A shallow anterior chamber is a condition in which the anterior chamber depth (ACD), the space between the corneal endothelium and the iris/lens anterior surface, is shallower than normal. Generally, a central anterior chamber depth < 2.5 mm is considered a guideline, but in elderly hyperopic eyes with a short axial length, it may be relatively shallow even within the normal range.
In primary angle-closure disease (PACD), characteristic anatomical structures such as a shallow anterior chamber, short axial length, and a relatively thick lens positioned anteriorly are observed. A shallow anterior chamber is not a disease in itself but appears as a clinical sign of various conditions, including angle-closure disease. It is often managed as a continuum from PACS to PAC to PACG.
Approximately 0.7% of people aged 40 and older worldwide have primary angle-closure glaucoma (PACG), with an estimated 20.2 million patients, of whom about 15.5 million are Asian 2). With aging, the lens thickens and shifts forward, and the anterior chamber naturally tends to become shallower.
Risk factors
Details
Sex and age
More common in elderly women
Refraction and eye shape
Hyperopia, short axial length, small corneal diameter, lens thickening
Family history
First-degree family history of angle-closure glaucoma
Race
Higher prevalence in Asians (Chinese, Japanese) and Inuit2)
QI was told I have a shallow anterior chamber. Do I need immediate treatment?
A
In the shallow anterior chamber stage (PACS), most patients are asymptomatic and immediate treatment is not always necessary. However, prophylactic laser iridotomy (LI) has been reported to reduce the risk of developing PAC by 47% at 6 years and 70% at 14 years2). Progression from PACS to PAC/acute attack is relatively rare, occurring in about 4% at 6 years and 12% at 14 years. However, it is important to decide on a management plan in consultation with an ophthalmologist, considering factors such as family history, frequency of mydriatic use, and difficulty in accessing medical care.
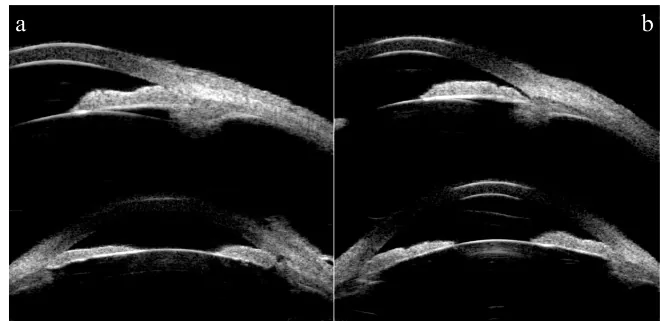
Lv K, et al. Unilateral pigmented paravenous retinochoroidal atrophy with acute angle-closure glaucoma: a case report. BMC Ophthalmol. 2023. Figure 3. PMCID: PMC10169484. License: CC BY.
Anterior segment UBM shows a short distance between the posterior corneal surface and the anterior surfaces of the iris and lens, indicating a shallow anterior chamber. The anterior chamber angle is also narrowed, providing diagnostic findings for shallow anterior chamber.
Symptoms of shallow anterior chamber are broadly classified into acute and chronic types depending on the cause and course.
In acute primary angle closure (APAC) attacks, a rapid and severe elevation of intraocular pressure to 40–80 mmHg occurs, requiring emergency ophthalmic management.
Subjective symptoms:
Sudden eye pain and periorbital pain (may be misdiagnosed as gastrointestinal disease or migraine)
Headache, nausea, vomiting (vagal reflex)
Blurred vision, sudden vision loss (due to corneal edema)
Halos around lights (rainbow-colored rings around light sources)
Objective findings:
Severely shallow anterior chamber (ACD approximately 1.4 mm during an attack, sometimes with corneal–iris contact)
Chronic shallow anterior chamber is often asymptomatic and may go unnoticed until moderate intraocular pressure elevation of 20–30 mmHg or visual field changes are detected. Slit-lamp microscopy reveals a shallow peripheral anterior chamber, and screening is performed using the van Herick method and gonioscopy.
QWhat should be done if sudden eye pain with headache and nausea occurs?
A
This may indicate an acute angle-closure glaucoma attack. If severe unilateral eye pain, headache, nausea, along with decreased vision, blurred vision, and colored halos appear simultaneously, immediate ophthalmic emergency care should be sought. Intraocular pressure can rapidly rise to 40–80 mmHg, and irreversible optic nerve damage can occur within hours without treatment. Self-medication with over-the-counter drugs is dangerous; prompt ophthalmic intervention (eye drops, intravenous medication, laser treatment) is necessary.
Mechanism: Secondary shallow anterior chamber due to forward displacement of posterior ocular tissues.
Malignant glaucoma: Anterior rotation of the ciliary body or abnormal aqueous flow into the vitreous cavity → forward displacement of the vitreous → circumferential shallow anterior chamber.
Choroidal hemorrhage, choroidal detachment, and intraocular tumors (choroidal elevation).
④Postoperative and traumatic causes
Mechanism: Shallow anterior chamber due to low intraocular pressure, wound leakage, or tissue damage
Overfiltration after filtering surgery (hypotony), inadequate watertightness of corneal incision, postoperative choroidal detachment, after ocular trauma.
After filtering surgery in eyes with chronic angle-closure, the risk of shallow anterior chamber, choroidal detachment, and malignant glaucoma is particularly high.
⑤ Inflammatory
Mechanism: Anterior displacement of posterior ocular tissues due to edema and inflammation
Harada disease (Vogt-Koyanagi-Harada disease): Angle closure caused by choroidal and ciliary body edema. Bilateral, with systemic symptoms (headache, tinnitus, skin manifestations).
Secondary glaucoma associated with uveitis may also present with a shallow anterior chamber.
Multiple mechanisms are involved in the development of angle-closure glaucoma1).
Relative pupillary block: The most common mechanism. Increased posterior chamber pressure at the iris-lens contact area leads to forward bowing of the iris and trabecular meshwork obstruction.
Plateau iris: Anterior positioning of the ciliary processes causes the iris root to bend forward. Mydriasis directly closes the angle. Intraocular pressure elevation persists even after laser iridotomy.
Lens-related factors: Angle narrowing due to anterior lens displacement or age-related lens thickening.
Retrolenticular factors (ciliary body factors): Angle closure due to anterior ciliary body displacement or increased vitreous pressure.
Secondary angle closure can be caused by intumescent cataract, lens dislocation, topiramate or sulfonamide drugs (inducing ciliary body edema), scleral buckle surgery, and panretinal photocoagulation2).
QWhich medications can trigger shallow anterior chamber or acute attack?
A
Drugs with mydriatic effects or those that induce ciliary body edema are dangerous. These include anticholinergics (butylscopolamine, scopolamine, antihistamines, antipsychotics), sympathomimetics (nasal decongestants), tricyclic antidepressants, SSRIs, topiramate, and sulfonamide drugs2)3). Mydriasis triggers attacks because pupillary block is maximal at mid-dilation (4–6 mm). If shallow anterior chamber or angle closure is noted, it is important to consult an ophthalmologist before using these medications.
This is a non-contact screening examination using only a slit-lamp microscope. The patient’s eye is kept in primary gaze, and a thin slit beam is directed at the temporal corneal limbus at a 60-degree oblique angle. The peripheral anterior chamber depth (ACD) is evaluated as a ratio to the peripheral corneal thickness (CT). It does not require a gonioscope or special equipment and is widely used for screening angle closure.
Grade
ACD/CT Ratio
Likelihood of Angle Closure
4
≥ 1
Almost none
3
1/4 to less than 1
Low
2
= 1/4
Possible (indication for detailed examination)
1
< 1/4
High
0
0 (contact)
Occluded
Grade 2 or lower (ACD/CT ≤ 1/4) indicates possible angle closure, and gonioscopy should be performed. However, in plateau iris, the central anterior chamber is relatively deep, so it may be missed on screening, requiring caution.
Gonioscopy (Gold standard for definitive diagnosis)
Gonioscopy is the clinical standard for angle evaluation. It is performed in a dark room using a thin slit beam, taking care to avoid illuminating the pupil, and evaluating all four quadrants.
Static gonioscopy: Evaluate angle opening using the Shaffer-Kanski classification, Scheie classification, or Spaeth classification.
Dynamic/indentation gonioscopy: Differentiate between appositional closure and synechial closure (peripheral anterior synechiae = PAS)2)
If ITC extends 180 degrees or more across two or more quadrants, it is diagnosed as angle closure.
It can scan all four quadrants simultaneously without contact. It can be performed by a technician and is suitable for dynamic evaluation of angle changes under both dark and light conditions.
Quantitative evaluation indices (all still under development) 2):
Angle opening distance (AOD)
Trabecular-iris space area (TISA)
ITC index (iris-trabecular contact area)
Anterior lens vault (ALV)
Although there may be discrepancies with gonioscopy, it is useful for tracking changes over time 2). It cannot assess color information, neovascularization, or angle nodules, and does not replace gonioscopy.
It is the only examination method that can evaluate the ciliary body and the posterior surface of the iris. It is essential for diagnosing plateau iris and malignant glaucoma.
The central anterior chamber is relatively deep, and the central iris is flat.
The iris root is thick and bends forward, narrowing the angle recess.
Anterior displacement of the ciliary body and obliteration of the ciliary sulcus.
“Double hump sign”: a peripheral hump from the ciliary processes and a central hump from the lens 2)
Plateau iris is thought to be involved in about one-third of cases where ITC persists after LI2). It is superior to AS-OCT in identifying plateau iris2).
ITC: iridotrabecular contact. Assessed by gonioscopy or AS-OCT2).
Key points for differential diagnosis:
Malignant glaucoma: Shallow anterior chamber and high intraocular pressure persist after LI. UBM shows abnormal aqueous flow into the vitreous cavity.
Choroidal hemorrhage: Acute onset after surgery. Confirmed by B-scan ultrasound. Intraocular pressure may be low to normal.
Harada disease: Characterized by bilateral involvement, systemic symptoms (headache, tinnitus, skin vitiligo), and ciliary body edema.
Lens subluxation: Suspect when there is a deep anterior chamber in one eye combined with an open angle 3).
QHow does anterior segment OCT differ from gonioscopy?
A
Anterior segment OCT (AS-OCT) is non-contact, can be performed by technicians, imposes less burden on patients, and is excellent for quantitative assessment and longitudinal follow-up. In contrast, gonioscopy allows observation of iris color, neovascularization, and angle nodules, and can differentiate appositional closure from PAS using compression. Currently, gonioscopy remains the gold standard for definitive diagnosis. A practical approach is to use AS-OCT for screening and then perform gonioscopy for detailed examination when abnormalities are found 2).
Contraindicated or use with caution in heart failure or renal impairment
Glycerol
300–500 mL intravenously over 45–90 minutes
Monitor for hyperglycemia in diabetic patients
1–2% Pilocarpine hydrochloride
Instill every 20–30 minutes (2–3 times per hour)
Ineffective when sphincter paralysis occurs due to high intraocular pressure. May worsen pupillary block by forward movement of the ciliary muscle 1)
Acetazolamide
10 mg/kg IV or oral
Monitor for metabolic acidosis and electrolyte abnormalities
Corticosteroid eye drops
Usual concentration as appropriate
To reduce inflammation
Note that when the iris sphincter is paralyzed due to high intraocular pressure, frequent administration of pilocarpine is ineffective and may worsen pupillary block by anterior movement of the ciliary muscle1).
Alternative rapid intraocular pressure reduction methods
This is chosen when drug therapy is insufficient or when rapid corneal clearing is needed.
Anterior chamber paracentesis (ACP): Paracentesis of the anterior chamber with a 30G needle. Can immediately normalize intraocular pressure to 12–15 mmHg3)
Argon laser peripheral iridoplasty (ALPI): Contractile laser irradiation to the peripheral iris mechanically opens the angle. RCTs have confirmed a safe reduction in intraocular pressure within 15–30 minutes3)
Laser pupilloplasty (LPP): Contracts and everts the iris at the pupillary margin using a 532 nm laser to relieve pupillary block3)
This is the definitive treatment for relieving pupillary block and is rated as recommendation grade 1A in the 5th edition of the Glaucoma Practice Guidelines1).
Perform after the cornea has become sufficiently clear
If the cornea is opaque, consider surgical peripheral iridectomy
Laser used: Nd:YAG laser (alone or combined with argon + YAG)
Replacing the lens with an intraocular lens increases anterior chamber depth and fundamentally resolves pupillary block (recommendation grade 1A)1). In the acute phase, the risk of intraoperative complications is high, and an experienced surgeon is recommended (recommendation grade 1B)1).
Management of PACS (primary angle closure suspect)
Prophylactic LI for PACS reduces the risk of developing PAC by 47% at 6 years and 70% at 14 years2)
However, progression from PACS to PAC/acute attack is relatively rare, occurring in about 4% at 6 years and about 12% at 14 years2)
The indication for prophylactic LI is determined by considering individual circumstances (family history, frequency of mydriatic use, difficulty in accessing medical care)1)2).
If elevated intraocular pressure persists after LI relieves pupillary block, additional medical or surgical treatment for residual glaucoma is added1).
EAGLE trial (Lancet 2016): A multicenter RCT comparing early lens extraction (phaco-IOL) with LI for PAC (IOP ≥ 30 mmHg) and PACG (IOP ≥ 21 mmHg). At 3 years, the early lens extraction group had approximately 10 times better medication-free IOP control than the LI group, and QOL measures were significantly better4). Based on these results, lens reconstruction is recommended as first-line treatment for APAC patients1).
Aqueous outflow reconstruction procedures (goniosynechialysis, trabeculotomy, MIGS) are indicated for cases with extensive PAS1).
Laser gonioplasty (LGP): First-line treatment. Using an argon laser with a spot size of 500 μm, duration 0.2–0.5 seconds, and power starting at 200 mW, adjust power based on iris response. Apply to half to full circumference of the peripheral iris, aiming for 15 shots per quadrant.
Miotics (e.g., pilocarpine): Pull the peripheral iris to widen the angle 1).
Lens extraction: Expected to widen the angle by retracting the ciliary processes 1).
QWhy does cataract surgery improve shallow anterior chamber?
A
Replacing the aged lens (approximately 5 mm thick) with a thin intraocular lens (approximately 0.5–1 mm) increases anterior chamber depth by an average of 1–2 mm. Additionally, in eyes with angle closure, lens extraction causes the ciliary processes to move posteriorly, further widening the angle. This dual mechanism relieves pupillary block, normalizing anterior chamber depth and opening aqueous outflow pathways. The EAGLE study demonstrated in a large RCT that this effect significantly surpasses that of LI alone 4).
Relative pupillary block is the most common mechanism of angle-closure disease.
The flow of aqueous humor from the posterior chamber through the pupil to the anterior chamber is blocked at the contact surface between the back of the iris and the front of the lens.
Posterior chamber pressure increases, causing the iris to bulge forward (iris bombe).
The peripheral iris almost completely covers the trabecular meshwork, leading to angle closure.
Vicious cycle: forward movement of the lens → increased iris-lens contact area → enhanced pupillary block → further iris bulging.
Pupillary block is most likely to occur when the pupil is mid-dilated (diameter 4–6 mm), as the iris-lens contact area is maximal at this size2).
This is the pathophysiological basis for why mydriatics, anticholinergics, and dark environments at night can trigger acute attacks.
Dynamic changes in the choroid may contribute to acute angle closure attacks. Imaging studies have reported a mechanism in which choroidal expansion during intraocular pressure elevation increases posterior pressure, pushing the lens-iris diaphragm forward and triggering angle closure 3). This is considered one of the reasons why acute attacks tend to occur at night (in darkness) and in a face-down position (choroidal congestion).
Changes in anterior chamber depth after cataract surgery
Cataract surgery replaces the thickened lens with a thin intraocular lens, which not only increases anterior chamber depth but also, in eyes with angle closure, causes the ciliary processes to move posteriorly after lens extraction, further widening the angle. This dual mechanism supports the high efficacy of early lens extraction demonstrated in the EAGLE trial4).
Expansion of indications for early lens extraction: Based on the results of the EAGLE trial, further expansion of the indications for early lens extraction in mild PAC/PACG is being considered4). The APACG consensus recommends early lens extraction 1–3 months after an acute attack, as LI alone leads to progression to CACG in up to 58% of cases after APACA3)
Combined surgery with MIGS: Combinations of lens extraction with goniosynechialysis (GSL), goniotomy, trabecular microbypass stent, and endoscopic cyclophotocoagulation (ECP) are being studied. Phaco-goniotomy for PACG has been reported to have fewer complications and better QOL compared to phaco-trabeculectomy2)
AI-based screening for PACD: Machine learning of AS-OCT images for automated detection and risk stratification of angle closure is under research
Epidemiology of drug-induced angle closure: Data accumulation on the risk of angle closure due to SSRIs and nasal decongestants is ongoing3)
Gedde SJ, Chopra V, Vinod K, et al. Primary Angle-Closure Disease Preferred Practice Pattern®. Ophthalmology. 2026;133(2):P154-P200.
Chan PP, Zhang X, Aung T, Chew PTK, Congdon N, Dada T, Fang SK, He M, et al. Controversies, consensuses, and guidelines for acute primary angle closure attack (APACA) by the Asia-Pacific Glaucoma Society (APGS) and the Academy of Asia-Pacific Professors of Ophthalmology (AAPPO). Asia-Pacific journal of ophthalmology (Philadelphia, Pa.). 2025;14(6):100223. doi:10.1016/j.apjo.2025.100223. PMID:40615047.
Augusto Azuara-Blanco, Jennifer Burr, Craig Ramsay, David Cooper, Paul J Foster, David S Friedman, et al. Effectiveness of early lens extraction for the treatment of primary angle-closure glaucoma (EAGLE): a randomised controlled trial. The Lancet. 2016;388(10052):1389-1397. doi:10.1016/s0140-6736(16)30956-4.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.