Pseudoexfoliation syndrome (XFS, PEX) is a disease in which fibrous abnormal material (pseudoexfoliation material) accumulates in various parts of the eye, including the lens, iris, ciliary body, and trabecular meshwork. It was first described by Linberg in 1917 1).
The term “pseudoexfoliation” is used to distinguish it from true exfoliation of the lens capsule (glassblower’s exfoliation) that occurs in workers exposed to high temperatures. Although it appears to be a local eye disease, exfoliation material has also been found in systemic tissues such as skin, heart, lung, liver, and blood vessel walls, and it is understood as a systemic disease 2).
The global prevalence is estimated at 10–20% in people aged about 60 years and older, but it is particularly high in Scandinavia and the Middle East, and relatively low in East Asia 2). In Japan, pseudoexfoliation syndrome is found in about 4% of people aged 70 years and older, and glaucoma coexists in 20–40% of eyes with PEX.
Population-based data indicate that about 15–26% of XFS eyes develop pseudoexfoliation glaucoma within 5 years 4). Pseudoexfoliation glaucoma is the most common identifiable cause of open-angle glaucoma worldwide 2).
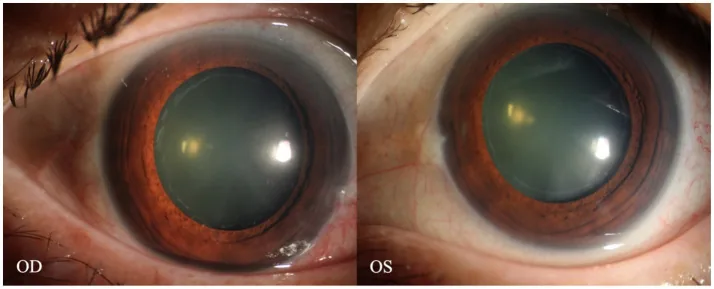
Lin B, et al. “Spider Web”-like zonular deposits in pseudoexfoliation syndrome: endoscopic insights-a case report. Front Med (Lausanne). 2025. Figure 3. PMCID: PMC12521236. License: CC BY.
Anterior segment photographs of both eyes after pupil dilation show ring-shaped gray-white deposits around the anterior lens capsule. This demonstrates pseudoexfoliation material on the anterior capsule characteristic of pseudoexfoliation syndrome, suitable for explaining clinical findings.
The following characteristic findings are observed on slit-lamp examination.
Findings of the Anterior Lens Capsule
Central disc: Accumulation of white granular material in the center of the anterior capsule.
Intermediate clear zone: A clear ring-shaped area where material has been removed by friction with the iris at the pupillary margin.
Peripheral band: A deposit zone of granular material outside the intermediate clear zone. Present in all cases, sometimes only visible after pupil dilation.
The concentric ring pattern of the above three zones is a typical finding. Best observed after pupil dilation.
Other Ocular Findings
Pseudoexfoliative material on the pupillary margin: White material deposits easily seen during miosis.
Poor pupillary dilation (moth-eaten pupil): Iris rigidity and pigment loss at the pupillary margin due to exfoliative material deposition on the iris sphincter4).
Zonular weakness: Observable as phacodonesis (lens tremulousness).
Sampaolesi line: Wavy pigmentation extending beyond the Schwalbe line. Accompanied by heavy pigmentation in the inferior trabecular meshwork.
Elevated intraocular pressure and increased diurnal variation: IOP levels are higher than in POAG, and diurnal variation is also greater4).
QIs pseudoexfoliation syndrome bilateral?
A
Initially, it is often found as a unilateral condition. However, over the long term, many patients develop it in the contralateral eye, and the rate of eventual bilaterality is high4). Regular observation of the contralateral eye when detected unilaterally is important.
XFS is an age-related disease, with prevalence increasing sharply after age 60. It is multifactorial, but genetic factors are most important.
LOXL1 gene polymorphism: SNPs (rs1048661, rs3825942) in the gene encoding lysyl oxidase-like 1 (LOXL1) are strongly associated with XFS3). Identified by genome-wide association studies (GWAS). In Japan, about half of the population carries high-risk polymorphisms.
Aging: The greatest environmental risk factor. Onset before age 60 is rare.
Geographic and ethnic background: Prevalence is high in Scandinavia, the Middle East, and the Mediterranean region, and relatively low in Japanese and Chinese populations. In a 21-year follow-up study in northern Sweden, the prevalence of pseudoexfoliation syndrome was high, and progression to PXFG was consistently observed2).
Ultraviolet exposure: Increased prevalence has been reported among farmers and outdoor workers2).
Association with systemic diseases: Associations with cardiovascular disease, stroke, inguinal hernia, and female pelvic organ prolapse have been suggested4).
The central mechanism of pseudoexfoliation material production is abnormal extracellular matrix metabolism and accumulation of elastic fibers. The material contains fibrillin, vitronectin, laminin, and others2). The exfoliative material deposits on the zonules of Zinn, promoting degradation by matrix metalloproteinases (MMPs) and leading to weakening of the supporting structure8).
The diagnosis of XFS is primarily clinical, based on slit-lamp microscopy. It is important to examine both under miosis and mydriasis: under miosis, evaluate white exfoliative material at the pupillary margin; under mydriasis, assess the three-zone pattern on the lens surface and the condition of the zonules of Zinn.
Observation of the anterior lens capsule after mydriasis is fundamental. Confirm the three-zone pattern: central disc, intermediate clear zone, and peripheral granular band. The peripheral band is present in all cases and may only be visible after mydriasis. Also check for material deposition on the pupillary margin, iris, and lens equator 2).
Sampaolesi’s line (wavy pigmentation extending beyond Schwalbe’s line) is characteristic of XFS 4). Confirm an open angle and assess heavy pigmentation of the trabecular meshwork.
Multiple intraocular pressure measurements at different times of day are recommended. XFS tends to have large diurnal fluctuations, which may be missed with a single measurement 4).
Performed when pseudoexfoliation glaucoma is suspected. Evaluates thinning of the retinal nerve fiber layer (RNFL). Regular examinations according to the 5th edition of the Glaucoma Practice Guidelines are conducted 6).
As a preoperative evaluation, check for the presence and degree of phacodonesis. An anterior chamber depth of less than 2.5 mm suggests zonular weakness and increases the risk of complications by approximately 5 times 5). Asymmetry of anterior chamber depth and the presence of lens displacement are also important. Corneal endothelial cell density evaluation by specular microscopy is also performed preoperatively 5).
QWhat is the difference between XFS and true lens capsule exfoliation (true exfoliation)?
A
True exfoliation is a lamellar peeling of the anterior lens capsule that occurs in high-temperature workers and glassblowers, caused by infrared exposure. It is a different disease from pseudoexfoliation syndrome (XFS). XFS involves deposition of cell-derived fibrous material, with a different pathology. In recent years, the number of glassblowers has decreased, and cases of true exfoliation are now rarely seen.
Pseudoexfoliation glaucoma is the most common cause of secondary open-angle glaucoma, and its progression is about three times faster than POAG2)4). Intraocular pressure fluctuations are large, and aggressive intraocular pressure reduction is recommended (evidence level 1B) 6). Considering that approximately 15–26% of XFS eyes develop pseudoexfoliation glaucoma within 5 years, regular follow-up is important 4).
Medical treatment: Following POAG guidelines, set a target intraocular pressure and aim to lower it. Prostaglandin (PG) agents are first-line. Depending on the situation, combine with beta-blocker eye drops, carbonic anhydrase inhibitor (CAI) eye drops, or oral medication 6).
Reports indicate that pseudoexfoliation glaucoma may achieve greater intraocular pressure reduction than POAG (evidence level 1B)6).
It is relatively effective, but long-term effects are not very promising. It is positioned as a bridge to surgery or as an option when surgery is not possible4).
Laser therapy and medication have comparable efficacy, but both tend to diminish in effect after a few years.
Surgical treatment6):
Consider early surgery in cases where visual field damage progresses and intraocular pressure reduction is insufficient, or when intraocular pressure fluctuations are large.
Both filtering surgery (trabeculectomy) and outflow pathway reconstruction (trabeculotomy) are effective.
In trabeculotomy, sufficient intraocular pressure reduction may not be achieved in cases with very high preoperative intraocular pressure.
In cases with extremely high intraocular pressure or severe visual field damage, it is safer to choose trabeculectomy.
Patients with XFS require special management during cataract surgery. Poor mydriasis and zonular weakness coexist, and the risk of intraoperative complications is reported to be approximately 2.68 times higher 5). Risk stratification based on preoperative evaluation is the most important step 5).
Risk item
Situation in XFS patients
Zonular dialysis
Up to 2.0% in low-risk cases, up to 9.0% in high-risk cases 5)
Capsular rupture / vitreous loss
Significantly higher risk in XFS eyes 5)
Poor pupil dilation
Even with maximal dilation, pupil diameter often remains less than 6 mm5)
Reduced long-term stability of in-the-bag fixation. Late dislocation of the IOL-capsule complex may occur
Anterior chamber depth less than 2.5 mm suggests zonular weakness and increases complication risk approximately 5-fold5). Evaluation of corneal endothelial cell density by specular microscopy is also useful for assessing the risk of postoperative corneal endothelial failure.
Ensuring pupil dilation:
Mechanical dilation with ophthalmic viscosurgical device (OVD): Use a high-viscosity cohesive OVD to secure a minimum pupil diameter of 4–5 mm 5).
Pupil stretching: A technique to physically stretch the pupillary margin to achieve mydriasis.
Pupil expansion devices and iris hooks: Maintain intraoperative mydriasis.
Anterior capsulotomy and nucleus management:
Anterior capsulotomy (CCC): Create a large continuous curvilinear capsulorhexis of 5.5–6.0 mm 5). A large CCC facilitates nucleus removal and reduces the risk of postoperative capsular contraction. Trypan blue staining is useful in cases of lens intumescence.
Minimization of ultrasound time: In hard brown cataracts, the amount of ultrasound energy used increases, so attention should be paid to the risk of posterior capsule rupture and corneal endothelial damage.
Support of the zonules and lens capsule:
Capsular tension ring (CTR): Inserted into the lens capsule before intraocular lens implantation to maintain the circular shape of the capsule and equalize tension on the zonules. It is also useful for preventing postoperative capsular contraction and intraocular lens decentration.
Iris hook-type capsule expander: Supports both the pupil and the lens capsule simultaneously.
Preparation for intravitreal triamcinolone injection: Prepare in advance for management of vitreous prolapse.
Angle irrigation: At the end of surgery, irrigate the anterior chamber angle to remove pseudoexfoliative material and OVD. This improves aqueous outflow through the trabecular meshwork and prevents postoperative intraocular pressure elevation.
Large-scale studies have reported that after adjusting for age and nuclear opacity, the best-corrected visual acuity at one year postoperatively was comparable between the PXF group and the control group (P=0.09), and the complication rate at one year was also not significantly different (2.7% in the PXF group vs. 2.5% in the control group)5). The mean corneal endothelial cell loss rate was 14.7% in the PXF group vs. 12.7% in the control group (P=0.066). This indicates that with appropriate preoperative evaluation and risk management, cataract surgery in PXF eyes can achieve good outcomes5).
QHow is cataract surgery for pseudoexfoliation syndrome different from standard cataract surgery?
A
There are three main differences: ① Poor mydriasis: Deposition of exfoliative material on the iris makes pupil dilation difficult, requiring assistance with OVD, pupil expansion rings, etc. ② Zonular weakness: Use of a capsular tension ring (CTR) enhances intraoperative safety. ③ Postoperative risk management: There is a risk of late dislocation of the IOL-capsule complex, necessitating long-term follow-up5). The risk of complications is approximately 2.68 times higher, but with appropriate management, good visual outcomes can be achieved5).
Pseudoexfoliative material is a complex composed of degenerated elastic fiber microfibrils and extracellular matrix components. Under electron microscopy, it shows a characteristic structure of fine fibrils 50–60 nm in diameter arranged in bundles and radially 2).
There are multiple sites of production of pseudoexfoliative material. Lens epithelial cells, iris pigment epithelium and non-pigment epithelium, and ciliary non-pigment epithelium have been identified as main sources. Production has also been confirmed in vascular endothelial cells and fibroblasts outside the eye, supporting that XFS is a systemic disease 2).
Role of LOXL1: LOXL1 belongs to the lysyl oxidase family and is an enzyme that catalyzes cross-linking of collagen and elastin 3). Reduced function of LOXL1 disrupts elastic fiber homeostasis, leading to accumulation of abnormal fibrous material.
Mechanism of intraocular pressure elevation: Exfoliative material and pigment granules accumulate in the trabecular meshwork and Schlemm’s canal, increasing aqueous humor outflow resistance. Production of exfoliative material by trabecular cells, phagocytosis of pigment granules by trabecular cells, and abnormal deposition of extracellular matrix due to inhibition of elastic fiber formation are also involved 2).
Mechanism of zonular weakness: The zonules of Zinn are composed of microfibrils mainly containing fibrillin-1. In XFS, pseudoexfoliative material deposits along the zonules, and degradation by lysosomal enzymes (MMPs) is promoted. This leads to progressive loss of support function over time 8).
The frequency of zonular rupture during cataract surgery in XFS is reported to be four times that of the control group 8). This finding indicates that intraoperative mechanical manipulation reveals the vulnerability of the zonules.
Rare combined case: A case of MRCS syndrome (Microcornea-Rod-Cone Dystrophy-Cataract-Posterior Staphyloma) combined with XFS has been reported, where the combination of fibrous material deposition characteristic of XFS and severe axial length elongation (axial length 30.9 mm) caused marked weakening of the Zinn zonules8).
Risk of lens dislocation in surgeries other than cataract surgery: XFS patients have potential Zinn zonule weakness and are at risk of lens dislocation during intraocular surgeries other than cataract surgery. Yamamoto et al. (2025) reported a case of a 78-year-old man with pseudoexfoliation glaucoma who experienced spontaneous posterior lens dislocation immediately after trocar insertion during vitreous surgery9). Although no lens instability was confirmed preoperatively, fibrous pseudoexfoliation material deposition and weakness on the Zinn zonules were observed intraoperatively. This case highlights the need to consider lens dislocation in all intraocular surgeries for XFS patients.
Genome-wide association studies (GWAS) have identified multiple susceptibility loci besides LOXL1. CACNA1A, POMP, AGPAT1, RBMS3, SEMA6A, and others have been reported. Elucidating the functions of these gene products will deepen understanding of the pathology and may become future therapeutic targets. Associations between genetic polymorphisms in vascular tone pathways and POAG have also been reported3).
Research is underway to identify small molecule compounds that regulate LOXL1 expression. Additionally, TGF-β1 has been shown to promote the production of fibrous material in XFS, and inhibition of the TGF-β signaling pathway is being studied as a therapeutic strategy.
Quantification of pseudoexfoliative material and related proteins in aqueous humor and serum may be useful for monitoring disease activity. It is expected to be applied to preclinical diagnosis and risk stratification.
Compared to POAG, intraocular pressure levels are higher, progression is more aggressive, and many cases have poor prognosis. Even with early detection and treatment, visual field damage may progress. Cases with large intraocular pressure fluctuations require particular attention, and analysis of the Early Manifest Glaucoma Trial (EMGT) has confirmed the rapid progression of pseudoexfoliative glaucoma7). Early initiation of aggressive treatment is important.
Elhawy E, Kamthan G, Dong CQ, Danias J. Pseudoexfoliation syndrome, a systemic disorder with ocular manifestations. Hum Genomics. 2012;6:22. doi:10.1186/1479-7364-6-22. https://pmc.ncbi.nlm.nih.gov/articles/PMC3500235/
Thorleifsson G, Magnusson KP, Sulem P, et al. Common sequence variants in the LOXL1 gene confer susceptibility to exfoliation glaucoma. Science. 2007;317(5843):1397-1400. doi:10.1126/science.1146554.
European Glaucoma Society. European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition. Br J Ophthalmol. 2021 Jun;105(Suppl 1):1-169. doi:10.1136/bjophthalmol-2021-egsguidelines. PMID:34675001.
Fontana L, Coassin M, Iovieno A, et al. Cataract surgery in patients with pseudoex-foliation syndrome: current updates. Clin Ophthalmol. 2017;11:1377-1383. doi:10.2147/OPTH.S142870. PMID:28814824; PMCID:PMC5546806.
Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P71-P150. doi:10.1016/j.ophtha.2020.10.022. PMID:34933745.
Wang X, Jiang X, Liu Z, Wang C, Li X. Coexistence of MRCS syndrome, extremely long axis and exfoliation syndrome: a case report and literature review. BMC Ophthalmol. 2023;23(1):241. doi:10.1186/s12886-023-02965-7. PMID: 37254066; PMCID: PMC10227401.
Yamamoto MH, Au A, Giaconi J, Tsui I. Spontaneous Crystalline Lens Dislocation Associated With Pseudoexfoliation Glaucoma: An Unexpected Complication of Vitrectomy. Journal of vitreoretinal diseases. 2025. doi:10.1177/24741264251386412. PMID:41185663; PMCID:PMC12579588.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.