A second opinion is seeking the opinion of an ophthalmologist other than the current primary physician regarding diagnosis and treatment plan. This is a consultation and is fundamentally different from a transfer of care, which involves changing healthcare institutions or primary physicians. It helps the patient refer to another doctor’s opinion and facilitates further discussion with the primary physician. Therefore, the institution providing the second opinion does not perform new examinations or tests but gives an opinion based on the provided medical information letter. Since it is not covered by health insurance, the cost is borne by the patient.
Refractive surgery is an irreversible treatment that involves invasion of the normal anterior segment of the eye. Because there are uncertainties in long-term outcomes, careful judgment of surgical indication is required1). In addition to being a board-certified ophthalmologist of the Japanese Ophthalmological Society, the surgeon must be proficient in the physiology, diseases, and optics of the anterior segment including the cornea and lens. Attendance at the Refractive Surgery Seminar designated by the Japanese Ophthalmological Society and seminars sponsored by manufacturers is also mandatory1).
The main situations in which a second opinion is sought for refractive surgery are as follows.
Preoperative: When there is concern about surgical indication (suspected keratoconus, thin cornea, high refractive error)
Preoperative: When the patient wants another specialist to confirm whether surgery is indicated
Postoperative: When expected visual acuity is not achieved or is worse than before surgery
Postoperative: When complications such as halos, glare, or dry eye occur
When considering reoperation: Assessment of suitability for enhancement surgery (residual corneal thickness, risk of ectasia)
In obtaining informed consent, it is required to clearly inform the patient that a second opinion can be obtained and to record the patient’s intention in the consent form.
QWhen should I seek a second opinion?
A
Since refractive surgery is irreversible, a second opinion is useful when there is concern about preoperative suitability (suspected keratoconus, thin cornea, high refractive error, etc.), or when expected visual acuity is not achieved postoperatively, complications persist, or an enhancement surgery is proposed but its suitability is questionable. Unlike changing doctors, the goal is to obtain an opinion to aid in further discussion with the primary physician. The cost is out-of-pocket, but it is a recognized patient right.
2. Main Symptoms and Clinical Findings (Triggers for Seeking a Second Opinion)
Provide opinions from an objective and professional standpoint. State views based on scientific evidence, and do not comment on evaluations of the current medical institution or physician, matters related to medical accidents or lawsuits, or content outside one’s own specialty. After the consultation, prepare a written opinion and send it to the primary care physician.
3. Causes and risk factors (risks of inappropriate surgery)
The main causes of complications after refractive surgery are broadly divided into overlooking contraindications, exceeding the limit of correction, and inadequate informed consent (IC).
Severe dry eye: Postoperative worsening, decreased visual quality
Pregnancy and breastfeeding: Hormonal fluctuations cause unstable refraction
Missed detection of subclinical keratoconus: Occurs when tests such as BAD-D and epithelial thickness mapping are insufficient3)
Cautious cases include glaucoma, connective tissue diseases, use of psychotropic medications, history of corneal herpes, and history of refractive surgery1).
Excimer laser surgery (LASIK, PRK, SMILE) is generally indicated up to 6 D, and up to 10 D with informed consent. It is essential to ensure a residual corneal stromal bed thickness of 250 μm or more1). Phakic intraocular lenses (phakic IOL) are indicated for myopia of 6 D or more, with cautious indication for 3 D to less than 6 D, and caution for over 15 D1).
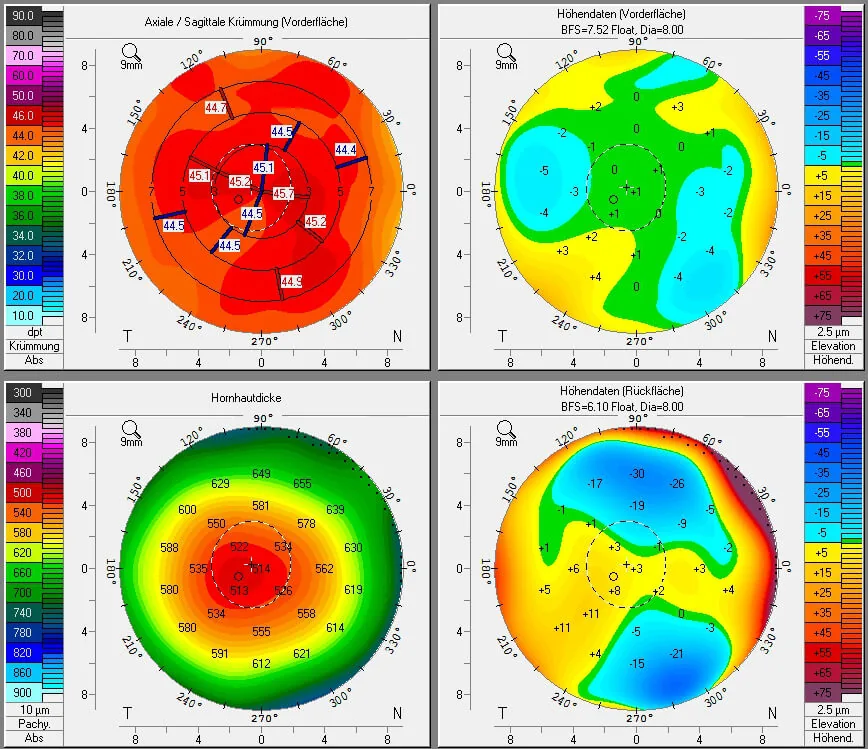
Four-panel corneal tomography obtained with Pentacam (Scheimpflug camera) before LASIK. Upper left: axial/sagittal curvature map (central 44–46 D, uniform distribution). Upper right: anterior elevation map (BFS 7.52, normal deviation within +4 μm). Lower left: pachymetry map (thinnest point 514 μm, central thickness around 530 μm). Lower right: posterior elevation map (BFS 6.10, within ±5 μm at center). Corresponds to corneal topography/tomography, corneal thickness measurement, and ectasia risk assessment discussed in section “4. Diagnosis and examination methods (tests to confirm with a second opinion).”
Combined evaluation of anterior-posterior height difference and corneal thickness3)
PTA (Percent Tissue Altered)
<40%: low risk
(Flap thickness + ablation depth) ÷ preoperative central corneal thickness7)
Randleman Score
0–2: low risk, 4 or higher: high risk
Combination of age, corneal thickness, topography, RSB, and correction amount
Epithelial Thickness Mapping
Epithelial donut pattern = ectasia
Can differentiate from CL warpage
BAD-D is a score that integrates five parameters (dp, db, df, dt, dy) based on anterior-posterior height difference and corneal thickness 3). PTA of 40% or more is significantly associated with corneal ectasia even in eyes with normal preoperative corneal shape 7). Epithelial thickness mapping shows an “epithelial donut pattern” with epithelial thinning at the steepening area in ectatic diseases, which can be differentiated from contact lens warpage (epithelial thickening at the steepening area) 3).
To exclude corneal deformation due to contact lenses (warpage), preoperative examinations should be performed after a cessation period of about 2 weeks for soft lenses and about 3 weeks for hard lenses 3).
QWhat kind of examination data should I bring for a second opinion?
A
Preoperative corneal shape analysis data (topography/tomography), preoperative and postoperative refraction values and corrected visual acuity, and postoperative course records (details of complication management) are particularly important. If possible, bringing current corneal shape analysis and anterior segment OCT data will help evaluate the progression of ectasia. Since a second opinion is given based on the provided medical information letter, it is recommended to obtain the letter from the primary doctor before making an appointment.
5. Standard Treatment Methods (Criteria for Surgical Technique Selection)
Scene just before the surgeon applies the suction ring (blue) for eyeball fixation to the patient’s eye and creates the corneal flap with a microkeratome during LASIK surgery. The eyelids are fixed with a lid speculum, and the surgical field is illuminated by the operating microscope. This corresponds to LASIK flap-related complications (free cap, flap wrinkles, epithelial ingrowth) discussed in the section “5. Standard Treatment Methods (Criteria for Surgical Technique Selection).”
The ablation depth for LASIK is estimated using the Munnerlyn formula.
t = S²D / 3 (t: ablation depth [μm], S: optical zone diameter [mm], D: spherical equivalent)
RSB (residual stromal bed) = central corneal thickness − ablation depth − flap thickness, ensuring a minimum of 250 μm (safe margin 300 μm). For SMILE, a planning protocol maintaining a minimum RST of 220 μm and total uncut stromal thickness of 300 μm is adopted 2). An optical zone exceeding the pupil diameter by more than 15% can effectively suppress higher-order aberrations 3).
QIf multiple surgical techniques are offered, how should I choose?
A
The choice of surgical technique is determined by comprehensively evaluating refractive error, corneal shape, lifestyle, age, etc. Generally, SMILE is suitable for mild to moderate myopia when dry eye is a concern. For high myopia (over −10 D), phakic IOL is considered. PRK has the lowest risk of ectasia and is also chosen for thin corneas or re-treatment. In a second opinion, a third party can verify whether the rationale for the proposed technique (residual corneal thickness, PTA, BAD-D value, etc.) is appropriate.
The corneal stroma is ablated using an excimer laser (193 nm wavelength) to alter the corneal curvature. For myopia correction, the central cornea is flattened; for astigmatism correction, asymmetric ablation is performed. LASIK and PRK access the surface, while SMILE removes a lenticule through a cap, preserving the anterior corneal structure. The impact on biomechanical strength is greatest for LASIK, followed by PRK and SMILE.
This method involves inserting an additional lens in front of the crystalline lens to add refractive power to the optical system. Since the cornea is not ablated, its shape is preserved. However, the presence of a foreign body in the anterior chamber carries long-term risks of decreased corneal endothelial cell density, intraocular pressure fluctuations, and cataract formation.
Postoperative corneal ectasia is predisposed by a reduction in the biomechanical strength of the corneal stroma due to ablation and removal. The risk increases when the residual stromal bed is insufficient (RSB <250 μm) or when surgery is performed in the presence of subclinical keratoconus3). The minimum progression criteria for ectasia are documented as at least two of the following: steepening of the anterior surface, steepening of the posterior surface, and thinning 3).
Since PRK and SMILE do not create a flap, applying the LASIK-based PTA calculation directly to SMILE may overestimate the risk of ectasia2).
Enhancement surgery after LASIK (flap lift) has been reported to have a high incidence of epithelial ingrowth, approximately 32% 5). In a case of rapidly progressive epithelial ingrowth on the first day after enhancement surgery, corneal topography showed a temporal increase in anterior elevation difference in the inferonasal quadrant and corneal thickening in the same area, with irregular oblique astigmatism increasing from 0.6 D on day 1 to 2.0 D on day 5 5).
Nomogram adjustment directly affects the accuracy and predictability of laser surgery 2). The preoperative spherical equivalent is the most important adjustment factor, and age, eye laterality, corneal curvature, corneal diameter, and corneal biomechanical properties are also relevant. Personalized adjustment using artificial intelligence (AI) is attracting attention, and is expected to achieve higher accuracy than conventional multivariate regression analysis 2).
In a prospective study by Rush et al., topography-guided LASIK (TG-LASIK) using Phorcides analysis software improved the overall visual satisfaction index on the PROWL questionnaire from 4.07 preoperatively to 5.00 (maximum) postoperatively, with 100% of patients reporting the highest postoperative satisfaction 4). Binocular uncorrected visual acuity was 20/16 or better in 100% of patients at 26 weeks 4). Significant improvements were observed in all measures of night vision, glare, halos, and dry eye symptoms 4).
Patients with low corneal stiffness have been reported to have a 2- to 3-fold higher risk of residual refractive error after KLEx 2). Combining biomechanical indices with topographic parameters has been reported to improve the prediction accuracy of KLEx by more than 25% 2).
Corneal densitometry using a Scheimpflug camera is a technique that objectively measures corneal transparency on a scale of 0 to 100 GSU (gray scale units). A prospective study by Balparda et al. (110 eyes) showed excellent reproducibility in areas up to 10 mm, and changes of 1.0 GSU or more can be judged as clinically significant transparency changes 6). It may be useful for quantitative evaluation of corneal haze after PRK 6).
Ang M, Gatinel D, Reinstein DZ, et al. Evidence-based guidelines for keratorefractive lenticule extraction. Ophthalmology. 2025;132(4):404-418.
Jhanji V, Ahmad S, Amescua G, et al. Corneal Ectasia Preferred Practice Pattern. Ophthalmology. 2024 Apr;131(4):P205-P246. doi:10.1016/j.ophtha.2023.12.038. PMID:38349299.
Rush SW, Pickett CJ, Wilson BJ, Rush RB. Topography-guided LASIK: a prospective study evaluating patient-reported outcomes. Clin Ophthalmol. 2023;17:2815-2824.
Li X, Gu Y. Unusual visual impairment after enhancement refractive surgery. Journal of surgical case reports. 2024;2024(2):rjae074. doi:10.1093/jscr/rjae074. PMID:38370587; PMCID:PMC10873836.
Balparda K, Mesa-Mesa S, Maya-Naranjo MI, Mora-Sánchez C, Escobar-Giraldo M. Determination of the repeatability of corneal densitometry as measured with a Scheimpflug camera device in refractive surgery candidates. Indian journal of ophthalmology. 2023;71(1):63-68. doi:10.4103/ijo.IJO_1121_22. PMID:36588209; PMCID:PMC10155537.
Santhiago MR, Smadja D, Gomes BF, et al. Association between the percent tissue altered and post-laser in situ keratomileusis ectasia in eyes with normal preoperative topography. Am J Ophthalmol. 2014;158(1):87-95.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.


{kind=link}
{kind=link}