Findings of IOL dislocation

Scleral Fixation of IOL (Suturing and Intrascleral Fixation)
Key Points at a Glance
Section titled “Key Points at a Glance”1. What is suturing and intrascleral fixation?
Section titled “1. What is suturing and intrascleral fixation?”Suturing and intrascleral fixation are surgical techniques for refixing an intraocular lens (IOL) that has lost capsular support. They are indicated when capsular support is unavailable, such as in cases of posterior capsule rupture, zonular dialysis, IOL dislocation, IOL drop, or aphakia. In cases of zonular dialysis, completing the procedure with suturing is ideal for long-term prognosis, and a technique for suturing a 7.0 mm IOL through a small incision has been established.
Scleral suture fixation is a technique in which a non-absorbable suture is tied to the haptic of the IOL and fixed to the sclera through the ciliary sulcus. It can be performed using an ab interno (from inside the eye) or ab externo (from outside the eye) approach.
Intrascleral haptic fixation is a technique in which the haptic of the IOL is passed through a scleral tunnel created with a 30-gauge needle, without using any sutures or adhesives, and secured by a flange (bulbous enlargement) formed by cauterization. The double-needle technique reported by Yamane et al. in 2017 (Yamane method) has become a representative procedure. 1)
Note that this article focuses specifically on the techniques, indications, and selection of suturing and intrascleral fixation, unlike “Intraocular Lens Dislocation,” which covers the overall pathology and diagnosis of IOL dislocation, and “Secondary IOL Implantation,” which covers general surgical techniques for secondary IOL insertion.
Main Indications
Section titled “Main Indications”- IOL dislocation: IOL displacement or drop due to zonular dialysis
- Aphakic eye: When there is no capsular support due to complications or trauma during initial surgery
- Capsular insufficiency: Eyes with partially damaged lens capsule
- Posterior capsule rupture: When in-the-bag insertion is impossible
- IOL exchange: Replacement of existing IOL due to opacification or refractive error
| Indication status | Corresponding surgery |
|---|---|
| Mild IOL deviation (position correction only) | IOL repositioning |
| IOL dislocation / loss of capsular support | Sutured or intrascleral fixation |
| IOL drop (into vitreous cavity) | Vitrectomy + sutured or intrascleral fixation |
| Zinn zonule rupture + simultaneous PEA | Temporary CTR use → Suture fixation |
| Posterior capsule rupture (cannot be inserted in the bag) | Suturing technique (performed by experienced surgeon) |
Q
What is the difference between suturing and intrascleral fixation?
A
Sutured scleral fixation is a technique in which the haptics of an IOL are fixed to the sclera via the ciliary sulcus using non-absorbable sutures (e.g., 9-0 or 8-0 polypropylene). It requires the creation of a scleral flap and carries a risk of late dislocation due to long-term suture breakage. Intrascleral fixation (Yamane technique) uses no sutures; the haptics are inserted into a scleral tunnel created with a 30-gauge needle, and the tips are cauterized to form flanges for fixation. It is minimally invasive and eliminates the risk of suture breakage, but requires a learning curve and is unsuitable for patients with atopy and habitual eye rubbing. Network meta-analysis shows equivalent efficacy between the two techniques. 3)
2. Main symptoms and clinical findings
Section titled “2. Main symptoms and clinical findings”Subjective symptoms
Section titled “Subjective symptoms”The main subjective symptoms of IOL dislocation or subluxation are as follows.
- Decreased visual acuity and refractive changes: Refractive errors due to IOL decentration or tilt, or when the optic part moves out of the pupillary area.
- Monocular diplopia and glare: Caused by the IOL edge being exposed in the pupillary area
- Oscillopsia: The IOL moves with changes in body position, altering vision
- Visual field defect: Occurs when the optic portion moves out of the visual field due to IOL dislocation or drop
- Severe hyperopia: When the IOL falls into the vitreous cavity, high hyperopia similar to aphakia occurs
- Asthenopia: Associated with refractive error and aniseikonia
Clinical Findings
Section titled “Clinical Findings”Diagnosis can be easily made by dilating the pupil and checking the following four items.
- Position of the IOL optic and haptics
- Condition of the zonules of Zinn
- Condition of the lens capsule
- Presence or absence of IOL oscillation (tremor)
For dislocation or drop, exchange surgery is required, so always confirm in the supine position under an operating microscope. Even if the IOL appears to be in the pupillary area when assessed in the sitting position with a slit lamp, it often tilts or sinks posteriorly in the supine position. IOL dislocation into the anterior chamber carries risks of corneal endothelial damage and pupillary block glaucoma, and may require emergency management. The position of the haptic and its relationship with capsular contraction should be evaluated in detail with a slit lamp microscope.
Q
What symptoms occur when the IOL dislocates?
A
The most common symptom is decreased visual acuity. When the IOL is displaced, the optical part of the lens moves out of the pupil, causing refractive error. Additionally, monocular diplopia (exposure of the IOL edge in the pupillary area), glare, and oscillopsia with changes in body position may occur. If the IOL falls into the vitreous cavity, significant hyperopia occurs, similar to an aphakic eye. Dislocation into the anterior chamber can be an emergency with eye pain and elevated intraocular pressure.
3. Causes and Risk Factors
Section titled “3. Causes and Risk Factors”The causes of IOL dislocation vary by type. Decentration and tilt are often due to surgical technique issues such as extracapsular insertion or asymmetric placement. In-the-bag dislocation occurs when the IOL sinks posteriorly due to progression of zonular rupture, with pseudoexfoliation syndrome being the most common cause, accounting for about 40% of zonular deterioration. Out-of-the-bag dislocation often occurs after intraoperative capsular complications. IOL drop occurs when in-the-bag dislocation progresses to complete zonular rupture, or when the IOL completely separates from the capsule in out-of-the-bag dislocation.
The zonules pull the lens capsule equator in 360 degrees, serving a dual role of fixing the lens on the visual axis and maintaining capsule shape through uniform traction. Depending on the extent and degree of rupture, either fixation, shape maintenance, or both may be lost.
Ocular Risk Factors
Pseudoexfoliation syndrome (PXF): The most common cause. Pseudoexfoliative material accumulates on the zonules, progressively weakening the fibers. It accounts for about 40% of in-the-bag dislocations.
After vitreous surgery: Damage to the zonules of Zinn and loss of vitreous support due to peripheral vitrectomy. Often occurs 10–20 years postoperatively due to age-related changes.
High myopia: Weakening of the capsule and zonules of Zinn due to axial elongation, and reduced support from vitreous liquefaction.
Anterior capsule contraction (capsular phimosis): Centripetal contraction due to proliferation of lens epithelial cells and myofibroblastic metaplasia after CCC. This places excessive tension on the zonules of Zinn, contributing to late dislocation.
Systemic and external risk factors
Atopic dermatitis: Mechanical trauma to the zonules of Zinn from repeated eye rubbing. This condition is a contraindication for intrascleral fixation.
Marfan syndrome: A connective tissue disorder caused by mutations in the FBN1 gene. Lens dislocation occurs in approximately 60% of cases.
History of trauma (blunt trauma): Rupture of the zonules of Zinn due to deformation of the eyeball.
History of intraoperative capsular complications: Previous intraoperative posterior capsule rupture or anterior capsule tear increases the risk of late dislocation.
4. Diagnosis, Examination Methods, and Surgical Approach Selection
Section titled “4. Diagnosis, Examination Methods, and Surgical Approach Selection”Diagnostic Approach
Section titled “Diagnostic Approach”The basic diagnostic method is slit-lamp examination under mydriasis, but supine evaluation under an operating microscope is essential for confirming dislocation or subluxation. In many cases, the lens appears normally positioned in the pupillary area when the patient is seated, but posterior tilt or sinking becomes apparent in the supine position.
The following assessments are necessary for preoperative diagnosis.
- Dislocation or subluxation (differentiating the degree of IOL displacement)
- Intracapsular or extracapsular dislocation
- How to lift the IOL onto the iris
- Extent of vitrectomy to be performed
- Selection of instruments needed for extraction and fixation
Required examination items
Section titled “Required examination items”| Examination method | Main purpose |
|---|---|
| Slit-lamp microscopy (under mydriasis) | Evaluation of IOL position and stability, confirmation of haptic position |
| Surgical microscope (supine position) | Definitive diagnosis of dislocation or drop |
| B-mode ultrasound | Detection of intraocular lens in vitreous cavity, confirmation of posterior segment status |
| Anterior segment OCT / UBM | Evaluation of IOL behind iris, assessment of zonular status, detailed evaluation of haptics |
| Specular microscopy | Corneal endothelial cell density (preoperative evaluation) |
| Corneal curvature and anterior chamber depth measurement | IOL power calculation and surgical method determination |
| Fundus examination | Exclusion of retinal complications (e.g., detachment) |
Surgical method selection algorithm
Section titled “Surgical method selection algorithm”- Capsular support present → Prioritize ciliary sulcus fixation (3-piece IOL)
- No capsular support, weak Zinn zonules → Suture fixation or intrascleral fixation
- Atopy/eye rubbing habit present → Scleral suturing is appropriate. Intrascleral fixation is inappropriate.
- PVDF multipiece IOL → Scleral refixation of the existing IOL within the vitreous cavity is also an option
- Need for simultaneous glaucoma surgery → Select the surgical technique individually considering interference with conjunctival and scleral manipulation. There are case reports of simultaneous intrascleral fixation and trabeculectomy6)
- Poor iris/sclera condition or repeated dislocation → Consider exchange to ACIOL
Criteria for selecting surgical technique
Section titled “Criteria for selecting surgical technique”| Evaluation item | Sutured technique | Yamane technique |
|---|---|---|
| Learning curve | Established | Requires time to master |
| Estimated surgery time | 20–30 minutes | 15–20 minutes |
| Risk of suture breakage or loss | Yes | No |
| Risk of intraocular infection | Relatively high | Low |
| Long-term outcomes | Over 30 years of data | Data being accumulated |
Q
What tests determine whether surgery is necessary?
A
First, evaluate the IOL position, movement, and zonular status using a slit-lamp microscope under mydriasis. If dislocation or subluxation is suspected, always confirm the patient in the supine position under an operating microscope. If intraocular lens drop into the vitreous cavity is suspected, add B-mode ultrasound. Anterior segment OCT or UBM is useful for detailed evaluation behind the iris, and preoperative assessment of corneal endothelial cell density by specular microscopy influences the choice of surgical technique.
5. Standard Treatment
Section titled “5. Standard Treatment”5-1. Overview of Treatment Strategy
Section titled “5-1. Overview of Treatment Strategy”Management of a dislocated or dropped IOL varies greatly depending on the degree and condition of the displacement.
- Mild displacement (pupillary capture, capsular capture, loop dislocation into the anterior chamber, early postoperative asymmetric fixation, etc.) → IOL repositioning. Position can be corrected with a hook or spatula through a side port.
- Dislocation/Drop → In principle, after IOL removal, insert a new suture-fixated IOL or an IOL suitable for intrascleral fixation.
- Dropped IOL → After total vitrectomy, retrieve and remove using vitreous forceps. Suture fixation or intrascleral fixation after removal is as usual.
- PVDF material multipiece IOL → Because the haptics are resistant to breakage, scleral refixation can be performed directly within the vitreous cavity.
5-2. Surgical technique for removal of dislocated IOL
Section titled “5-2. Surgical technique for removal of dislocated IOL”First, lift the IOL above the pupil, then create an incision of appropriate width and remove it.
- Foldable IOL: Can be cut in the anterior chamber and removed through a small incision of 3–4 mm width.
- PMMA IOL: An incision of approximately 6.5 mm is required to match the optic size.
- Dislocated IOL: Liquid perfluorocarbon (LPFC) can be used to float the IOL up to the iris plane.
- Corneal endothelial protection: Fill the eye with ophthalmic viscosurgical device (OVD) during IOL manipulation and removal.
5-3. Suture fixation (transscleral suture fixation)
Section titled “5-3. Suture fixation (transscleral suture fixation)”Principle: Using an ab interno or ab externo approach, a non-absorbable suture is tied to the IOL haptic and fixed to the sclera through the ciliary sulcus. Two-point fixation is standard.
Specific technique using the cow-hitch method:
- Create a scleral flap at the limbus at the 12 o’clock position
- Puncture the ciliary sulcus with a long needle attached to 9-0 polypropylene suture
- Puncture from the 6 o’clock direction with a 30-gauge pick-up needle
- Connect the long needle and the pick-up needle to pass the suture
- Tie the suture to the IOL haptic using a cow-hitch knot
- Insert the haptic into the predetermined ciliary sulcus position
- Sutured and fixed to the sclera under a scleral flap
Haptic externalization method: The IOL haptic is inserted into a 25-gauge needle and guided out of the eye through a side port. After creating a cow-hitch knot, the tip is enlarged by electric cautery and pulled into a scleral tunnel.
Suture selection:
- 9-0 or 8-0 polypropylene (Prolene) suture is standard. 10-0 polypropylene carries a risk of suture breakage at an average of 4–6.5 years 4)
- CV-8 Gore-Tex suture has high tensile strength and is expected to reduce long-term breakage risk
Situations to consider capsule preservation: In cases with zonular weakness but remaining capsular support, a capsule-preserving technique may be considered. Although it may reduce vitreous cavity invasion, evaluation of posterior capsule rupture and long-term stability is necessary, and it is determined on a case-by-case basis as a standard procedure.
Main complications:
- IOL redislocation (late dislocation due to suture breakage)
- IOL tilt and decentration
- Intraocular hemorrhage
- Retinal detachment
- Exposure, erosion, or breakage of suture knot 5)
- Glaucoma
- Pupillary capture after suturing (prone to recurrence because the optic is not covered by the capsule immediately behind the iris)
5-4. Intrascleral fixation (Yamane technique / flanged intrascleral fixation)
Section titled “5-4. Intrascleral fixation (Yamane technique / flanged intrascleral fixation)”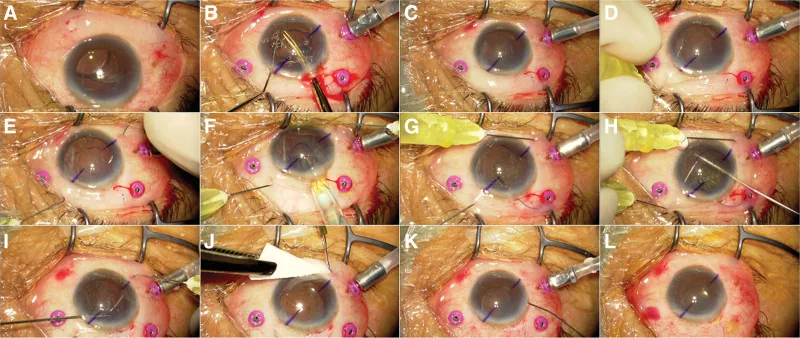
Nakagawa S, Ishii K. Secondary intrascleral intraocular lens (IOL) fixation with capsule preservation for IOL dislocation following mature cataract surgery with incomplete capsulorhexis: A case report. Medicine (Baltimore). 2025;104(25):e43030. doi:10.1097/MD.0000000000043030. PMID:40550021. PMCID:PMC12187320. Figure 1. License: CC BY 4.
Intraoperative course shown in 12 panels from preoperative IOL inferonasal decentration (A) to 30-gauge needle insertion (D/E), 3-piece IOL injector insertion (F/G), and flange formation and scleral fixation using the double-needle technique (H–J). Corresponds to the sequential steps of the Yamane double-needle technique described in section “5-4. Intrascleral fixation (Yamane technique).”
Principle: A scleral tunnel is created with a 30-gauge thin-wall needle, the haptic of a 3-piece IOL is inserted into the needle lumen and externalized through the sclera, and the tip of the haptic is cauterized to form a flange (spherical bulge). The IOL is fixed by the flange being locked within the scleral tunnel. No sutures or adhesives are used. 1)
Specific technique of the Yamane double-needle method:
- Puncture at two points 180 degrees apart, 2 mm from the corneal limbus, using a 30-gauge thin-wall needle.
- Insert each haptic of the IOL into the lumen of each needle.
- Pull the haptic out through the sclera together with the needle.
- Form a flange (bulbous enlargement) at the tip of the haptic using low-temperature electrocautery.
- Pull the flange back into the scleral tunnel and embed it for fixation.
Recommended IOL: 3-piece IOLs with PVDF (polyvinylidene fluoride) haptics offer excellent durability. CT Lucia 602P, NX-70, etc. are used.
Advantages:
- No need for scleral flap creation, making it minimally invasive
- No risk of late dislocation due to suture breakage
- Early visual recovery can be expected
- When combined with glaucoma surgery, the surgical technique should be individually considered to avoid interference with conjunctival and scleral manipulation6)
Main complications:
- Elevated intraocular pressure
- IOL tilt and decentration10)
- Optic capture
- Vitreous hemorrhage
- Cystoid macular edema (CME)
- Conjunctival penetration/erosion of the haptic
- Endophthalmitis2)
Important note: Intrascleral fixation is not suitable for patients with atopic dermatitis who have a habit of eye rubbing; sutured fixation is chosen instead.
5-5. Surgical technique comparison table
Section titled “5-5. Surgical technique comparison table”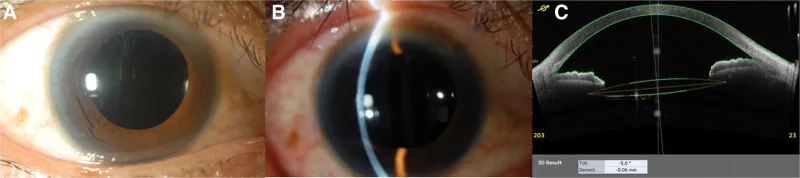
Nakagawa S, Ishii K. Secondary intrascleral intraocular lens (IOL) fixation with capsule preservation for IOL dislocation following mature cataract surgery with incomplete capsulorhexis: A case report. Medicine (Baltimore). 2025;104(25):e43030. doi:10.1097/MD.0000000000043030. PMID:40550021. PMCID:PMC12187320. Figure 2. License: CC BY 4.
Anterior segment photographs (A: normal illumination, B: slit-lamp optical section) and anterior segment OCT (C) three months after intrascleral fixation. IOL tilt 5.0 degrees and decentration 0.06 mm indicate good centration. Corresponds to refractive predictability and tilt evaluation after intrascleral fixation discussed in section “5-5. Surgical technique comparison table.”
| Item | Suturing technique (transscleral suture fixation) | Intrascleral fixation (Yamane technique) |
|---|---|---|
| Fixation principle | Fix haptic to sclera with suture | Embed haptic flange in scleral tunnel |
| Suture | Required (e.g., 9-0/8-0 polypropylene) | Not required |
| Scleral flap | Required | Not required |
| Suitable IOL | Various types compatible (including PMMA) | 3-piece IOL (PVDF haptic recommended) |
| Late rupture risk | Yes (rupture reported at average 4–6.5 years4)) | None |
| Haptic erosion risk | Low | Present |
| Procedure complexity | Moderately high | High (requires training) |
| Suitability for oculodigital habit | Suitable | Unsuitable |
| Combined glaucoma surgery | Case-by-case | Case-by-case6) |
| Refractive predictability (within ±0.5 D) | Approximately 50% | Approximately 50% |
A network meta-analysis of the three methods (iris fixation, transscleral suturing, and intrascleral fixation) confirmed that their efficacy is equivalent. 3) The AAO PPP also recommends the three methods in parallel (I+, Good, Strong). 2)
5-6. Key points for suturing in cases of Zinn zonule rupture
Section titled “5-6. Key points for suturing in cases of Zinn zonule rupture”If Zinn zonule rupture is detected intraoperatively, manage it with the following steps.
- Temporarily use a CTR (capsular tension ring) to perform PEA (phacoemulsification)
- After PEA, remove the CTR and capsular bag through a small incision
- Perform anterior vitrectomy before suturing
- All steps can be performed through a 3.0 mm sclerocorneal incision and two 2.0 mm corneal ports
Note that the capsular tension ring with suture fixation (sutured CTR) has been found to have uncertain long-term outcomes and is generally not recommended.
Suturing technique (transscleral suture fixation)
Indications: General loss of capsular support, zonular dialysis, history of eye rubbing in atopic patients, various IOLs (including PMMA).
Suture: 9-0 or 8-0 polypropylene. Tie to the haptic using a cow-hitch technique and suture under a scleral flap via the ciliary sulcus.
Advantages: Compatible with many IOL designs. Reliable fixation. Suitable for patients with eye rubbing habits.
Disadvantages: Risk of suture breakage (late dislocation). Requires creation of a scleral flap. Difficult to perform simultaneously with glaucoma surgery.
Intrascleral Fixation (Yamane Technique)
Indications: Loss of capsular support, concurrent glaucoma surgery, 3-piece IOL (PVDF haptic), cases desiring minimally invasive approach.
Fixation method: Scleral tunnel with 30G thin-wall needle + haptic flange fixation. No sutures, adhesive, or scleral flap required.
Advantages: Minimally invasive. No risk of suture breakage. Favorable for simultaneous glaucoma surgery. Early visual recovery.
Disadvantages: Requires skill acquisition. Unsuitable for patients with eye rubbing habit. Risk of haptic erosion.
Q
Which is better: suture fixation or intrascleral fixation?
A
Network meta-analysis shows that iris fixation, transscleral suture fixation, and intrascleral fixation all have equivalent efficacy. 3) The choice of procedure depends on patient background, surgeon’s proficiency, and the IOL used. Suture fixation is safer for patients with atopy and eye rubbing habit. Intrascleral fixation is advantageous when simultaneous glaucoma surgery is needed. For any procedure, refractive predictability is inferior to in-the-bag fixation (within ±0.5 D: about 72%) at about 50%, so postoperative refractive error should be anticipated.
Q
What should I be careful about in daily life after surgery?
A
After suturing or intrascleral fixation, the IOL is not covered by the capsule just behind the iris, making pupillary capture more likely to recur. If vision changes, seek medical attention promptly. Suturing carries a risk of late dislocation due to long-term suture degradation or breakage, so regular ophthalmology follow-up is necessary. Avoid rubbing the eyes vigorously or applying external force. If the patient has a habit of hitting the eyes due to atopy, collaboration with a dermatologist or psychosomatic specialist may be needed.
6. Prognosis and Long-term Course
Section titled “6. Prognosis and Long-term Course”Visual Prognosis
Section titled “Visual Prognosis”Both sutured and intrascleral fixation achieve best-corrected visual acuity of 0.6 or better in approximately 60–80% of cases at 3 months postoperatively. The rate of achieving refractive prediction within ±0.5 D is about 50%, which is inferior to in-the-bag fixation (approximately 72%), and this should be explained to patients preoperatively.
Frequency of Major Complications
Section titled “Frequency of Major Complications”| Complications | Suture method | Yamane method | Special notes |
|---|---|---|---|
| Suture breakage or loosening | 5–15% | 0% | Main late complications of suture fixation |
| Endophthalmitis | 0.1–0.2% | <0.1% | Tends to be lower with Yamane technique |
| IOL dislocation/decentration | 5–10% | 2–5% | Visual axis deviation |
| IOL tilt/decentration | Present | Present10) | Cause of refractive error |
| Refractive error | Variable | Variable | IOL power calculation is important |
| Shallowing of anterior chamber | Rare | Rare | Severe cases are rare |
| Pupillary capture | Present | Present | Because the optic is located just behind the iris |
Key points for long-term follow-up
Section titled “Key points for long-term follow-up”- In scleral fixation, long-term regular follow-up is necessary to prepare for late IOL dislocation due to suture degradation.
- In the Yamane method, check for conjunctival penetration/erosion of the haptic and temporal changes in IOL tilt/decentration.
- Cystoid macular edema (CME) may develop several months after surgery; perform OCT evaluation when visual acuity decreases.
7. Pathophysiology and Detailed Mechanism
Section titled “7. Pathophysiology and Detailed Mechanism”Function of Zinn’s Zonules and Mechanism of IOL Decentration
Section titled “Function of Zinn’s Zonules and Mechanism of IOL Decentration”Zinn’s zonules pull the lens capsule equator in 360 degrees, serving a dual role of fixing the position toward the visual axis center and maintaining capsule shape through uniform traction. Depending on the degree and extent of rupture, either or both of position fixation and shape maintenance are lost.
The mechanisms of IOL decentration by cause are as follows:
- Eccentricity/tilt: Due to surgical errors such as extracapsular insertion, asymmetric insertion, or improper placement during suturing or scleral fixation
- Intracapsular dislocation: A condition where the IOL sinks posteriorly due to progression of zonular rupture. Exfoliation syndrome accounts for about 40%, followed by post-vitrectomy, high myopia, and atopic eye rubbing habit
- Extracapsular dislocation: Often occurs after intraoperative capsular complications
- IOL drop: When intracapsular dislocation progresses to complete zonular rupture, or when the IOL completely separates from the capsule in extracapsular dislocation
Zonular weakness in exfoliation syndrome
Section titled “Zonular weakness in exfoliation syndrome”In exfoliation syndrome, exfoliation material deposits on the iris, lens surface, angle, and ciliary body surface. This material accumulates directly on zonular fibers, and fiber weakening progresses with age. Poor mydriasis during cataract surgery is also common, increasing surgical difficulty.
Late dislocation due to anterior capsule contraction
Section titled “Late dislocation due to anterior capsule contraction”After continuous curvilinear capsulorhexis (CCC), lens epithelial cells at the capsulorhexis margin proliferate and transdifferentiate into myofibroblasts. When the centripetal contractile force generated by these cells exceeds the centrifugal traction of the zonules, anterior capsule contraction (capsular phimosis) progresses. The increased weight of the IOL and capsule due to posterior capsule opacification further increases stress on the zonules.
Refractive characteristics of sutured and scleral-fixated IOLs
Section titled “Refractive characteristics of sutured and scleral-fixated IOLs”IOLs after suturing or scleral fixation tend to be positioned more anteriorly compared to in-the-bag fixation, resulting in reduced refractive predictability. The rate of achieving within ±0.5 D is approximately 72% for in-the-bag fixation, but only about 50% for scleral fixation. 10) This is an important point that should be thoroughly explained to patients preoperatively.
Indications for suturing when the posterior capsule is ruptured
Section titled “Indications for suturing when the posterior capsule is ruptured”When intraoperative posterior capsule rupture prevents in-the-bag insertion, IOL suturing is indicated. The procedure is complex and has a high complication rate; it is recommended to be performed by an experienced surgeon.
8. Latest Research and Future Prospects
Section titled “8. Latest Research and Future Prospects”Application of Light Adjustable Lens (LAL) to Scleral Fixation
Section titled “Application of Light Adjustable Lens (LAL) to Scleral Fixation”The biggest challenge after suturing or intrascleral fixation is poor refractive predictability (achievement rate within ±0.5 D: approximately 50%10)). The Light Adjustable Lens (LAL) is an IOL whose power can be adjusted postoperatively by UV irradiation.
Ma et al. (2023) performed trocar-based ISHF (intrascleral haptic fixation) of an LAL in a 53-year-old woman with spontaneous bilateral lens subluxation.7) Postoperatively, power adjustment was performed targeting micro-monovision, achieving uncorrected visual acuity of 20/20 in both eyes. The application of LAL to scleral fixation is noted as an approach that may overcome the biggest weakness of scleral fixation: refractive prediction error.
Simplification of the procedure using the trocar-based modification
Section titled “Simplification of the procedure using the trocar-based modification”Bever et al. (2021) reported a modification in which the IOL is intentionally dropped onto the retina and then the haptic tip is directly grasped with a 27-gauge forceps and pulled out through the sclera. 8) This technique eliminates the need for manipulation at the iris plane and is safe and efficient for surgeons skilled in vitreoretinal surgery. Stable IOL positioning and good centration were achieved in all 4 cases.
Refixation of multifocal IOL using the cable tie method
Section titled “Refixation of multifocal IOL using the cable tie method”Eom et al. (2022) reported four-point flanged intrascleral fixation for subluxated multifocal IOLs with C-loop and double C-loop haptics using the cable tie method with 6-0 polypropylene. 9) By forming a loop of suture like a cable tie, secure fixation at the optic-haptic junction was achieved, and good IOL centration and distance and near visual acuity were obtained in both cases.
Four-point flanged intrascleral fixation
Section titled “Four-point flanged intrascleral fixation”Canabrava (2020) reported a four-point flanged intrascleral fixation method that uses no scleral flaps, sutures, or glue. 11) Four-point fixation of the haptics is expected to reduce tilt.
9. References
Section titled “9. References”- Yamane S, Sato S, Maruyama-Inoue M, Kadonosono K. Flanged intrascleral intraocular lens fixation with double-needle technique. Ophthalmology. 2017;124:1136-1142. doi:10.1016/j.ophtha.2017.03.036.
- Miller KM, Oetting TA, Tweeten JP, Carter K, Lee BS, Lin S, et al. Cataract in the Adult Eye Preferred Practice Pattern. Ophthalmology. 2022;129(1):P1-P126. doi:10.1016/j.ophtha.2021.10.006. PMID:34780842.
- Li X, Ni S, Li S, Zheng Q, Wu J, Liang G, et al. Comparison of Three Intraocular Lens Implantation Procedures for Aphakic Eyes With Insufficient Capsular Support: A Network Meta-analysis. American journal of ophthalmology. 2018;192:10-19. doi:10.1016/j.ajo.2018.04.023. PMID:29750951.
- John T, Tighe S, Hashem O, Sheha H. New use of 8-0 polypropylene suture for four-point scleral fixation of secondary intraocular lenses. Journal of cataract and refractive surgery. 2018;44(12):1421-1425. doi:10.1016/j.jcrs.2018.08.008. PMID:30314754.
- Yamane S, Ito A. Flanged fixation: Yamane technique and its application. Current opinion in ophthalmology. 2021;32(1):19-24. doi:10.1097/ICU.0000000000000720. PMID:33196545.
- Mano Y, Mizobuchi K, Watanabe T, Watanabe A, Nakano T. Minimally invasive surgery for intraocular lens removal and intrascleral intraocular lens fixation with trabeculectomy in a patient with dislocated intraocular lens and elevated intraocular pressure. Case Rep Ophthalmol. 2021;12:538-542. PMID: 34248588. PMCID: PMC8255743. doi:10.1159/000511593.
- Chu Jian Ma, Craig C. Schallhorn, Jay M. Stewart, Julie M. Schallhorn. Modified intrascleral haptic fixation of the light adjustable lens in a case of spontaneous adult-onset bilateral lens subluxation. American Journal of Ophthalmology Case Reports. 2023;31:101864. doi:10.1016/j.ajoc.2023.101864.
- Bever GJ, Liu Y, Stewart JM. Modified technique for trocar-based sutureless scleral fixation of intraocular lenses: A new approach to haptic externalization. American journal of ophthalmology case reports. 2021;23:101145. doi:10.1016/j.ajoc.2021.101145. PMID:34195478; PMCID:PMC8233194.
- Eom Y, Lee YJ, Park SY, Choi Y, Kim JW, Kim SJ, et al. Cable tie technique for securing scleral fixation suture to intraocular lens. American journal of ophthalmology case reports. 2022;27:101646. doi:10.1016/j.ajoc.2022.101646. PMID:35813586; PMCID:PMC9263869.
- Kumar DA, Agarwal A, Agarwal A, Chandrasekar R, Priyanka V. Long-term assessment of tilt of glued intraocular lenses: an optical coherence tomography analysis 5 years after surgery. Ophthalmology. 2015;122(1):48-55. doi:10.1016/j.ophtha.2014.07.032. PMID:25200402.
- Canabrava S, Canêdo Domingos Lima AC, Ribeiro G. Four-Flanged Intrascleral Intraocular Lens Fixation Technique: No Flaps, No Knots, No Glue. Cornea. 2020;39(4):527-528. doi:10.1097/ICO.0000000000002185. PMID:31658168.