Radial keratotomy (RK) is a surgical procedure that corrects myopia by making radial incisions in the cornea with a diamond knife, sparing the pupillary zone, down to near Descemet’s membrane, thereby flattening the cornea. It was introduced in the 1970s and performed on hundreds of thousands of patients.
However, problems such as diurnal fluctuation of vision, glare, and progressive hyperopia became apparent, and RK has now been largely replaced by excimer laser refractive surgery. According to the PERK (Prospective Evaluation of Radial Keratotomy) study, fewer than 1% of patients experienced decreased visual acuity after RK, but long-term sequelae can continue to affect patients many years after surgery.
In cataract surgery after RK, wound dehiscence and refractive error variability are concerns 1). If the existing radial incisions intersect with the cataract surgery incision, wound dehiscence, delayed healing, and irregular astigmatism may occur 1).
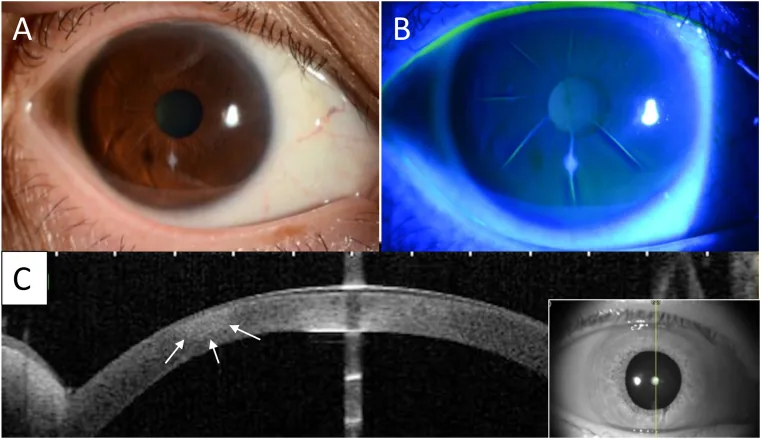
Kawasaki M, Fukuoka H, Kawabata M, et al. A rare case of infectious keratitis that developed 27-years after radial keratotomy. American Journal of Ophthalmology Case Reports. 2021 Dec 7; 25:101240. Figure 3. PMCID: PMC8665298. License: CC BY.
Slit-lamp image, fluorescein staining, and anterior segment OCT are shown side by side, demonstrating the separation of radial keratotomy incisions and changes in the shape of the surrounding cornea. The wound opening, staining area, and cross-sectional irregularity can be seen correspondingly.
Slit-lamp microscopy and various imaging tests reveal the following findings.
Corneal incision scars: Radial incision marks remain on the cornea. The degree of scarring varies greatly among individuals.
Incisional neovascularization: Particularly observed in contact lens wearers when the incision extends to the limbus.
Irregular astigmatism: Caused by uneven incision depth, asymmetric incision placement, and optical zone decentration.
Corneal topographic abnormalities: Irregular corneal shape along the incisions is observed. It is also useful for evaluating shape changes over time.
In the PERK study, at 3 years postoperatively, 58% of eyes were within 1.00 D of emmetropia, while 26% were undercorrected and 16% were overcorrected by more than 1.00 D.
QWhy do diurnal fluctuations occur after RK?
A
After RK, the cornea is structurally weakened by the incisions. During eyelid closure at night, the cornea flattens, and it gradually steepens after waking. This diurnal variation in corneal shape is perceived as changes in refractive error. The fluctuation is greatest within a few hours after waking and tends to stabilize as the day progresses.
Corneal incision sites have reduced strength compared to normal cornea, leading to a higher risk of rupture from direct trauma. High-risk activities without appropriate eye protection should be avoided.
QIs the cornea more vulnerable to trauma after RK?
A
The incision sites in RK have reduced strength compared to normal cornea. Even years after surgery, the incisions do not fully regain original strength, so there is a risk of rupture from direct trauma. Protective eyewear is recommended during sports or hazardous work.
The following examinations are performed to evaluate complications after RK.
Slit-lamp microscopy: Evaluates the condition of the incision, scars, neovascularization, epithelial ingrowth, and infection.
Corneal topography: Quantitatively evaluates corneal shape irregularities and the degree of irregular astigmatism. It is also used to confirm refractive stability before additional surgery.
Refraction test: Both subjective refraction and cycloplegic refraction are performed to assess the degree of overcorrection or undercorrection.
Corneal thickness measurement: Confirms the residual thickness of the corneal stroma. It is essential when considering additional laser surgery.
Intraocular lens power calculation is particularly difficult in cataract surgery after RK 1). This is because it is difficult to determine the true corneal refractive power and predict the effective lens position.
Problem
Details
Overestimation of corneal refractive power
Keratometers measure only the central area, but after RK, the cornea is flat in the center and steep in the periphery.
Specialized formulas such as the Double-K method and Barrett True K formula have been proposed.
When an intraocular lens is inserted with a plano target after RK, hyperopia was observed in 83.4% of cases. Targeting myopia can reduce the frequency of hyperopia to 42.0%, but it cannot be completely eliminated 2).
Glasses and Contact Lenses: The most basic correction method. RGP lenses are effective for irregular astigmatism.
PRK: The most predictable treatment for RK-induced hyperopia and irregular astigmatism. Wavefront-guided PRK is recommended.
Corneal Suturing: Single circumferential suture, double circumferential suture, or square stitches at incisions can stabilize refractive errors.
Management of Other Complications
Corneal Perforation: Microperforations are managed conservatively with cycloplegics, aqueous suppressants, and antibiotics. Large perforations require 10-0 nylon sutures.
Infectious Keratitis: Common causative organisms include Pseudomonas aeruginosa, Staphylococcus aureus, and Staphylococcus epidermidis. Treat with antibiotics based on sensitivity.
The cataract surgery incision should be placed to avoid crossing existing radial incisions 1). A short scleral incision is advantageous to avoid crossing radial incisions 1). Postoperative corneal edema and elevated intraocular pressure can amplify the effect of RK incisions, causing transient hyperopia and astigmatic shifts 1). Additional refractive surgery should be delayed until refraction stabilizes 1).
QWhat are the points to note in cataract surgery after RK?
A
In cataract surgery after RK, it is important to (1) avoid intersecting existing radial incisions, (2) use a dedicated intraocular lens power calculation formula, and (3) set a myopic target (to prevent hyperopic shift) 1)2). Postoperatively, it may take several weeks or more for the refractive value to stabilize, and the decision for additional surgery should be made carefully.
QIs LASIK indicated for hyperopic shift after RK?
A
For hyperopic shift after RK, PRK is recommended over LASIK. This is because creating a LASIK flap can open the RK incisions, leading to a risk of epithelial ingrowth. Wavefront-guided PRK is considered the most predictable treatment for irregular astigmatism.
In RK, the corneal stroma is incised deeply to near Descemet’s membrane, compromising the structural integrity of the cornea. The incisions heal through wound healing but do not fully restore original strength.
During eyelid closure at night, intraocular pressure rises, causing the weakened incisions to widen and the cornea to flatten. After waking, intraocular pressure decreases, and the cornea gradually steepens. This cycle is perceived as diurnal variation.
Wound healing of corneal incisions progresses over a long period. Remodeling of scar tissue causes the incisions to widen, leading to further flattening of the central cornea. This is thought to be the cause of progressive hyperopic shift. In the PERK study, changes toward hyperopia continued even 10 years after surgery.
Early postoperative infection is due to bacterial invasion through the surgical wound, but late-onset infection (1-3 years after surgery) has also been reported. Delayed wound healing after RK is considered a predisposing factor for late-onset infection. It shows a characteristic distribution pattern with infiltration within the corneal incisions.
Miller KM, Oetting TA, Tweeten JP, Carter K, Lee BS, Lin S, et al. Cataract in the Adult Eye Preferred Practice Pattern. Ophthalmology. 2022;129(1):P1-P126. doi:10.1016/j.ophtha.2021.10.006. PMID:34780842.
European Society of Cataract and Refractive Surgeons (ESCRS). ESCRS Cataract Surgery Guideline. 2024.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.