Bacillary Layer Detachment (BALAD) is an OCT finding showing a separation within the retina occurring between the external limiting membrane (ELM) and the ellipsoid zone (EZ)—that is, at the site of the photoreceptor inner segment myoid zone (MZ) 5).
The term “bacillary” originates from neuroanatomist Polyak’s 1941 definition of the photoreceptor inner and outer segments (IS-OS) as the “bacillary layer.” BALAD was formally named in 2018 when Mehta et al. reported this OCT finding in patients with toxoplasmosis and pachychoroid disease 1),3),5),9).
Although the incidence is rare, reports are increasing annually. In exudative AMD (nAMD) cohorts, the incidence is 4.5% (20 of 442 eyes), and in the HAWK trial it was reported as 7.2% 4). In Vogt-Koyanagi-Harada disease, a high incidence of 47% has been shown 9), and the frequency varies greatly by disease category. The disease-specific frequencies in reported cases are: VKH 47%, APMPPE 11%, sympathetic ophthalmia 7.3%, choroidal neovascularization 6.2%, toxoplasmosis 5.5%, and AIm 5.5% 9).
The first report of “intraretinal fluid accumulation in the outer retina” was by Maruyama & Kishi in 2009, in patients with Vogt-Koyanagi-Harada disease9).
QHow common is BALAD as an OCT finding?
A
In nAMD, it is found in 4.5–7.2% of cases; in Vogt-Koyanagi-Harada disease, up to 47%. It is a rare but important finding, often appearing in the acute or exudative phase of the disease.
Subjective symptoms depend on the underlying disease. Representative examples are shown below.
Decreased visual acuity: The most common complaint. In BALAD associated with nAMD, the mean best-corrected visual acuity is 20/138, with a wide range from CF to 20/4001),4),5).
Intact foveal roof type: The foveal roof is preserved. Good recovery can be expected with scleral buckling.
Lamellar type (foveal roof loss type): The foveal roof is lost. There is a risk of progression to full-thickness macular hole (FTMH).
QHow to differentiate BALAD from usual serous retinal detachment (SRF) on OCT?
A
SRF is a hyporeflective fluid space between the RPE and neurosensory retina. In contrast, BALAD is a separation occurring between the ELM and EZ (myoid), and it also differs in that it contains hyperreflective material of moderate reflectivity within the cavity. Judgment is made based on both location and reflectivity characteristics.
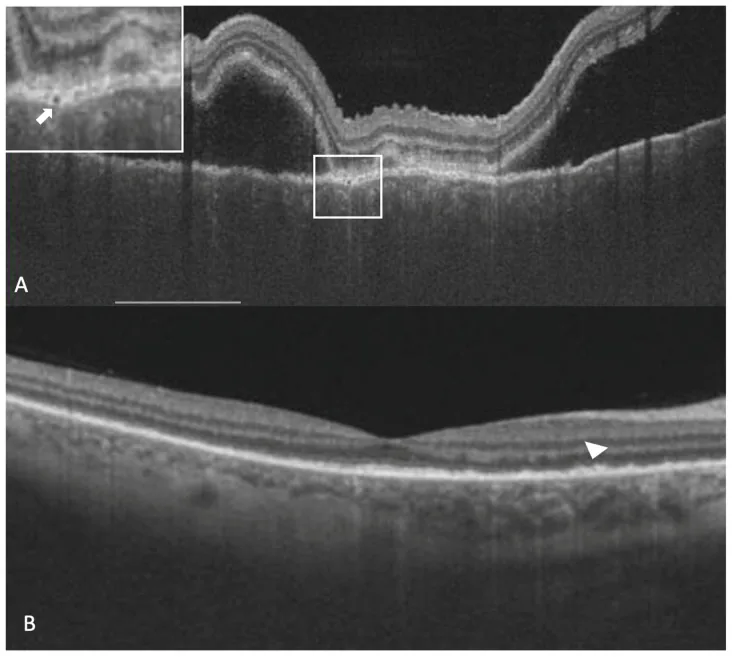
Ninan Jacob; Mudit Tyagi; Jay Chhablani; Raja Narayanan; Anup Kelgaonkar; Mukesh Jain. Retinal Pigment Epithelial Characteristics in Acute and Resolved Vogt-Koyanagi-Harada Disease. J Clin Med. 2023 Mar 19; 12(6):2368 Figure 3. PMCID: PMC10054856. License: CC BY.
A 26-year-old lady with a diagnosis of acute Vogt-Koyanagi-Harada disease. The right eye shows sub-retinal fluid, thickened choroid, a thickened retinal pigment epithelium (RPE) and an RPE vacuolation (white arrow in the white box inset at the top left corner) in the vertical optical coherence tomography scan (A). After the resolution of sub-retinal fluid, persistent deposits over RPE could be noticed (arrowhead) (B).
The first-line treatment for nAMD is anti-VEGF intravitreal injection, and BALAD disappears rapidly after treatment1),4),5). The main drugs and doses are as follows5).
bevacizumab: 1.25 mg/0.05 mL
ranibizumab: 0.5 mg/0.05 mL
aflibercept: 2.0 mg/0.05 mL
Jung JJ et al. (2021) reported two cases in which BALAD completely disappeared after a single bevacizumab injection5). In the first case, best-corrected visual acuity improved from 20/80 to 20/25, and in the second case, from 20/160 to 20/50. A case has also been reported in which CRT decreased from 929 μm to 310 μm and best-corrected visual acuity improved from CF to 20/50 after six aflibercept injections4).
Desai & Tyagi (2023) reported that in toxoplasmic retinochoroiditis, TMP-SMX (160/800 mg twice daily for 2 months) alone resulted in persistent inflammation and enlargement of BALAD, but the addition of prednisolone 50 mg/day led to resolution of BALAD within one week 3).
For tuberculous SLC, combination therapy with ATT (rifampicin + isoniazid + pyrazinamide + ethambutol) plus prednisone 60 mg/day has been reported to resolve BALAD within 2 months 6).
Laser photocoagulation (532 nm, 250 μm, 50 mW, 200 ms) for CSCR-related BALAD associated with high hyperopia has been reported to resolve BALAD within 16 days 7). In CSCR patients using steroids, discontinuation of steroids should be considered 8).
Surgical Treatment for Rhegmatogenous Retinal Detachment-Related BALAD
Intact foveal roof type: Scleral buckling results in good visual function recovery (best corrected visual acuity 20/200 → 20/25, foveal thickness 80 → 166 μm).
Lamellar type: Because there is a risk of progression to FTMH after scleral buckling, vitrectomy + ILM peeling + inverted flap technique is recommended.
Intravitreal injection of voriconazole 100 μg/0.05 mL combined with systemic antifungal therapy has been reported to resolve BALAD within 3 weeks 9).
QCan BALAD be cured with treatment?
A
BALAD often resolves with treatment of the underlying disease. In nAMD, anti-VEGF injections; in inflammatory diseases, steroids and antibiotics can make BALAD disappear. However, even after BALAD resolves, long-term visual impairment may persist, for example, 77% of nAMD cases develop subretinal fibrosis within 4 years 4).
The inner segment (IS) of photoreceptors is functionally divided into two zones.
Myoid zone (MZ): Contains Golgi apparatus, ribosomes, and endoplasmic reticulum (ER). Structurally, it is not as robust as the ELM or EZ, and is prone to artificial cleavage in tissue specimens 5),9).
Ellipsoid zone (EZ): Contains dense mitochondria and forms a hyperreflective line on OCT.
The structural vulnerability of the MZ provides the anatomical basis for BALAD formation.
Rapid influx of proteinaceous fluid through defects in the RPE/Bruch membrane complex elevates the ELM. Additionally, subretinal hemorrhage may form fibrin adhesions between the EZ and RPE, leading to cleavage in the MZ 5).
Tangential forces at the macula are thought to disrupt the Müller cell cone, leading to ELM detachment and splitting in the MZ 2).
Govetto et al. (2023) proposed the possibility of a “foveation mechanism” in which healthy parafoveal cones migrate centripetally to reconstruct the fovea during BALAD repair after rhegmatogenous retinal detachment2). Since post-mitotic cones cannot replicate, this hypothesis suggests foveal regeneration through migration rather than new formation.
QWhy does splitting occur in the myoid of the photoreceptor inner segment?
A
The myoid zone (MZ) is structurally less robust than the ELM or EZ and represents an anatomical weak point. It is known that artificial separation easily occurs at this site in tissue specimens 5),9). When hydrostatic pressure from the choroid increases, splitting occurs at this weak point, leading to BALAD formation.
7. Latest research and future perspectives (reports at research stage)
Flindris et al. (2025) reported that BALAD associated with nAMD is a biomarker indicating an aggressive disease phenotype 4). It was shown that 77% of nAMD eyes with BALAD developed subretinal fibrosis within 4 years. This suggests that BALAD may serve not only as an OCT finding but also as a prognostic indicator.
In more than half of BALAD cases, gradual recovery of EZ and IZ is observed 9). Since cone photoreceptors are post-mitotic and cannot replicate, the aforementioned foveation mechanism (centripetal migration for foveal reconstruction) may be key to recovery 2).
The precise histopathological correlation of BALAD remains unestablished 1),4),5). Currently, most reports are case reports or small case series, and large-scale prospective studies are needed to elucidate the natural course and prognostic factors of BALAD.
Palmieri F, Younis S, Raslan W, Fabozzi L. Bacillary layer detachment in neovascular age-related macular degeneration: case series. Biomedicines. 2023;11(3):988.
Govetto A, Radice P, Lucchini S, et al. Recovery of bacillary layer detachment associated with macula-off rhegmatogenous retinal detachment: evidence of foveation mechanisms? Am J Ophthalmol Case Rep. 2023;32:101923.
Desai A, Tyagi M. Bacillary layer detachment as an inflammatory biomarker in toxoplasmosis retinochoroiditis: serial evolution on optical coherence tomography. BMJ Case Rep. 2023;16:e256629.
Jung JJ, Soh YQ, Yu DJG, et al. Bacillary layer detachment due to macular neovascularization. Retina. 2021;41(10):2106-2114.
Socci da Costa D, Gomes e Silva A, Melichar A, et al. Bacillary layer detachment in serpiginous-like choroiditis of presumed intraocular tuberculosis: Report of two cases. Am J Ophthalmol Case Rep. 2022;27:101653. doi:10.1016/j.ajoc.2022.101653.
Murillo SA, Medina SP, Romero RM, Murillo FH. Bacillary layer detachment in an atypical case of central serous chorioretinopathy associated with high hyperopia. Case Rep Ophthalmol. 2022;13:504-510.
Fuganti RM, Casella AM, Roisman L, et al. Case series bacillary layer detachment associated with acute central serous chorioretinopathy in patients with COVID-19. Am J Ophthalmol Case Rep. 2022;28:101690.