Patients who do not achieve the expected visual improvement after LASIK (laser in situ keratomileusis) or experience a decrease in visual quality (QOV) are commonly referred to as “LASIK refugees.” This term is not an academic definition but a Japanese-specific expression describing the reality of patients seeking relief at other facilities.
Overcorrection refers to a state in which myopic LASIK results in excessive correction toward hyperopia. The main problems are eye strain, headaches, and difficulty with near vision during near work (reading, computer work). In presbyopic age, distance vision may be good, but impairment of intermediate and near vision becomes prominent, significantly affecting the patient’s QOL.
The Guidelines for Refractive Surgery (8th edition) set the following basic policies 1).
The goal is that postoperative refraction should not become overcorrected, including in the future.
The amount of myopia correction is generally 6D, up to 10D with adequate informed consent.
Ensure residual corneal thickness of 250 μm or more.
For myopia within 3D, fully explain the disadvantage of decreased near vision at presbyopic age before surgery.
Decreased QOV is not only due to overcorrection. Increased higher-order aberrations (halo, glare, starburst), dry eye (decreased tear production due to corneal nerve transection), irregular astigmatism (decentered ablation, flap striae), and DLK (diffuse lamellar keratitis) are also important causes. Dry eye improves in many cases within 3–6 months postoperatively, but persists in some.
QWhat is a LASIK refugee?
A
“LASIK refugee” is a Japanese colloquial term referring to patients who do not achieve satisfactory visual function after LASIK and seek relief at other facilities. Overcorrection (hyperopic shift), dry eye, increased higher-order aberrations, irregular astigmatism, and corneal ectasia may overlap. It is important to identify the cause through detailed examination at a specialized facility and to perform stepwise management.
Optical zone diameter < scotopic pupil diameter → increased spherical aberration. With a 7 mm optical zone, correction of 3.50 D shows almost no increase in higher-order aberrations
Decentered ablation → coma aberration
Dry eye: Decreased tear secretion due to corneal nerve transection
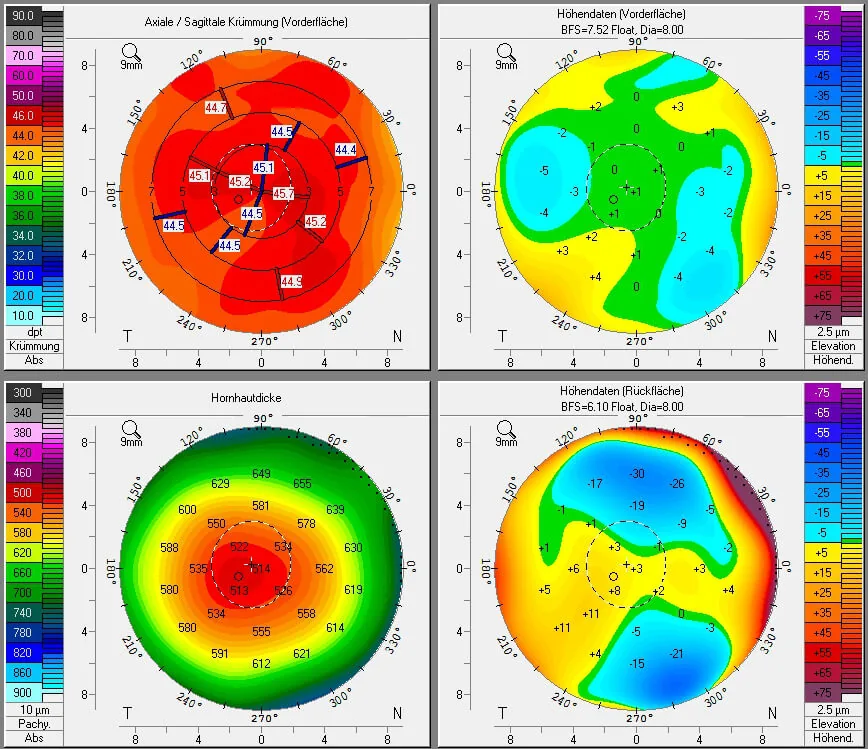
A four-panel topography image taken with Pentacam before LASIK, displaying the anterior corneal curvature map, anterior and posterior elevation difference map, and corneal thickness distribution map on one screen. This corresponds to the topographic evaluation that forms the basis for the ectasia screening indices (BAD-D, PTA) discussed in the section “Diagnosis and examination methods”.
The Munnerlyn formula t = S²D / 3 (t: ablation depth [μm], S: optical zone diameter [mm], D: spherical equivalent) is used to calculate ablation depth, and the residual stromal bed (RSB) is confirmed as RSB = CCT − ablation depth − flap thickness. A minimum of 250 μm must be ensured1).
Differentiation from CL warpage: Epithelial thickening with normal corneal thickness distinguishes from ectasia
QCan overcorrection occur even years after surgery?
A
Yes, it can. Even if LASIK performed at a young age achieved appropriate correction, age-related hyperopic shift may manifest as overcorrection in the 40s to 50s or later. Particularly in cases of myopic correction within 3D, significant decline in near vision becomes problematic when reaching presbyopic age. Therefore, preoperative explanation is important, and regular postoperative refractive examinations are recommended.
Enhancement surgery, which involves additional excimer laser ablation after flap lift, is performed after confirming that the refractive state is non-progressive and that the residual corneal thickness is sufficient 1). Li & Gu reported rapidly progressive epithelial ingrowth from the first day after enhancement surgery, with corneal topography showing increased anterior elevation difference in the inferonasal quadrant and corneal thickening in the same area. Irregular astigmatism increased from 0.6 D on day 1 to 2.0 D on day 5 6).
TG-LASIK is a procedure that reduces higher-order aberrations through customized ablation based on corneal topography data. In a prospective study by Rush et al., TG-LASIK using Phorcides analysis showed improvement in the overall visual satisfaction index on the PROWL questionnaire from 4.07 preoperatively to 5.00 (maximum) postoperatively, with all patients reporting the highest satisfaction 5). Significant postoperative improvements were observed in night vision, glare, halos, and dry eye symptoms 5).
SMILE (KLEx: keratorefractive lenticule extraction) does not create a flap, thus avoiding flap-related complications (flap striae, epithelial ingrowth, free cap) 2). In KLEx, the cap preserves the anterior Bowman’s layer side structure and maintains biomechanical strength, so the risk of ectasia is considered lower than with LASIK 2). A planning protocol maintaining a minimum RST of 220 μm and total uncut stromal thickness of 300 μm has been reported 2).
QIs reoperation possible for overcorrection?
A
If conditions are met, enhancement surgery or additional correction with PRK is possible. However, all of the following conditions must be satisfied: ① refractive stability for at least 6 months postoperatively, ② sufficient residual corneal thickness (minimum 250 μm), ③ no progression of ectasia, and ④ ectasia risk indicators (BAD-D, PTA, etc.) within acceptable range. Epithelial ingrowth has been reported at a high frequency of 32% with flap-lift enhancement, requiring careful management by an experienced surgeon.
The excimer laser ablates the corneal stroma with 193 nm ultraviolet pulses, and the ablation depth is estimated by the Munnerlyn formula t = S²D/3. Overcorrection occurs when the ablation amount exceeds the target value, or when the ablative effect increases during the corneal wound healing process. As a result, excessive flattening of the anterior cornea occurs, reducing myopic refractive power and causing hyperopia.
In LASIK, flap creation cuts the lamellar structure of the cornea. This alters the biomechanical strength of the cornea, creating a risk of postoperative anterior corneal protrusion (ectasia). Femtosecond laser flaps (100–120 μm) are more uniform and thinner than mechanical microkeratome flaps (average 120 μm, with variability), which is advantageous for preserving residual stromal bed (RSB).
PRK does not create a corneal flap, resulting in a thicker residual stromal bed than LASIK. This provides a biomechanical advantage and lower risk of ectasia. However, because Bowman’s layer is ablated, there is a risk of postoperative corneal haze. Prophylactic use of MMC suppresses corneal haze.
In KLEx, the cap preserves the anterior structure (Bowman’s layer side). Because the anterior lamellae remain continuous, the cornea’s pressure resistance is higher than in LASIK. It has been reported that patients with low corneal stiffness have a 2–3 times higher risk of residual refractive error after KLEx2), and preoperative biomechanical evaluation contributes to improving the accuracy of surgical planning.
In corneal ectasia, the epithelium thins over the area of stromal protrusion and forms an epithelial doughnut pattern around it. This epithelial remodeling may lead to underestimation of the degree of ectasia by topography alone. Adding epithelial thickness mapping (AS-OCT) improves the accuracy of differentiating ectasia from CL warpage.
Machine learning algorithms applied to topography and tomography analysis are improving the accuracy of ectasia detection. AI has been reported to achieve results approaching those of corneal specialists in distinguishing normal corneas, suspicious irregular corneas, and keratoconus.
Patients with low corneal stiffness have a 2–3 times higher risk of residual refractive error after KLEx2). Combining biomechanical indices with topographic parameters has been reported to improve the predictive accuracy of KLEx by more than 25%2). Preoperative evaluation using Corvis ST and Ocular Response Analyzer is being utilized for personalized surgical planning.
Nomogram adjustment is directly linked to the accuracy and predictability of laser surgery. Preoperative spherical equivalent is the most important factor, with age, eye laterality, corneal curvature, corneal diameter, and corneal biomechanical properties also being relevant 2). Research on multivariate regression analysis and AI-based personalized adjustment is advancing.
Corneal densitometry using a Scheimpflug camera is an objective method for measuring corneal transparency 4). A prospective study by Balparda et al. (110 eyes) showed excellent reproducibility in areas up to 10 mm, and changes of 1.0 GSU or more can be considered true changes in transparency 4). It may be useful for quantitative evaluation of corneal haze after PRK.
Ang M, Gatinel D, Reinstein DZ, et al. Evidence-based guidelines for keratorefractive lenticule extraction. Ophthalmology. 2025;132(4):404-418.
Jhanji V, Ahmad S, Amescua G, et al. Corneal Ectasia Preferred Practice Pattern. Ophthalmology. 2024 Apr;131(4):P205-P246. doi:10.1016/j.ophtha.2023.12.038. PMID:38349299.
Balparda K, Mesa-Mesa S, Maya-Naranjo MI, Mora-Sánchez C, Escobar-Giraldo M. Determination of the repeatability of corneal densitometry as measured with a Scheimpflug camera device in refractive surgery candidates. Indian journal of ophthalmology. 2023;71(1):63-68. doi:10.4103/ijo.IJO_1121_22. PMID:36588209; PMCID:PMC10155537.
Rush SW, Pickett CJ, Wilson BJ, Rush RB. Topography-guided LASIK: a prospective study evaluating patient-reported outcomes. Clin Ophthalmol. 2023;17:2815-2824.
Li X, Gu Y. Unusual visual impairment after enhancement refractive surgery. Journal of surgical case reports. 2024;2024(2):rjae074. doi:10.1093/jscr/rjae074. PMID:38370587; PMCID:PMC10873836.
Santhiago MR, Smadja D, Gomes BF, et al. Association between the percent tissue altered and post-laser in situ keratomileusis ectasia in eyes with normal preoperative topography. Am J Ophthalmol. 2014;158(1):87-95.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.

{kind=link}