A bleb leak is a condition in which aqueous humor leaks out of the eye through the wall of a filtering bleb formed after glaucomafiltration surgery (such as trabeculectomy or Ex-PRESS shunt surgery). It is confirmed by a positive Seidel test using fluorescein. This is a complication specific to filtration surgery and is not typically seen in other ophthalmic surgeries.
Based on the time of onset, bleb leaks are broadly classified as follows.
Early leak: Occurs within 1 month after surgery. The main causes are suture site insufficiency or conjunctival wound closure failure. In many cases, spontaneous closure can be expected with suture adjustment of the scleral flap or conservative management.
Late bleb leak: Occurs 1 month or more after surgery. It often results from thinning and avascularity of the bleb wall due to the use of antimetabolites, and is clinically problematic. Late leaks are less likely to close spontaneously and often require surgical intervention.
Furthermore, based on persistence, leaks are divided into transient and persistent leaks. Persistent leaks carry a high risk of infection and may progress to hypotony maculopathy, thus requiring more aggressive treatment.
The incidence of aqueous humor leakage from the conjunctival wound in the early period after trabeculectomy is reported to be 3.4–14% 1). When mitomycin C (MMC) is used, the risk of leakage over 5 years after surgery reaches 15% 2). The incidence of hypotony maculopathy occurring 1 month or more after surgery is 0.9–5% 1).
Bleb leak is the greatest risk factor for bleb infection, increasing the infection risk by 26 times. The cumulative incidence of bleb-related infection within 5 years after trabeculectomy with MMC is reported to be 2.2%2).
Trabeculectomy is the most established filtering surgery for glaucoma, offering excellent long-term intraocular pressure reduction, but complications related to the filtering bleb can occur throughout the patient’s life. Bleb leak is one of the representative complications, and early detection and appropriate management of the leak determine the long-term postoperative prognosis.
This article covers the management of bleb leak (the leak itself). For details on infections secondary to leakage, see Bleb-related infections.
QWhat is the difference between bleb leak and bleb infection?
A
Bleb leak refers to the leakage of aqueous humor through the bleb wall, confirmed by a positive Seidel test. In contrast, bleb infection (bleb-related infection) is an infectious complication caused by bacterial entry through the leak site. Bleb leak is the greatest risk factor for infection, but many cases involve leakage without infection. Prompt closure of the leak is key to preventing infection.
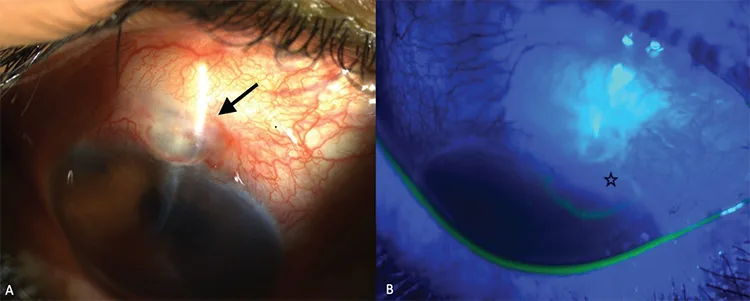
Yalniz-Akkaya Z, Burcu A, Ornek F. Late-Onset Glaucoma-Filtrating Bleb Leak in a Penetrating Keratoplasty Patient: A Case Report. Case Rep Ophthalmol Med. 2012;2012:810751. Figure 2. PMID: 22606503; PMCID: PMC3349998. DOI: 10.1155/2012/810751. License: CC BY 3.0.
Bleb leak 10 years after trabeculectomy: A shows an avascular bleb (black arrow) on slit-lamp examination of the right eye, and B shows conjunctival defect and leakage (black star) demonstrated by Seidel test. This corresponds to the aqueous humor leakage discussed in section “2. Main symptoms and clinical findings.”
Bleb leak itself is often asymptomatic, but may be accompanied by the following symptoms.
Tearing upon waking: Reflects the finding that aqueous humor seeps out when the upper eyelid is elevated due to a thin bleb wall2)
Discomfort due to low intraocular pressure: May cause mild foreign body sensation or dull pain. However, even with low intraocular pressure, it is not uncommon to be asymptomatic.
Decreased vision: Occurs when hypotony maculopathy develops. It is due to the formation of choroidal folds or macular folds, which can lead to permanent visual impairment if persistent. Often perceived as blurred vision.
Redness and irritation: May be accompanied by mild conjunctival injection around the leakage site. Marked redness or pain suggests possible infection.
Observation of the bleb appearance is primarily performed using slit-lamp microscopy, and the following five items are assessed.
Bleb extent (spread): Diffuse blebs have better intraocular pressure-lowering effects than localized blebs. Extensive conjunctival dissection during surgery to ensure a large area for aqueous humor diffusion promotes the formation of low, wide filtering blebs and also helps prevent leakage.
Bleb height: Low, flat blebs suggest reduced filtering function. Conversely, high, tense, localized blebs place greater mechanical stress on the wall and pose a risk of leakage.
Bleb wall thickness: Trabeculectomy with antimetabolites frequently results in thinning of the bleb wall. Thin-walled blebs often achieve good intraocular pressure reduction but are prone to aqueous humor leakage, requiring caution. When the slit beam of the slit lamp is directed laterally at the bleb wall, transparency of thin areas can be easily evaluated.
Vascularity: Avascular blebs have a high risk of aqueous humor leakage. Ischemic blebs also have reduced conjunctival barrier function, increasing infection risk. Conversely, blebs with a thick wall and dilated invading vessels are called encapsulated blebs, a different condition that leads to elevated intraocular pressure.
Presence of aqueous humor leakage by Seidel test: After staining with fluorescein strips, the entire bleb is observed under cobalt blue light. If leakage is present, the fluorescein is diluted by aqueous humor and appears to flow (see “Diagnosis and Examination Methods” section for details).
Hypotony maculopathy: characterized by shortened axial length, choroidal folds, macular folds, tortuous retinal vessels, and optic disc edema. It is more common in young myopic eyes1)
Anterior segment OCT: objectively evaluates bleb wall thickness and internal structure4). Combined with slit-lamp examination, it provides a comprehensive assessment of bleb filtration function
B-mode ultrasound: useful for evaluating the extent of choroidal detachment
Use of antimetabolites (MMC, 5-FU): The most important risk factor. Causes thinning and avascularity of the bleb wall. Decreased mucin production due to reduction of goblet cells weakens the conjunctival physical and immunological barrier. Postoperative subconjunctival injection of 5-FU has been shown to increase the frequency of aqueous humor leakage1)
Scleral flap suture insufficiency: Main cause of early leakage. Occurs when the number or strength of sutures during surgery is insufficient
Conjunctival closure insufficiency: Aqueous humor leaks due to inadequate suturing of the conjunctival incision or tissue fragility
Young age and myopia: Higher risk of hypotony maculopathy1). The eye wall is more flexible and susceptible to axial shortening due to low intraocular pressure
Tendency for conjunctival scarring: In cases of reoperation or inflammatory disease, conjunctival tissue is fragile and healing capacity is reduced
Comorbid blepharitis and conjunctivitis: Chronic inflammation of the ocular surface reduces the barrier function of the conjunctiva, increasing the risk of both leakage and infection
Diabetes: May be a factor in delayed wound healing
QWhy does using antimetabolites increase the risk of bleb leak?
A
Antimetabolites such as mitomycin C (MMC) and 5-FU are used to suppress scar formation around the filtering bleb, thereby maintaining long-term intraocular pressure reduction. However, they also promote thinning and avascularity of the bleb wall and reduce mucin production due to decreased goblet cells. These changes weaken the conjunctival barrier and increase the risk of aqueous humor leakage.
The Seidel test is used for definitive diagnosis of bleb leak. It is recommended to perform this test routinely at each examination after trabeculectomy to assess for leakage. The procedure is as follows.
Preparation of test strip: Gently apply a fluorescein strip moistened with topical anesthetic to the bleb surface. Avoid excessive pressure on the conjunctiva, as this may cause artificial leakage; only light contact is needed.
Observation conditions: Observe the entire bleb under cobalt blue light (blue filter). Reducing ambient lighting improves detection of small leaks.
Eyelid closure/opening method: Have the patient close the eyes, then observe the entire bleb for a few seconds immediately after opening; this makes evaluation easier. Eyelid closure temporarily promotes leakage due to pressure on the eyelids.
Positive determination: If aqueous humor leaks from the bleb, fluorescein diluted by the aqueous humor can be seen flowing (positive Seidel test). A characteristic finding is the outflow of diluted fluid emitting green fluorescence from the leak site against the surrounding orange staining.
Recording the leak: It is clinically important to record the leak location (e.g., bleb apex, margin, conjunctival suture site) and extent. Recording the amount of leakage helps determine treatment strategy.
Representative bleb classification systems based on appearance include the Moorfields Bleb Grading System (MBGS) and the Indiana Bleb Appearance Grading Scale (IBAGS). These systems score bleb extent, height, vascularity of the wall, and wall thickness, and are used for functional evaluation of filtering blebs and stratification of leakage risk. Recording scores over time allows objective tracking of morphological changes and progression of thinning.
Anterior segment OCT can evaluate bleb wall thickness, cavity status, and subconjunctival tissue characteristics in cross-sectional images 4). It is useful for detecting subtle wall thinning that is difficult to assess by slit-lamp examination and for longitudinal evaluation of treatment effects.
In bleb infection, debris may temporarily occlude the leakage site, causing the Seidel test to be negative. If an opaque, white, cloudy bleb surrounded by hyperemic conjunctiva (so-called “white-on-red”) is observed, infection should be suspected, and a detailed examination including conjunctival swab and aqueous humor culture should be performed. Overfiltration is excessive aqueous outflow from the scleral flap, leading to hypotony and shallow anterior chamber, but it is distinguished from bleb leak by the absence of conjunctival leakage.
Treatment for bleb leak is selected based on the degree of leakage, bleb vascularity, and presence of complications. Since aqueous leakage is a significant risk factor for bleb infection, it must be promptly controlled 2).
Leaks occurring in vascularized conjunctiva have a relatively high chance of closure with conservative treatment.
Non-invasive Treatment
Pressure patch: Accurately compress the scleral flap with gauze, etc. Also effective for improving overfiltration.
Bandage contact lens (BCL): A large-diameter soft contact lens of 18 mm is worn to promote wound closure.
Aqueous humor suppressants: Reduce leakage by decreasing aqueous humor production via eye drops.
Atropine sulfate hydrate eye drops: Suppress aqueous humor production by relaxing the ciliary body, and are also expected to have anti-inflammatory effects1).
Minimally Invasive Procedures
Autologous blood injection: A method of injecting the patient’s own blood into and around the filtering bleb. Improvement of hypotony maculopathy has been reported3).
Cyanoacrylate tissue adhesive: Applied locally to small leakage sites to seal them.
Intracameral injection of viscoelastic material or air: Forms the anterior chamber and temporarily suppresses leakage.
If conservative treatment does not improve the condition or if hypotony maculopathy develops, surgical intervention is performed.
Transconjunctival scleral flap suture: A method of suturing the scleral flap directly with nylon thread through the conjunctiva, which has shown long-term effectiveness in treating hypotony maculopathy3). It is also used to suppress overfiltration.
Direct scleral flap suture: When transconjunctival approach is not possible, the conjunctiva is opened surgically and the scleral flap is sutured under direct visualization. If marked choroidal detachment is present, drainage via sclerostomy is performed concurrently1).
Avascular bleb excision with conjunctival advancement: A method of excising an avascular bleb with aqueous humor leakage and advancing the posterior normal conjunctiva and Tenon’s capsule. It has been reported that aqueous leakage stops in approximately 90% of cases after a single surgery, and there is no recurrence including reoperation cases3).
Tenon advancement with amniotic membrane: A surgical technique combining conjunctival advancement with amniotic membrane, reported to be effective in cases with insufficient conjunctival tissue or recurrent cases3).
Mild or transient leakage with maintained intraocular pressure → Attempt conservative treatment for 2–4 weeks. Leakage from a well-vascularized conjunctiva may close spontaneously.
Persistent leakage causing hypotony → Consider surgical intervention in addition to conservative treatment.
When hypotony maculopathy develops → Promptly perform aggressive surgical closure. Early intervention before visual function becomes fixed is important.
If infection is present → urgent antibiotic treatment and surgical intervention are required (see Bleb-related infection for details)
The Glaucoma Practice Guidelines (5th edition) recommend the following regarding antibiotic use after trabeculectomy1)2).
Early postoperative period: Continuous instillation of fluoroquinolone antibiotics is recommended for 1–3 months (strength of recommendation: strong recommendation to “do it”, strength of evidence: C)
Long-term postoperative period: If bleb leakage is present, consider using fluoroquinolone antibiotic ointment before bedtime. Long-term use significantly delays the onset of bleb infection (non-use group: 3.9 years vs. long-term use group: 6.4 years vs. ointment group: 10.5 years)2)
QWhat is autologous blood injection treatment?
A
Autologous blood injection is a treatment in which the patient’s own blood is collected and injected into and around the filtering bleb3). The clotting action of the blood promotes closure of the leakage site. While improvement of hypotony maculopathy has been reported, it can cause a sudden rise in intraocular pressure3), so strict postoperative intraocular pressure monitoring is necessary.
QCan bleb leak be treated with surgery?
A
If conservative treatment does not improve the condition, surgical treatment is performed. Excision of the avascular filtering bleb and conjunctival advancement have been reported to stop leakage in about 90% of cases with a single surgery, and recurrence is rare3). The use of amniotic membrane transplantation in combination has also been reported to be effective3). The indication for surgery is determined by the degree of leakage, bleb characteristics, and presence of complications.
6. Pathophysiology and Detailed Mechanism of Onset
Trabeculectomy is a surgery that creates a window in the limbal corneosclera, establishing a non-physiological aqueous humor outflow pathway from the anterior chamber to the subconjunctival tissue 1). Postoperative intraocular pressure is determined by the balance between aqueous humor production and outflow through the scleral flap into the filtering bleb.
During the postoperative wound healing process, scar tissue forms in the subconjunctival tissue. Since this scarring can lead to reduced bleb function (elevated intraocular pressure), the standard management involves using MMC to suppress early excessive tissue reactions and increase the likelihood of long-term bleb maintenance 1). However, MMC also induces the following changes.
Conjunctival thinning: The physical fragility of the bleb wall increases, making aqueous humor transudation and leakage more likely. The intraoperative MMC concentration (typically 0.2–0.4 mg/mL) and application time influence the degree of thinning.
Avascularity: Neovascularization of the conjunctiva is suppressed, reducing repair capacity. An avascular bleb also diminishes nutrient supply to the conjunctival epithelium, delaying epithelial turnover.
Goblet cell depletion: Reduced mucin production impairs the protective function of the conjunctival surface. The mucin layer stabilizes the tear film and acts as a physical barrier against microorganisms; its loss increases the risk of both leakage and infection.
Fibroblast inhibition: Fibroblasts, the primary mediators of wound repair, are reduced, decreasing the self-repair capacity of the bleb wall.
These changes act in combination, sustaining the risk of bleb leak from the early to late postoperative period. Particularly during the first few months after surgery, when scarring progresses rapidly, the outflow resistance of the scleral flap and bleb morphology change dynamically, requiring timely intervention.
Differences in mechanisms between early and late leakage
Early leakage is mainly due to mechanical failure of the surgical wound. The main causes are suture insufficiency of the scleral flap, dehiscence of the conjunctival incision, or excessive filtration due to a sudden change in the balance of aqueous humor production and outflow. It has been shown that additional postoperative subconjunctival injection of 5-FU increases the frequency of aqueous humor leakage in addition to corneal epithelial damage 1).
Late leakage occurs as a result of chronic tissue degeneration caused by antimetabolites. Progressive thinning of the bleb wall over a long period exceeds a critical point at some time, and transmural leakage of aqueous humor becomes apparent. Mechanical trauma (such as rubbing the eye) may also trigger it.
These combined factors lead to severe visual impairment (hypotony maculopathy). Transient postoperative hypotony does not affect long-term intraocular pressure, but persistent hypotony can cause irreversible macular changes.
Aqueous humor leakage from the filtering bleb provides a route for tears and periocular commensal bacteria to enter the eye through the leak site 2). The normal conjunctiva has multilayered defense mechanisms including epithelial tight junctions, mucin from goblet cells, and lysozyme and IgA in tears; however, in blebs weakened by antimetabolites, bacteria can easily invade through the leakage site.
The longer the leakage persists, the higher the infection risk. Once infection occurs, it may progress through the stage of blebitis (infection localized to the filtering bleb) to spread into the anterior chamber and further into the vitreous (bleb-associated endophthalmitis) 2). Bleb-associated endophthalmitis has been reported to result in visual acuity of 0.1 or worse in 94% of cases despite aggressive treatment, so prompt management at the bleb leak stage greatly affects prognosis.
7. Latest research and future perspectives (reports at the research stage)
For filtering blebs with leakage or hypotony, surgical repair such as avascular bleb excision or conjunctival advancement aims to achieve both leak closure and intraocular pressure control3).
In reoperation cases with insufficient healthy conjunctiva, repair methods combining conjunctival advancement with auxiliary materials such as amniotic membrane may be considered3).
Avoidance of leakage risk with minimally invasive glaucoma surgery (MIGS)
Minimally invasive glaucoma surgery (MIGS), which has become increasingly popular in recent years, includes many devices that do not form blebs, unlike traditional trabeculectomy. Because they drain aqueous humor via Schlemm’s canal or the suprachoroidal space, they do not create subconjunctival filtering blebs, structurally avoiding the risk of postoperative hypotony or bleb leak. However, the intraocular pressure-lowering effect is more limited than trabeculectomy, and indications are often restricted to mild to moderate glaucoma. Some MIGS devices that form subconjunctival blebs exist, but since they do not use antimetabolites, the leakage risk is reduced compared to traditional trabeculectomy.
Advances in bleb evaluation using anterior segment OCT
Kojima et al. (2015) reported the evaluation of filtering bleb internal structure using anterior segment OCT4). Since it allows quantitative assessment of wall thickness, low-reflectivity areas in the lumen, and subconjunctival tissue characteristics, it is expected to be applied for predicting microleaks and leakage risk that are difficult to detect with Seidel testing alone. In the future, AI-based OCT image analysis is expected to enable automatic detection of progressive bleb wall thinning and prediction of the optimal timing for preventive intervention before leakage occurs.
In addition to amniotic membrane transplantation, reports on bleb repair methods using biomaterials such as collagen matrix and fibrin glue are accumulating. For cases where healthy conjunctiva is insufficient for conventional conjunctival advancement, the development of conjunctival substitutes through tissue engineering approaches is also under research.