A phakic intraocular lens (pIOL) is a surgery that inserts an intraocular lens into the eye while preserving the natural lens to correct refractive errors. Similar to intraocular lens implantation in cataract surgery, it is an intraocular procedure performed under an operating microscope, but differs in that the lens is not removed.
pIOL is mainly indicated for moderate to high myopia (especially -6 D or more). Since the cornea is not ablated, there is no risk of corneal ectasia. Advantages include preservation of accommodation and excellent reversibility. It is particularly useful for cases unsuitable for LASIK or PRK, and for patients with thin corneas.
Historically, Strampelli developed the first anterior chamber pIOL in 1953. Early lenses had many complications such as corneal endothelial failure and glaucoma, but in 1977 Worst developed the iris-fixated lens (iris claw), and in 1986 Fyodorov developed the posterior chamber type, greatly improving safety. Currently, STAAR Surgical’s Visian Implantable Collamer Lens (ICL) is the most widely used posterior chamber pIOL.
In Japan, posterior chamber pIOL is mainstream. Under topical anesthesia, an ophthalmic viscosurgical device is injected into the anterior chamber, and the lens is inserted between the iris and the natural lens using a dedicated injector. Types with astigmatism correction and central hole (perforated) are also approved.
QWhich is better: posterior chamber phakic intraocular lens or LASIK?
A
Both have advantages and disadvantages. Posterior chamber phakic intraocular lens does not ablate the cornea, so there is no risk of corneal ectasia; it can correct high myopia and preserves accommodation. LASIK is simpler and has faster postoperative recovery. For high myopia (-6 D or more), posterior chamber phakic intraocular lens offers better visual quality (higher-order aberrations, contrast sensitivity). For mild to moderate myopia, LASIK is often the first choice. Posterior chamber phakic intraocular lens is also advantageous for thin corneas or severe dry eye.
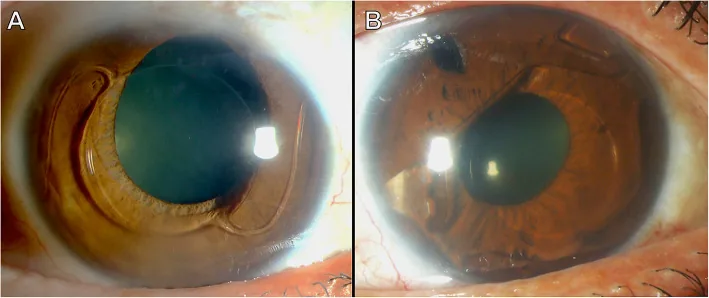
Timur M Yildirim et al. Reasons for explantation of phakic intraocular lenses and associated perioperative complications: cross-sectional explant registry analysis. BMC Ophthalmology. 2021 Feb 12; 21:80. Figure 1. PMCID: PMC7879667. License: CC BY.
Representative example: AcrySof (Alcon). The support is placed in the anterior chamber angle.
Complications: Chronic loss of corneal endothelial cells, pupil ovalization, and nuclear cataract were problematic, and it has now been withdrawn from the market. It is not recommended for refractive correction in young patients.
Features: Fixed to the mid-peripheral iris with claws. Chronic loss of corneal endothelial cells is a concern, but it is safer than angle-supported types. A large incision is required, and attention must be paid to postoperative astigmatism4).
Posterior Chamber (ICL)
Representative example: Visian Implantable Collamer Lens (STAAR Surgical). Made of Collamer material (hydroxyethyl methacrylate + collagen copolymer).
Features: Placed in the ciliary sulcus. It is away from the corneal endothelium, so the risk of endothelial cell loss is low. In the EVO/EVO+ models, the central hole reduces the risk of pupillary block and anterior subcapsular cataract. It can be inserted through a 3.0 mm small incision.
The ESCRS guidelines recommend preoperative evaluation for cataract surgery after anterior chamber pIOL implantation, including assessment of iris damage, patency of peripheral iridotomy, and confirmation of corneal endothelial cell density and morphology 4). Anterior chamber types requiring a large incision cause with-the-rule astigmatism, but foldable iris-fixated types have less astigmatic change due to the small incision 4).
QWhat is the central hole of the EVO phakic posterior chamber lens?
A
The central hole (KS-Aquaport) of the EVO/EVO+ phakic posterior chamber lens is a small hole with a diameter of 360 microns located in the center of the optic. Through this hole, aqueous humor flows physiologically across the anterior capsule surface, eliminating the need for preoperative peripheral iridotomy required with conventional types. Furthermore, improved aqueous humor supply to the anterior lens surface is thought to reduce the risk of anterior subcapsular cataract. It received FDA approval in 2022.
For anterior chamber lenses, the Van der Heijde nomogram is used to calculate power from refractive value, corneal refractive power, and anterior chamber depth. For posterior chamber phakic intraocular lenses, the Binkhorst nomogram is used to determine lens size from angle-to-angle distance or corneal diameter (WTW). The ESCRS guidelines recommend using biometric measurements taken before pIOL implantation when performing cataract surgery after pIOL implantation4).
For posterior chamber phakic intraocular lenses, the ideal distance between the lens and the anterior surface of the crystalline lens (vault) is 200 to 800 microns, which can be measured with anterior segment OCT.
Anterior chamberiris-fixated (Artisan/Verisyse): Performed under retrobulbar or peribulbar anesthesia. Under miosis, mark the corneal center, insert the lens with viscoelastic through a corneal or scleral incision. Fix the claws to the iris with a fixation needle. Perform peripheral iridectomy to prevent pupil block. Close the incision with 10-0 nylon.
Posterior chamber phakic intraocular lens (Visian ICL): Under mydriasis, insert the lens through a 3.0 mm incision using a dedicated injector. Position the haptics under the iris with a spatula. For EVO/EVO+, peripheral iridotomy is not required.
Corneal endothelial cell loss: This is the greatest concern common to anterior chamber lenses. Progressive cell loss can lead to corneal endothelial failure. Warrak et al. reported a case of cystoid macular edema (CME) 18 years after anterior chamber pIOL insertion 1).
Chronic inflammation: Subclinical inflammation due to microcontact between the lens and iris is suspected to cause cystoid macular edema1).
Haptic migration: Migration of the haptic into the peripheral iridotomy site has been observed in 23% of cases 1).
Complications of posterior chamber lenses
Cataract: Contact between the lens and the crystalline lens (low vault) can cause anterior subcapsular cataract2). The central hole in EVO/EVO+ reduces this risk.
Lens dislocation: Rarely occurs after trauma. Alsugayhi et al. reported two cases of phakic posterior chamber lens dislocation after blunt trauma, with good visual outcomes after early repositioning 3).
In the case of Warrak et al., cystoid macular edema due to occult low-grade inflammation developed 18 years after anterior chamber pIOL implantation, but completely resolved within 3 weeks with only ketorolac 0.5% eye drops 1). This is an important report showing that late-onset complications can occur even after a long period.
In the case of Mandal et al., TASS occurred after posterior chamber pIOL implantation, leading to a severe course requiring pIOL explantation, cataract surgery, and even corneal transplantation with scleral-fixated IOL2). The importance of early detection and intensive steroid treatment for TASS is emphasized.
Alsugayhi et al. reported two cases of phakic posterior chamber lens dislocation after trauma (young males aged 27 and 29), with good visual outcomes after repositioning within a few days of injury 3). Eye protection during contact sports is recommended for phakic posterior chamber lens wearers.
QWhat complications can occur after surgery?
A
Main complications include corneal endothelial cell loss (especially with anterior chamber type), cataract formation (with posterior chamber type if vault is insufficient), increased intraocular pressure (pupillary block, pigment dispersion glaucoma), and lens dislocation or decentration. Rarely, TASS (toxic anterior segment syndrome) or cystoid macular edema may occur 1)2). Early detection and appropriate management can improve visual prognosis for any complication, so regular follow-up is essential.
pIOL adjusts the focal point on the retina by placing an additional refractive lens inside the eye. In myopia, a concave (minus) lens delays convergence of light rays, moving the focal point from in front of the retina onto the retina. In hyperopia, a convex (plus) lens is used.
Unlike correction with glasses, intraocular lenses are located near the principal point of the eye, so there is almost no magnification or minification of the image, providing the most physiological vision. Compared to contact lenses, they induce fewer higher-order aberrations and maintain good contrast sensitivity.
Corneal endothelial cell loss: Anterior chamber phakic IOLs are positioned close to the corneal endothelium, and micro-movements of the lens cause mechanical stress on endothelial cells. Chronic cell damage leads to a gradual decrease in endothelial cell density over time, eventually resulting in corneal endothelial failure (bullous keratopathy).
Anterior subcapsular cataract: When the vault (distance between the lens and the anterior lens capsule) of a posterior chamber phakic IOL is insufficient, contact between the lens and the anterior capsule impairs aqueous humor circulation, causing metabolic disturbances in lens epithelial cells. The central hole in EVO/EVO+ improves this aqueous humor circulation disturbance.
TASS: Inadequate cleaning of surgical instruments, contaminants, or toxicity of intraocular solutions can cause acute non-infectious inflammation in the anterior segment 2). Severe cases can lead to corneal endothelial damage, peripheral anterior synechiae, and secondary glaucoma, requiring corneal transplantation.
EVO phakic posterior chamber IOLs with a central hole have significantly reduced the incidence of cataracts compared to conventional types. In a 5-year follow-up, no vision-affecting cataracts were reported, and the incidence of anterior subcapsular opacities not affecting vision was also low. It is believed that the physiological flow of aqueous humor across the anterior capsule contributes to maintaining lens health.
In recent years, comparative studies between phakic posterior chamber IOLs and SMILE for mild myopia (-3 to -6 D) have shown comparable safety and efficacy. Indications are expanding not only for high myopia but also for moderate myopia and hyperopia.
The advent of swept-source anterior segment OCT has enabled precise measurement of the angle-to-angle distance and sulcus-to-sulcus diameter. This has improved the accuracy of postoperative vault prediction, contributing to reduced risks of cataract and angle closure.
Warrak EL, Haddam MS, Dandan WN, Warrak JE, Sammouh FK. Cystoid Macular Edema 18 Years after Anterior ChamberPhakic Intraocular Lens Implantation. Case reports in ophthalmological medicine. 2022;2022:1853248. doi:10.1155/2022/1853248. PMID:35757521; PMCID:PMC9225911.
Mandal S, Sahay P, Tripathi M, Maharana PK. Complications following implantation of posterior chamber phakic intraocular lens (pIOL). BMJ case reports. 2022;15(12). doi:10.1136/bcr-2022-253876. PMID:36593609; PMCID:PMC9730352.
Alsugayhi M, Husain OB, Al-Swailem SA. Dislocation of implantable collamer lens following blunt trauma. American journal of ophthalmology case reports. 2023;29:101768. doi:10.1016/j.ajoc.2022.101768. PMID:36570105; PMCID:PMC9772575.
European Society of Cataract and Refractive Surgeons (ESCRS). ESCRS Clinical Guidelines for Cataract Surgery. Brussels: ESCRS; 2024.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.