Definition
Cause: Incomplete regression of glial tissue surrounding the hyaloid artery during embryonic development
Also known as: Epipapillary veil
First reported: 1877 by Otto Bergmeister (Austria)

Bergmeister papilla is a congenital finding in which the glial tissue surrounding the hyaloid artery during the fetal period fails to regress after birth. It was first reported in 1877 by Austrian ophthalmologist Otto Bergmeister. It is also called epipapillary veil.
Bergmeister papilla is a type of persistent fetal vasculature (PFV) and is classified as a remnant of the posterior hyaloid artery [1,2]. The PFV spectrum also includes Mittendorf dot (remnant on the posterior lens capsule), persistent hyaloid artery, persistent pupillary membrane, and persistent hyperplastic primary vitreous [1,2].
The hyaloid artery normally regresses and disappears before birth. When regression is incomplete, a sheath of glial tissue remains on the optic disc, forming Bergmeister papilla. It is usually asymptomatic and is often discovered incidentally during fundus examination.
Definition
Cause: Incomplete regression of glial tissue surrounding the hyaloid artery during embryonic development
Also known as: Epipapillary veil
First reported: 1877 by Otto Bergmeister (Austria)
Classification
Superordinate concept: Persistent fetal vasculature (PFV)
Classification: Posterior remnant of the hyaloid artery
Related types: Mittendorf dot, persistent hyaloid artery, Cloquet’s canal
Prognosis
Natural course: Mostly asymptomatic and stable
Treatment: Not required if no complications
Rare exception: Complications due to thrombosis of the prepapillary vascular loop
It is a relatively common congenital finding in PFV. Related Mittendorf dots are found in 1–2% of normal individuals. Minor residual glial tissue is often discovered incidentally without symptoms.
Usually asymptomatic, discovered incidentally during visual acuity or fundus examination. Visual impact depends on secondary involvement of the retina or macula.
A rare complication is the formation of a vitreous cyst, which can cause floaters and transient vision loss.
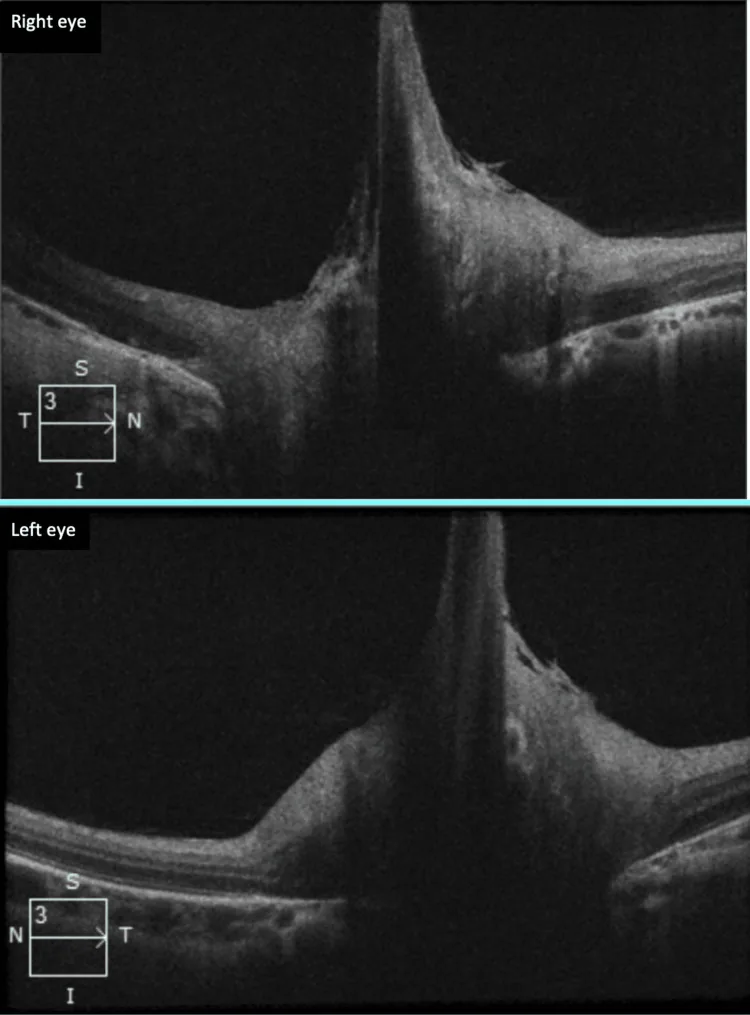
Observed as a membranous glial tissue protruding from the anterior, central, or nasal side of the optic disc. It may be unilateral or bilateral. It can affect the apparent size of the optic cup.
It may be vascularized by retinal vessels, in which case it is observed as a prepapillary vascular loop.
Bergmeister papilla is caused by incomplete regression of the hyaloid artery during the embryonic period.
The hyaloid artery branches from the internal carotid artery via the dorsal and ventral ophthalmic arteries at the end of the 4th week of gestation, enters the primary vitreous through the embryonic fissure, reaches the posterior surface of the lens to form the vasa hyaloidea propria, and supplies nutrients to the developing eye. When the secondary vitreous begins to form from the retinal side at the 6th week of gestation, the primary vitreous is pushed toward the center of the vitreous cavity.
The hyaloid artery normally loses function around the 6th month of gestation, transforms into the Cloquet canal around the 30th week of pregnancy, and regresses before birth. Bergmeister papilla is the remnant of glial tissue on the optic disc that persists without undergoing this regression process.
Deficiency of genes that induce apoptosis is thought to be involved in the overall development of PFV. It is common in preterm infants but also seen in full-term infants.
The spectrum of PFV is shown below.
| Type | Location | Characteristics |
|---|---|---|
| Mittendorf dot | Posterior lens capsule | 1–2% of normal individuals |
| Bergmeister papilla | On the optic disc | Remnant of glial tissue |
| Persistent hyaloid artery | Within the vitreous cavity | Rare cause of bleeding |
Diagnosis of Bergmeister papilla is based on fundus examination, combined with OCT or fluorescein angiography (FA) as needed.
The main examination methods are shown below.
| Examination method | Role | Notes |
|---|---|---|
| Fundus examination | Visual inspection | Initial screening |
| OCT | Detailed structural imaging | Useful for definitive diagnosis |
| FA | Assessment of vascularization | Detection of vascular loops |
The most important differential diagnosis is regressed optic disc neovascularization (NVD).
The differential diagnosis of severe PFV (formerly called PHPV) becomes an issue when it presents with leukocoria. In such cases, differentiation from retinoblastoma is necessary, and FA, electroretinography, ultrasound, CT, and MRI are useful for diagnosis.
Bergmeister papilla is congenital glial tissue and is not associated with vascular disease or inflammation. Papillary neovascularization occurs secondary to ischemia or inflammation. FA is useful for differentiation by confirming the presence of vascularization and fluorescein leakage pattern.
Bergmeister papilla without complications does not require treatment. Regular follow-up alone is sufficient, and the prognosis is favorable in the majority of cases.
If complications due to thrombosis of a prepapillary vascular loop occur (such as BRAO, BRVO, or vitreous hemorrhage), treatment is given according to the specific condition. If a vitreous cyst causes floaters or decreased vision, management is considered based on the severity of symptoms.
If there are no complications, treatment is not necessary. The prognosis is favorable in most cases, and regular follow-up is usually sufficient. Only when rare complications such as prepapillary vascular loop thrombosis occur, treatment is given according to the condition.
The mechanism of Bergmeister papilla involves incomplete regression of the hyaloid artery during embryonic development.
Formative Stage (4–6 weeks of gestation)
Branching of the hyaloid artery: The internal carotid artery gives rise to the dorsal and ventral ophthalmic arteries, which form the hyaloid artery.
Entry into the primary vitreous: The artery passes through the embryonic fissure into the primary vitreous, reaches the posterior lens surface, and forms the tunica vasculosa lentis.
Formation of glial tissue: Glial tissue surrounds the artery at the optic disc.
Regression Phase (13 weeks gestation to late stage)
Formation of the secondary vitreous: Starting from the 6th week of gestation, the secondary vitreous begins to form from the retinal side. The primary vitreous becomes confined to the Cloquet canal.
Initiation of regression: The hyaloid artery begins to regress from the 13th to 15th week of gestation and loses function around the 6th month of gestation.
Transformation into the Cloquet canal: Around the 30th week of pregnancy, the remaining lumen forms the Cloquet canal.
Residual Patterns at Birth
Normal: The hyaloid artery completely disappears, leaving only the Cloquet canal.
Bergmeister papilla: A glial sheath on the optic disc that fails to regress and remains.
Mittendorf dot: A remnant of the anterior end of the hyaloid artery on the posterior lens capsule (present in 1–2% of normal individuals).
From the 9th week of gestation, fine fibers appear and form an acellular reticular structure (secondary vitreous). As the secondary vitreous increases, the primary vitreous and the hyaloid artery within it become confined to the central axis of the vitreous cavity as the Cloquet canal. The hyaloid artery develops most prominently at 5–6 weeks of gestation, begins to regress from 13–15 weeks, and normally disappears in the later stages.
When regression is incomplete, the glial sheath on the optic disc remains as a Bergmeister papilla. Deficiency in genes that induce apoptosis is thought to be involved in this incomplete regression.