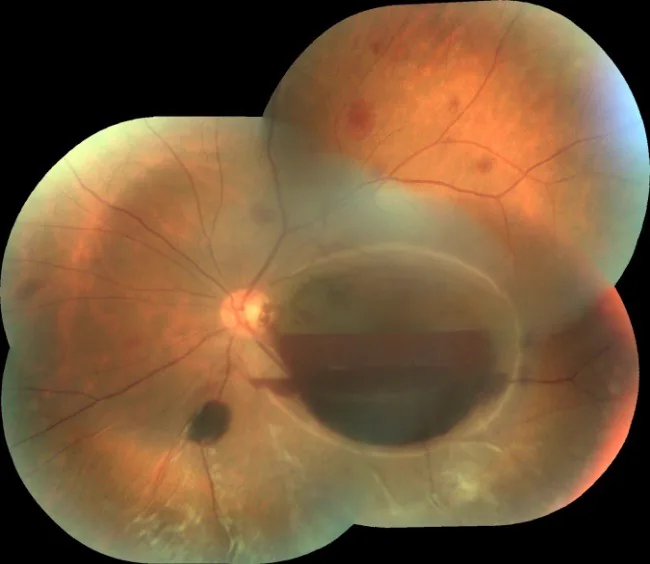
Moraru A, et al. Terson’s Syndrome – case report. Rom J Ophthalmol. 2017;61(1):44–48. Figure 2. PMCID: PMC5710052. License: CC BY.
On the wide-field fundus photograph of the left eye, a large dome-shaped pre-retinal hematoma (subinternal limiting membrane hematoma) is seen centered on the macula, and a clear horizontal two-layer hemorrhage level due to gravitational settling of blood can be identified (upper layer: liquid blood, lower layer: clotted blood). This corresponds to the macular pre-retinal hematoma (subinternal limiting membrane hematoma) discussed in the section “2. Main symptoms and clinical findings.”
The main subjective symptom of Terson syndrome is vision loss that appears after intracranial hemorrhage, usually within 2–3 days after the onset of SAH. When the vitreous hemorrhage is large, vision can drop suddenly and severely, and the fundus cannot be seen. Patients may also complain of floaters. Because symptoms of intracranial hemorrhage (severe headache, altered consciousness, nausea) are prominent, eye symptoms are easily overlooked.
It can occur in one eye or both eyes. In SAH patients with impaired consciousness, a complaint of vision loss may not be obtainable, so ophthalmic screening is important.
Sub-internal limiting membrane hematoma (preretinal hemorrhage): Seen around the optic disc and macula in the early stage after onset. The hematoma appears as a dark red, clearly defined elevation.
Small vitreous hemorrhage: The amount of bleeding may still be enough to see the fundus. This is a stage where spontaneous absorption can be expected.
Intraretinal and subretinal hemorrhage: Bleeding may be seen in the layers from around the optic disc to the macula.
Advanced findings
Large vitreous hemorrhage: When the internal limiting membrane breaks down, bleeding into the vitreous cavity increases rapidly, and the fundus can no longer be seen. Vision may fall to only light perception or worse.
Even after vitreous hemorrhage has spontaneously absorbed, follow-up is needed with attention to epiretinal membrane formation. If vision does not improve after spontaneous absorption and OCT shows an epiretinal membrane or macular edema, surgery should be considered.
QDoes vitreous hemorrhage go away on its own?
A
With mild to moderate vitreous hemorrhage, spontaneous absorption may sometimes be expected. However, absorption can take several weeks to several months, and during that time there is a risk of developing an epiretinal membrane or proliferative vitreoretinopathy. In younger patients in particular, proliferative changes are more likely to occur, so the duration and frequency of follow-up should be carefully considered. In cases of severe vitreous hemorrhage, bilateral involvement, or suspected retinal detachment on B-mode ultrasound, vitrectomy is recommended.
The intracranial hemorrhages that cause Terson syndrome are as follows.
Subarachnoid hemorrhage (most common): The main cause is rupture of a cerebral aneurysm. A sudden rise in intracranial pressure causes bleeding inside the eye.
Traumatic brain injury (TBI): It occurs after head trauma from traffic accidents, falls, drops, or blows. Terson syndrome has been reported to occur in about 3.1% of patients with TBI.1,2)
Subdural hemorrhage: It may be associated with subdural hematoma after head trauma. In infants and young children, retinal hemorrhage is known as an important finding in abusive head trauma (AHT, also called shaken baby syndrome), and differentiation from Terson syndrome becomes an issue.3,4)
Intracerebral hemorrhage: It may occur secondary to hypertensive intracerebral hemorrhage and similar conditions.
SAH severity: In high-grade (severe) cases by the Hunt & Hess classification, intracranial pressure rises sharply, making intraocular hemorrhage more likely.
Young age: Younger patients are more likely to develop proliferative vitreoretinopathy, so vitrectomy should be actively considered.
Time from onset to ophthalmology visit: The longer the time after onset, the higher the risk of proliferative changes. Extra caution is needed when the ophthalmology visit is delayed because of poor general condition.
Diagnosis of Terson syndrome is performed as follows.
Confirm history of intracranial hemorrhage: share the diagnoses of SAH, subdural hemorrhage, and intracerebral hemorrhage with neurosurgery.
Slit-lamp microscopy: evaluate the anterior segment and ocular media.
Fundus examination: perform a dilated fundus examination. If vitreous hemorrhage is severe, viewing the fundus becomes difficult.
B-mode ultrasonography: essential when the fundus cannot be visualized. Evaluate for retinal detachment, proliferative changes, and posterior vitreous detachment. Perform it frequently during follow-up as well so that the appearance of proliferative changes is not missed.
OCT examination: when the fundus can be visualized, it is useful for evaluating sub-internal limiting membrane hemorrhage, epiretinal membrane, and retinal layer structure.
Valsalva retinopathy: Pre-retinal hemorrhage and vitreous hemorrhage that occur after straining (such as weight lifting, vomiting, or coughing). There is no history of intracranial hemorrhage, so the distinction is relatively easy.
Vitreous hemorrhage due to diabetic retinopathy: A history of diabetes and fundus findings (neovascularization, hard exudates, etc.) are key to the distinction.
Retinal vein occlusion (CRVO/BRVO): Characteristic flame-shaped hemorrhages and venous dilation are distinguishing findings. A history of intracranial hemorrhage is required.
Abusive head trauma in infants and young children (AHT, shaken baby syndrome): If bilateral multilayered retinal hemorrhages, retinoschisis, and retinal folds are present together with subdural hematoma and no clear accident history, abuse should be strongly suspected. To distinguish this from Terson syndrome, systematic evaluation in cooperation with imaging studies, skeletal examination, pediatrics, and social welfare is essential.3,4)
When proliferative changes are present, evaluate with the possibility of retinal detachment, subretinal proliferation, and epiretinal membrane in mind. In cases that have passed a long time since onset, or cases that present late because of poor general condition, the risk of proliferative change is higher, so frequent follow-up with B-mode ultrasonography is especially important.
QIs an eye exam always necessary after SAH?
A
Ophthalmic screening for patients with SAH is strongly recommended to detect and manage Terson syndrome. Even in severe cases with impaired consciousness, fundus examination is possible, and early detection of vitreous hemorrhage can help avoid missing the right time for treatment. In particular, when the fundus cannot be viewed, B-mode ultrasonography is needed to check whether there is retinal detachment. A coordinated system involving neurosurgeons and ophthalmologists is required.
Treatment for Terson syndrome is determined by the severity of vitreous hemorrhage, the pattern of onset (unilateral/bilateral), the patient’s age, the length of time since onset, and the presence of complications. Broadly, there are two options: observation and vitrectomy.
Vitrectomy (pars plana vitrectomy: PPV) is performed using a 25G or 27G small-incision system. The main purpose of surgery is to remove the vitreous hemorrhage, which helps restore visual function early and prevent proliferative vitreoretinopathy. Clinical outcomes of vitrectomy for Terson syndrome secondary to TBI are favorable, and early postoperative improvement in vision has been reported in many cases.2,5) Even in pediatric cases, vitrectomy has been reported to yield good anatomic and functional outcomes.6)
The main intraoperative steps are as follows.
Removal of vitreous hemorrhage: the cloudy vitreous is removed to restore visibility of the retina.
Management of the internal limiting membrane (ILM): if an epiretinal membrane is present, membrane peeling is performed. The need for ILM peeling is determined based on intraoperative findings.
Management of retinal detachment: If retinal detachment is confirmed during surgery, retinal reattachment is performed (air, gas, or silicone oil tamponade, and laser photocoagulation if needed).
The timing of surgery is decided individually based on the patient’s general condition, amount of bleeding, presence or absence of complications, and age. Bilateral onset, younger age, severe vitreous hemorrhage, and cases in which retinal detachment is suspected on B-mode ultrasound are considered indications for active early surgery. On the other hand, if mild unilateral vitreous hemorrhage is expected to clear on its own, observation can be chosen. However, even during observation, it is essential to monitor for proliferative changes with frequent B-mode ultrasound examinations. Treatment of the SAH itself takes priority, and the timing of eye surgery is decided after the general condition has stabilized, in consultation with neurosurgery.
6. Pathophysiology and detailed mechanism of onset
Several theories have been proposed for the mechanism of Terson syndrome, and the topic is still debated today. The following three theories are the main ones.
A sudden rise in intracranial pressure caused by subarachnoid hemorrhage compresses the central retinal vein within the optic nerve. As a result, central retinal venous pressure rises, and the retinal capillaries and venules rupture, causing vitreous hemorrhage. This theory emphasizes the mechanism in which sudden changes in intracranial pressure are transmitted to the eye’s blood vessels, and it is consistent with findings that the severity of SAH (the degree of intracranial pressure elevation) correlates with the frequency of Terson syndrome.
This theory holds that blood from the subarachnoid hemorrhage that enters the subarachnoid space around the optic nerve flows directly into the eye through an anatomical pathway. The anatomical continuity between the subarachnoid space and the inside of the eyeball forms the basis for onset. This theory can partly explain the pattern in which blood enters beneath the internal limiting membrane.
This theory proposes that there is a cleft around the portion of the central retinal artery and vein that runs within the optic nerve, and that the distal end of this cleft extends to the area around the vessels near the optic disc. Through this route, blood from the subarachnoid space flows beneath the internal limiting membrane to form a subinternal limiting membrane hemorrhage. Later, physical rupture of the internal limiting membrane causes vitreous hemorrhage. This theory well explains the finding of subinternal limiting membrane hemorrhage (preretinal hemorrhage) as an early sign.
Two other theories are also described below.
The theory that retinal hemorrhage is caused by congestion of the central retinal vein accompanying a sudden rise in intracranial pressure
The theory that blood entering the optic nerve sheath from the subarachnoid space moves along the central retinal vein from the optic disc into the eye, progressing to retinal hemorrhage and vitreous hemorrhage
At present, no single mechanism has been established, and the mechanism involved may differ from case to case. All of these theories share the idea that sudden intracranial changes caused by SAH trigger intraocular hemorrhage.
Risk of proliferative vitreoretinopathy in younger patients
In younger patients, the vitreous has not yet undergone enough liquefaction or posterior vitreous detachment, so blood that has leaked into the eye tends to remain in the vitreous and is more likely to promote the formation of fibrovascular membranes through proliferative stimulation. As a result, proliferative vitreoretinopathy (proliferative vitreoretinopathy: PVR) is more likely to develop, and the risk of progression to tractional retinal detachment or rhegmatogenous retinal detachment is higher. It is important to determine how closely to follow the patient by taking both age and the time since onset into account.
The protocol for routine ophthalmic screening in SAH patients (fundus examination and B-mode ultrasonography) varies by facility, and no unified standard has yet been established. Building a system for cooperation between neurosurgery and ophthalmology in deciding when and how to perform ophthalmic screening in severe SAH patients with impaired consciousness is a future challenge.
There are few large comparative studies that have examined whether early intervention (soon after SAH onset) or elective surgery (after confirming spontaneous absorption) is better for visual prognosis and complication rates in Terson syndrome. In particular, more evidence is needed to clarify the benefits of early surgery in bilateral cases and in younger patients.
Minimally invasive approaches for cases with only subinternal limiting membrane hemorrhage
For cases that show only subinternal limiting membrane hemorrhage without massive vitreous hemorrhage, there are reports of a technique in which Nd:YAG laser is used to create an opening in the internal limiting membrane (a capsulotomy-like approach) to release the hemorrhage into the vitreous cavity. It is attracting attention as a way to rapidly drain the hemorrhage while keeping invasiveness to a minimum, but further verification is needed before it can be established as standard treatment.
Hemorrhage assessment and prognosis prediction using OCT
Three-dimensional evaluation of hematoma beneath the internal limiting membrane using optical coherence tomography (OCT) and OCT angiography (OCTA), along with prediction of visual prognosis based on it, are being studied. Quantifying the amount of bleeding, layer-by-layer distribution, and structural changes in the fovea may improve the accuracy of decisions about surgical indications.
Neurosurgery and ophthalmology collaboration protocol
By developing a standard protocol that defines the timing, methods, and frequency of ophthalmic evaluation after the onset of SAH, Terson syndrome may be detected more reliably and visual outcomes may improve. Building a team-based approach involving emergency care, intensive care, neurosurgery, and ophthalmology is recognized as a future challenge.
Czorlich P, Skevas C, Knospe V, et al. Terson syndrome in subarachnoid hemorrhage, intracerebral hemorrhage, and traumatic brain injury. Neurosurg Rev. 2015;38(1):129-136. PMID: 25173620. 1)
Narayanan R, Taylor SC, Nayaka A, et al. Visual Outcomes after Vitrectomy for Terson Syndrome Secondary to Traumatic Brain Injury. Ophthalmology. 2017;124(1):118-122. PMID: 27817917. 2)
Togioka BM, Arnold MA, Bathurst MA, et al. Retinal hemorrhages and shaken baby syndrome: an evidence-based review. J Emerg Med. 2009;37(1):98-106. PMID: 19081701. 3)
Squier W. Retinodural haemorrhage of infancy, abusive head trauma, shaken baby syndrome: The continuing quest for evidence. Dev Med Child Neurol. 2024;66(3):290-297. PMID: 37353945. 4)
Citirik M, Tekin K, Teke MY. Terson syndrome with persistent vitreous hemorrhage following traumatic brain injury. Saudi J Ophthalmol. 2019;33(4):392-397. PMID: 31920451; PMCID: PMC6950947. 5)
Sayman Muslubas I, Karacorlu M, Hocaoglu M, Ersoz MG, Arf S. Anatomical and functional outcomes following vitrectomy for dense vitreous hemorrhage related to Terson syndrome in children. Graefes Arch Clin Exp Ophthalmol. 2018;256(3):503-510. PMID: 29288413. 6)
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.