For cases where glasses or contact lenses are insufficient, LASIK is considered as a refractive surgery option 2). Other techniques include PRK, relaxing incisions, and wedge resection, but LASIK shows the highest efficacy and lowest complication rate 1,2). In a long-term analysis by Hardten et al. (2002), among 57 eyes, mean UCVA at final follow-up was 20/30, mean SE −0.35 D, and mean residual astigmatism 1.06 D 1). However, complications such as epithelial ingrowth (16%) and regraft (9%) were more frequent than in routine LASIK 1).
QWhen can LASIK be performed after corneal transplantation?
A
There is no consensus on the optimal interval between corneal transplantation and LASIK. Most studies recommend waiting at least 12 months after transplantation. It is generally agreed to allow a stable period of 3–6 months after suture removal. Some recommend a longer interval of 2–3 years after transplantation. The prerequisite is confirmed refractive and structural stability of the graft.
Refractive instability after penetrating keratoplasty is very common. High regular and irregular astigmatism are frequently observed. After combined penetrating keratoplasty and cataract extraction (triple procedure), only 39% of patients achieved within 2 D of emmetropia. The range of postoperative refractive error is -9.75 to +12.88 D.
Refractive errors after penetrating keratoplasty result from inhomogeneities in curvature, thickness, and suture tension between the graft and host cornea. Remodeling during the graft healing process is the main cause of refractive fluctuations.
Contraindications (risk factors) for LASIK after corneal transplant include peripheral corneal neovascularization, thinning of host tissue, wound ectasia, graft override, and graft-host mismatch. Corneal thickness less than 500 μm is also a contraindication for LASIK.
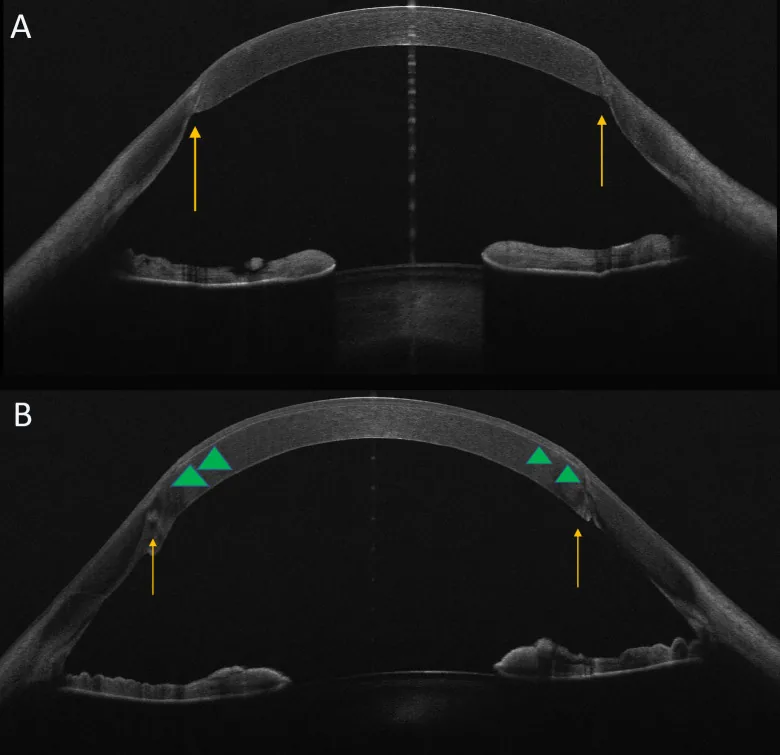
Mucciolo DP, Albani G, Terracciano L, Branchetti M, et al. Femtosecond laser-assisted in situ keratomileusis for the correction of residual ametropia after penetrating keratoplasty: 1-year follow-up. Front Ophthalmol (Lausanne). 2025 Apr 11;5:1562555. Figure 1. PMCID: PMC12022508. License: CC BY.
Cross-sectional image of the anterior segment OCT shows the LASIK flap interface and intrastromal incision plane within the grafted cornea. It allows confirmation of the depth at which the flap is formed relative to the post-transplant cornea.
Preoperative Evaluation Items
Corneal thickness measurement: Evaluate corneal thickness at the center and on both sides of the graft. A minimum of 500 μm is required.
Corneal endothelial cell count: Measure as much as possible to confirm endothelial function.
Corneal topography: Evaluate the distribution and degree of irregular astigmatism using videokeratography. If irregular astigmatism is present, wavefront-guided LASIK may be indicated.
Systemic and Ocular Complication Assessment
History of graft rejection: If present, consider the risk of recurrence after LASIK.
History of ocular herpes: Surgery may reactivate the virus.
Dry eye and blepharitis: Must be fully controlled before surgery.
Intraocular pressure: Exclude elevated intraocular pressure by applanation tonometry.
Glasses are indicated for cases with anisometropia less than 3.0 D and astigmatism less than 4.0 D. Contact lenses are the first choice for visual correction after corneal transplantation. They are successful in 80–90% of cases. Soft contact lenses are chosen for mild regular astigmatism, rigid gas permeable (RGP) lenses for irregular astigmatism, and scleral contact lenses for severe cases.
LASIK can correct spherical error and astigmatism simultaneously. In recent years, flap creation using a femtosecond laser has become common. Wavefront-guided LASIK is useful for correcting irregular astigmatism and is also indicated for cases of irregular astigmatism that cannot be corrected by arcuate keratotomy for Acanthamoeba keratitis or limbal relaxing incisions (LRI).
In the two-step method, topography is followed for several months after flap creation, and laser ablation is performed after confirming stability. Although vector analysis shows good results, there is no significant difference in final visual acuity compared to the one-step method, and the waiting period is long.
Effect: Effective for improving spherical error and astigmatism.
Disadvantages: The main problem is increased corneal haze. Patients after corneal transplantation are more prone to develop severe corneal haze than the general population. Even with mitomycin C (MMC), results are inferior to LASIK.
Indications: It may be chosen in special situations where the LASIK flap is prone to dislocation (e.g., contact sports).
Relaxing Incision / Wedge Resection
Effect: Effective for correcting astigmatism, but cannot address spherical error.
Disadvantages: High incidence of wound dehiscence and unstable wound healing.
Limbal Relaxing Incision (LRI): A relaxing incision is made along the steep meridian to flatten the cornea. A diamond knife or femtosecond laser is used.
QWhich is better, LASIK or PRK?
A
For refractive correction after corneal transplantation, LASIK shows better outcomes than PRK. A major problem with PRK is increased corneal haze, with a tendency for best corrected visual acuity to decrease by at least one line. Haze cannot be completely suppressed even with mitomycin C. LASIK results in less postoperative pain and faster visual recovery. However, PRK may be chosen if corneal thickness is insufficient.
QWill uncorrected visual acuity recover?
A
The main goal of LASIK after corneal transplantation is to reduce refractive error to a level correctable with glasses or contact lenses. Improvement in uncorrected visual acuity is a secondary goal and not always achievable. At 5-year follow-up, 86–98% of eyes achieve best corrected visual acuity of 20/40 or better. However, significant regression may occur, and reoperation rates are reported to be 9.1–51.6%.
Refractive errors after penetrating keratoplasty result from multiple factors. Differences in curvature between the graft and host cornea, uneven tension from sutures, and remodeling during wound healing produce astigmatism and spherical errors. Refractive fluctuations may continue even after suture removal.
Flap creation in LASIK itself alters corneal biomechanics. It may affect the structural stability of the host-graft interface, so in the two-step procedure, it is recommended to confirm stability after flap creation before performing laser ablation.
Because the corneal epithelium is not removed as a sheet, LASIK results in minimal postoperative pain and rapid visual recovery. Transection of corneal sensory nerves during flap creation causes transient dry eye, which improves over time. A residual corneal thickness of at least 250 μm must be ensured.
The introduction of femtosecond lasers has improved the precision and safety of flap creation. Compared to microkeratomes, the incision line and depth are more stable, offering better quantifiability. In cases with corneal opacity, use of a microkeratome or selection of PRK may be necessary.
The widespread use of wavefront-guided LASIK has made it possible to measure preoperative higher-order aberrations and reflect them in the laser ablation design. This is also useful for cases of irregular astigmatism that could not be corrected with conventional methods such as for Acanthamoeba keratitis or LRI.
Among refractive surgeries after corneal transplantation, LASIK shows the highest efficacy and the lowest complication rate. However, because the risk of complications is higher than in standard LASIK, careful patient selection and thorough preoperative evaluation are essential.
SMILE (small incision lenticule extraction), which preserves the corneal epithelium and does not create a flap, is being increasingly adopted, and its application for refractive correction after corneal transplantation may become a future challenge.
Hardten DR, Chittcharus A, Lindstrom RL. Long-term analysis of LASIK for the correction of refractive errors after penetrating keratoplasty. Transactions of the American Ophthalmological Society. 2002;100:143-50; discussion 150-2. PMID:12545688; PMCID:PMC1358957.
Buzard K, Febbraro JL, Fundingsland BR. Laser in situ keratomileusis for the correction of residual ametropia after penetrating keratoplasty. J Cataract Refract Surg. 2004;30(5):1006-1013.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.