
Iridoschisis
1. What is Iridoschisis?
Section titled “1. What is Iridoschisis?”Iridoschisis is a rare degenerative disease in which the iris stroma separates into anterior and posterior layers, with the anterior stromal fibers breaking down into thin fibrils whose free ends float in the aqueous humor. The name is derived from the Greek words iris (iris) and schisis (separation).
Schmitt reported the first case in 19221), and Loewenstein and Foster named it “iridoschisis” in 1945. Histological studies of bilateral iridoschisis revealed deep clefts between the anterior and posterior stroma1). Since then, case reports and small case series have been accumulating.
The disease follows a chronic progressive course, but in many cases it is asymptomatic and discovered during health checkups or examinations for other diseases. It often occurs bilaterally, but the degree of progression may differ between eyes.
2. Epidemiology
Section titled “2. Epidemiology”- Prevalence: More than 100 cases have been reported in the literature, but it is a very rare disease and the exact prevalence is unknown.
- Age of onset: It commonly occurs in elderly individuals aged 50–80 years. A systematic review reported a mean age of 66.95 ± 17.39 years4).
- Sex difference: A systematic review showed a slight female predominance4). The difference in age distribution is important for distinguishing it from progressive iris atrophy (ICE syndrome).
- Ocular characteristics: It is more common in eyes with shallow anterior chamber, short axial length, and hyperopia1).
- Glaucoma association: It is frequently associated with angle-closure glaucoma2). The frequency varies in the literature.
- Cataract association: It is associated with a higher rate of cataract compared to age-matched cohorts4).
- Bilaterality: It often occurs bilaterally, but the degree of progression may be asymmetric.
- Predilection site: It commonly occurs in the lower part of the iris (inferonasal to inferotemporal quadrant)6).
Heredity is generally not confirmed. Age-related degeneration of iris tissue is considered the main cause. A few families with autosomal dominant inheritance have been reported, but the vast majority of cases are sporadic in clinical practice, and there is currently insufficient evidence to explain it to patients as a hereditary disease.
3. Pathophysiology (Separation and Fibrillation of Iris Stroma)
Section titled “3. Pathophysiology (Separation and Fibrillation of Iris Stroma)”Anatomy and age-related changes of the iris
Section titled “Anatomy and age-related changes of the iris”The iris stroma is anatomically composed of the anterior leaf (anterior border layer + anterior iris stroma: melanocytes, fibroblasts, collagen, blood vessels) and the posterior leaf (posterior iris stroma + dilator muscle + two layers of iris pigment epithelium). With aging, microvessels in the iris stroma undergo degenerative changes, leading to progressive ischemia and atrophy.
Electron microscopy reveals a marked decrease in collagen fibers and thinning of the stroma in affected areas, while blood vessels and nerves maintain a normal appearance 1). These changes lead to weakening of the adhesion between the anterior and posterior layers. Iris fluorescein angiography shows preserved vascular perfusion in the separated areas, making ischemia alone an unlikely cause. This is an important distinguishing feature from essential iris atrophy (a type of ICE syndrome).
Progression from separation to fibrillar degeneration
Section titled “Progression from separation to fibrillar degeneration”- The adhesion between the anterior and posterior layers weakens, and separation progresses due to aqueous humor convection (forces that sway the iris plane back and forth).
- A leading theory is that age-related hardening of iris vessels induces shear stress during dilation and constriction, leading to stromal separation.
- The separated collagen fibers of the anterior leaf unravel and become free in the aqueous humor, presenting a characteristic “shredded wheat” appearance 1).
- The posterior pigment epithelial layer is usually intact 6).
Etiological hypotheses
Section titled “Etiological hypotheses”The etiology of iris schisis cannot be explained by a single theory 1).
- Age-related changes: The theory of iris vessel hardening and shear stress is prominent.
- Trauma/mechanical irritation: Bilateral iris schisis and partial lens dislocation have been reported in a patient who continuously used a neck massager on the eye 1). Repeated mechanical friction can cause iris stromal separation.
- Atopic dermatitis: Chronic eye rubbing may cause mechanical trauma leading to iris schisis 3).
- Plateau iris configuration: Coexistence of iris schisis and plateau iris has been reported, suggesting an etiology related to congenital anatomical abnormalities rather than aging.
- Others: Reports include syphilitic interstitial keratitis, long-term use of miotics, and familial cases (extremely rare).
4. Related Diseases
Section titled “4. Related Diseases”Angle-Closure Glaucoma
Section titled “Angle-Closure Glaucoma”Anatomical features such as shallow anterior chamber, short axial length, and hyperopia are common risk factors for both iridoschisis and angle-closure glaucoma. The underlying ocular structure involves a broad area of contact between the iris and lens, predisposing to pupillary block (increased resistance to aqueous humor flow at the pupillary margin). Furthermore, accumulation of free fibers from the anterior iris leaf in the angle accelerates obstruction, and the two factors synergistically elevate intraocular pressure2).
Exfoliation Syndrome (PEX)
Section titled “Exfoliation Syndrome (PEX)”This condition should be differentiated as a cause of secondary glaucoma in elderly patients presenting with white deposits on the anterior lens capsule and pupillary margin. It is distinguished from iridoschisis by the absence of free iris fibers.
Trauma and Mechanical Irritation
Section titled “Trauma and Mechanical Irritation”Repeated use of neck massagers on the eye or chronic eye rubbing due to atopic dermatitis may be associated with the development of iridoschisis1)3). In cases complicated by atopic dermatitis, the prognosis for corneal transplantation is extremely poor3).
Corneal Endothelial Disorders and Conditions Requiring Corneal Transplantation
Section titled “Corneal Endothelial Disorders and Conditions Requiring Corneal Transplantation”Floating iris fibers mechanically damage the corneal endothelium, and if progressive, can lead to corneal endothelial decompensation (bullous keratopathy). This may be an indication for DSAEK or DMEK5).
5. Clinical Features
Section titled “5. Clinical Features”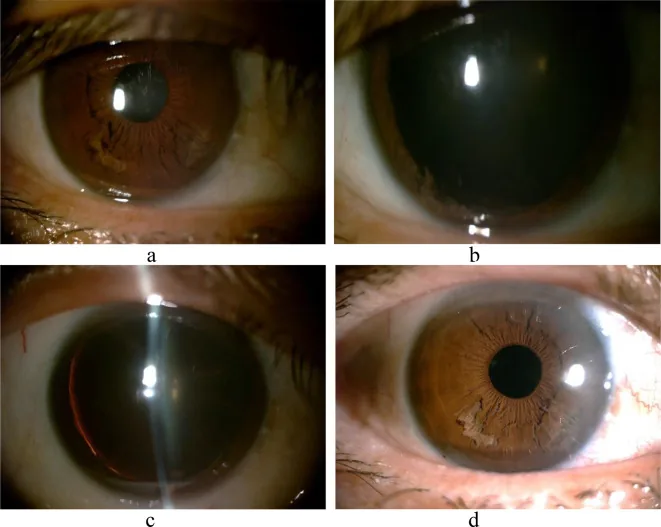
Subjective Symptoms
Section titled “Subjective Symptoms”Subjective symptoms due to iridoschisis itself are often scarce. Symptoms depend on the progression of complications (glaucoma, corneal endothelial damage).
- Often asymptomatic: Frequently discovered incidentally during slit-lamp examination.
- Headache/eye pain: Intermittent headache or eye pain may occur when glaucoma is present.
- Vision loss: Caused by visual field defects from associated glaucoma or progression of cataract.
- Blurred vision: Appears when corneal endothelial damage progresses and corneal edema occurs.
- During acute angle-closure attack: Severe eye pain, headache, nausea, and sudden vision loss. Requires emergency management.
- Floaters: Occasionally noticed when detached iris fibers float in the anterior chamber (rare).
Clinical Findings
Section titled “Clinical Findings”- Predominantly occurs in the inferior iris (inferonasal to inferotemporal quadrants), and in advanced cases, it may involve the entire circumference 1)6).
- On slit-lamp microscopy, it presents a unique appearance of “white shredded threads” or “fringe-like” fibers floating in the anterior chamber.
- The posterior iris leaf appears thinned on transillumination, but the pupillary sphincter is often preserved 1).
- The posterior pigment epithelium is usually intact 6).
- Free fibers may contact the corneal endothelium, causing mechanical irritation and corneal endothelial damage 3).
- Fiber deposition in the angle → risk of mechanical obstruction of the trabecular meshwork 2).
- Frequently accompanied by findings of shallow anterior chamber, short axial length, and hyperopia.
- Free fibers in the anterior chamber may move with changes in body position (standing or lying down) and can be observed during slit-lamp examination.
Iridoschisis itself rarely causes pain or vision loss. However, about two-thirds of cases are complicated by glaucoma, which may lead to symptoms such as headache, eye pain, and vision loss. Additionally, floating iris fibers can damage the corneal endothelium, causing blurred vision due to corneal edema. Regular eye examinations are important.
6. Examination
Section titled “6. Examination”The diagnosis of iridoschisis is primarily based on clinical examination using slit-lamp microscopy. No independent standard diagnostic criteria have been established, and confirmation of characteristic slit-lamp findings is essential for a definitive diagnosis.
Slit-lamp microscopy
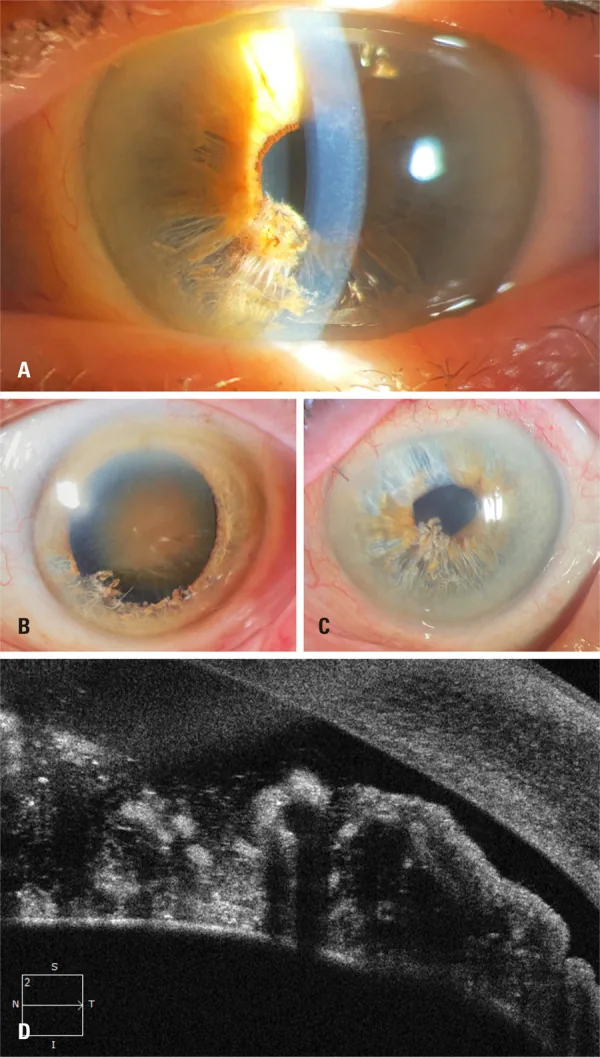
Section titled “Slit-lamp microscopy”In the inferior iris, ‘shredded wheat’-like atrophic fibers and floating fibers in the anterior chamber are observed 1)6). This is the first step in diagnosis. The extent of separation (number of quadrants) and the amount of fibers in the anterior chamber are evaluated. The presence of white thread-like fibers floating in the anterior chamber is a key finding for definitive diagnosis.
Gonioscopy
Section titled “Gonioscopy”Detailed evaluation of the presence of angle closure, extent of peripheral anterior synechiae (PAS), fiber deposition in the angle, and the condition of the trabecular meshwork. It is recommended in all cases.
Anterior segment OCT (AS-OCT)
Section titled “Anterior segment OCT (AS-OCT)”Detailed imaging of the bilayered separation of the iris stroma, floating fibers, and the condition of the posterior pigment epithelium 1)5)6). Findings include breaks in the anterior border layer, moth-eaten stromal separation, and shadows of free fibers in the anterior chamber. Angle assessment is possible even in cases where gonioscopy is difficult due to corneal edema 5).
The ITC (iridotrabecular contact) index is a quantitative measure of the extent of contact between the peripheral iris and trabecular meshwork. In a 76-year-old woman with bilateral iris separation, the ITC index improved from 23.6% to 4.7% after cataract surgery and became 0% after DSAEK 5).
Ultrasound Biomicroscopy (UBM)
Section titled “Ultrasound Biomicroscopy (UBM)”It can visualize separation of echo brightness within the iris, anterior displacement of the ciliary body, and dissociation of the zonules 1). It is useful for evaluating mechanisms of angle closure such as plateau iris and anterior rotation of the ciliary body.
Other Tests
Section titled “Other Tests”- Intraocular pressure measurement: Performed in all cases. Screening for glaucoma. Since diurnal variation can be large, measurement at multiple times of day is desirable.
- Specular microscopy: Quantitative evaluation of corneal endothelial cell density (ECD). Determines the degree and progression of endothelial damage due to free iris contact.
- Visual field testing (Humphrey 30-2, etc.): Regular visual field evaluation is essential in cases with glaucoma. Even in cases without glaucoma, initial measurement is recommended as a baseline.
- Axial length measurement (A-scan/IOLMaster): Confirms short axial length and hyperopia. Useful for quantitative assessment of angle closure predisposition.
7. Diagnosis and Differential Diagnosis
Section titled “7. Diagnosis and Differential Diagnosis”Differential Diagnosis
Section titled “Differential Diagnosis”| Disease | Age/Sex | Unilateral/Bilateral | Key Findings | Differentiating Points |
|---|---|---|---|---|
| Iridoschisis | 50s–80s, slightly more common in women | Bilateral | Separation and fraying of iris anterior layer fibers | Angle findings, posterior pigment epithelium preserved |
| ICE syndrome (progressive iris atrophy) | 30s–40s, more common in women | Unilateral | Corneal endothelial abnormality, iris atrophy, pupillary deviation | Atypical cells on specular microscopy |
| Axenfeld-Rieger syndrome | At birth | Bilateral | Iris atrophy, posterior embryotoxon | Congenital, angle abnormality |
| Exfoliation syndrome (PEX) | Elderly | Unilateral/bilateral | White deposits on anterior lens capsule and pupillary margin | No free iris fibers |
| Traumatic iris injury | All ages | Unilateral | Focal iris tears and pupillary distortion | History of trauma, asymmetry |
In differentiating from ICE syndrome, it is important that iridoschisis is more common in the elderly, often bilateral, and can be distinguished by gonioscopic findings. ICE syndrome is characterized by abnormal corneal endothelial cells, and specular microscopy is useful for differentiation.
Clinical diagnosis is made by slit-lamp microscopy, confirming atrophic fibers in the inferior iris and floating fibers in the anterior chamber. Anterior segment OCT can detail the two-layer separation of the iris stroma, and UBM can evaluate the ciliary body and zonules. Differentiation from ICE syndrome and Axenfeld-Rieger syndrome is important, based on age of onset, laterality, and pattern of iris changes.
8. Treatment
Section titled “8. Treatment”There is no curative treatment for the disease itself. Management of complications (glaucoma, corneal endothelial damage) is the mainstay of treatment. The treatment plan is determined based on the presence of glaucoma, intraocular pressure level, degree of visual field damage, and extent of corneal endothelial damage.
Pharmacotherapy for Cases with Glaucoma
Section titled “Pharmacotherapy for Cases with Glaucoma”Since approximately two-thirds of cases are complicated by glaucoma, baseline glaucoma evaluation (visual field test, OCT, gonioscopy, intraocular pressure measurement) is recommended for all patients. Many cases with elevated intraocular pressure respond to pharmacotherapy.
| Drug Class | Representative Drug | Dosage |
|---|---|---|
| Prostaglandin analogs (first-line) | Latanoprost 0.005% ophthalmic solution | Once daily at bedtime |
| Travoprost 0.004% ophthalmic solution | Once daily at bedtime | |
| Beta-blockers (second-line) | Timolol 0.5% ophthalmic solution | Twice daily |
| Carteolol 2% sustained-release ophthalmic solution | Once daily | |
| Carbonic anhydrase inhibitors | Dorzolamide 1% ophthalmic solution | 3 times daily |
| Brinzolamide 1% ophthalmic solution | 2 times daily | |
| Alpha-2 agonists | Brimonidine 0.1% ophthalmic solution | 2 times daily |
| Fixed combinations | Latanoprost/timolol fixed combination ophthalmic solution | Once daily |
| During acute attack | D-mannitol 250 mL (1.0–1.5 g/kg) intravenous infusion + acetazolamide 250–500 mg intravenous injection + pilocarpine 2% ophthalmic solution frequent instillation | — |
During an acute angle-closure attack, the highest priority is to rapidly lower intraocular pressure, and emergency treatment should be performed under inpatient management. After lowering intraocular pressure in the affected eye, laser iridotomy is performed.
Laser therapy
Section titled “Laser therapy”- Laser iridotomy (LPI): Performed to relieve angle closure. Since the iris tissue is fragile, care must be taken regarding the reaction to irradiation 2). After LPI, there is a risk of re-closure due to accumulation of free fibers, so regular postoperative angle evaluation is necessary.
- If LPI is technically difficult or insufficiently effective, surgical therapy (lens reconstruction) should be considered.
Cataract surgery
Section titled “Cataract surgery”Cataract surgery in eyes with iridoschisis is challenging for the following reasons 4).
- Poor pupil dilation: Due to iris atrophy and damage to the pupillary sphincter, mydriasis is often insufficient. Use of pupil devices (e.g., iris retractor) is recommended 1)4).
- Risk of aspirating free fibers: The phacoemulsification probe may aspirate free fibers. Techniques such as forming a barrier with ophthalmic viscosurgical devices (OVD) or pre-cutting fibers with a vitreous cutter have been reported 4).
- High risk of iris tear when using iris retractors.
- Use low perfusion and low aspiration settings to minimize intraocular pressure fluctuations.
- Manipulate while protecting the iris with ophthalmic viscosurgical devices.
In a systematic review (21 cases, 35 eyes), phacoemulsification was the most commonly performed surgery, and visual acuity improved significantly postoperatively. Complications included anterior chamber inflammation, corneal edema, and Descemet’s membrane folds 4).
Angle widening effect
Section titled “Angle widening effect”Cataract surgery significantly improves angle closure. In a case of a 76-year-old woman, cataract surgery reduced the ITC index from 23.6% to 4.7% 5). Early cataract surgery should be considered to prevent progression of corneal endothelial damage 5). Even in the absence of cataract, clear lens extraction may be considered to control angle closure.
Filtration surgery and goniosynechialysis
Section titled “Filtration surgery and goniosynechialysis”- Trabeculectomy with mitomycin C: Indicated when intraocular pressure is poorly controlled with medication or laser.
- Goniosynechialysis: Considered in cases with PAS formation.
- MIGS (Minimally Invasive Glaucoma Surgery): Whether it can be a treatment option for glaucoma-complicated cases requires further accumulation of cases.
Corneal Endothelial Management and Corneal Transplantation
Section titled “Corneal Endothelial Management and Corneal Transplantation”When corneal endothelial decompensation occurs, DSAEK (Descemet’s Stripping Automated Endothelial Keratoplasty) or DMEK is performed 5). There is a report that the ITC index improved to 0% after DSAEK 5).
Follow-up (Mild Cases without Glaucoma)
Section titled “Follow-up (Mild Cases without Glaucoma)”Even in mild cases without glaucoma, regular follow-up is necessary due to the risk of future glaucoma development.
- Intraocular pressure measurement: every 3–6 months
- Gonioscopy: every 6–12 months
- Visual field testing: every 6–12 months (more frequent in glaucoma-complicated cases)
- Corneal endothelial cell density measurement: approximately once a year
- Positional guidance: Some reports recommend elevating the head during sleep to reduce contact of free fibers with the corneal endothelium.
There is no surgery to cure iridoschisis itself. Management of coexisting glaucoma is the mainstay of treatment. Cataract surgery may be performed to resolve a shallow anterior chamber, but because the iris is fragile, more careful surgical manipulation than usual is required. If corneal endothelial damage is advanced, corneal endothelial transplantation may be considered. In any case, it is important to decide on a treatment plan after thorough consultation with a specialist.
9. Course and Prognosis
Section titled “9. Course and Prognosis”Mechanism of Disease Progression
Section titled “Mechanism of Disease Progression”- The adhesion between the anterior and posterior layers weakens, and separation progresses due to aqueous humor convection.
- Collagen fibers from the separated anterior layer become free in the aqueous humor.
- Free fibers reach and deposit in the angle, mechanically obstructing the trabecular meshwork, leading to secondary open-angle glaucoma with elevated intraocular pressure.
- Bulging of the iris root and accumulation of fibers cause peripheral anterior synechiae (PAS), progressing to secondary angle-closure glaucoma 2).
- A prevailing theory is that floating anterior layer stromal fibers bow forward and contact the trabecular meshwork, impeding aqueous outflow 6).
- A mechanism has also been proposed in which the posterior pigment epithelium hangs down onto the anterior lens capsule, inducing pupillary block.
Mechanism of Corneal Endothelial Damage
Section titled “Mechanism of Corneal Endothelial Damage”Floating iris fibers directly contact the corneal endothelium, causing mechanical irritation that leads to localized corneal edema and endothelial cell loss 1)3). Progression results in corneal endothelial decompensation (bullous keratopathy).
In three patients with atopic dermatitis, total protein in the aqueous humor was markedly elevated at 0.80, 0.95, and 1.40 mg/mL (normal 0.25–0.40 mg/mL), suggesting that protein leakage from the iris separation site contributes to early graft failure after corneal transplantation 3).
Prognosis and Outlook
Section titled “Prognosis and Outlook”- Due to the rarity of the disease, large-scale RCTs or cohort studies are almost nonexistent; the literature mainly consists of case reports and small case series.
- In cases with glaucoma, visual field prognosis depends on intraocular pressure control. Early detection and treatment are key to preserving visual function.
- In advanced cases of corneal endothelial damage, corneal endothelial transplantation is required, and the prognosis is extremely poor in patients with atopic dermatitis 3).
- The ITC index measured by anterior segment OCT is a new indicator that quantifies the contact area between the iris and trabecular meshwork, allowing objective tracking of changes before and after cataract surgery or DSAEK 5). It is expected to be useful as a criterion for determining the timing of surgery in the future.
- A systematic review has organized the risks and countermeasures during cataract surgery 4). It is important to select appropriate techniques according to the case, such as floating fiber management with microcautery, the OVD barrier method, and the use of pupillary devices.
- The role of lens reconstruction surgery for angle-closure glaucoma is being reevaluated, and accumulation of evidence is desired regarding the effectiveness of early surgical intervention to relieve shallow anterior chamber even in cases complicated by iridoschisis.
10. References
Section titled “10. References”-
Niu TT, Xin WJ. A case of iridoschisis with partial lens dislocation in both eyes. BMC ophthalmology. 2024;24(1):66. doi:10.1186/s12886-024-03330-y. PMID:38355462; PMCID:PMC10865630.
-
Pegu J, Jain K, Dubey S. Iridoschisis: Spectrum of Presentation. Middle East Afr J Ophthalmol. 2020;27(4):224-227. PMID: 33814819. PMCID: PMC7993048. doi:10.4103/meajo.MEAJO_120_19.
-
Kusano Y, Yamaguchi T, Shimazaki J, Dogru M. Iridoschisis in patients with atopic dermatitis leads to intractable bullous keratopathy. BMC ophthalmology. 2025;25(1):401. doi:10.1186/s12886-025-04245-y. PMID:40634911; PMCID:PMC12239428.
-
Amaral DC, Rodrigues MPM, Marques GN, Nascimento LM, Dinato RA, Oliveira VGA, et al. Iridoschisis associated with cataract: a systematic review of case reports. Einstein (Sao Paulo, Brazil). 2026;24:eRW1685. doi:10.31744/einstein_journal/2026RW1685. PMID:41563299; PMCID:PMC12711228.
-
Omoto T, Agata C, Akiyama R, Kitamoto K, Toyono T, Yoshida J, et al. Iridotrabecular and Iridocorneal Contact Changes after Cataract Surgery and Endothelial Keratoplasty in Bilateral Iridoschisis. Case reports in ophthalmology. 2021;12(1):198-203. doi:10.1159/000513793. PMID:33976682; PMCID:PMC8077475.
-
Bari A, Thulkar T, Tripathi M, Agarwal T. Iridoschisis: a rare ocular morbidity. BMJ case reports. 2023;16(5). doi:10.1136/bcr-2023-255297. PMID:37160378; PMCID:PMC10173979.