A phakic intraocular lens (phakic IOL) is a refractive lens inserted into the eye while preserving the natural lens. Since it does not ablate the cornea, it preserves corneal biomechanics and can correct high myopia. Its reversibility is also a notable advantage.
Phakic IOLs are classified into three types based on the fixation site.
Anterior chamber angle-supported
Representative example: AcrySof (Alcon) etc.
Design with support in the anterior chamber angle. Chronic corneal endothelial cell loss, pupil ovalization, and nuclear cataract were issues, and it has now been withdrawn from the market. Not recommended for refractive correction in young patients.
Iris-fixated
Artisan/Verisyse (Ophtec/Abbott): Fixed with claws to the mid-peripheral iris.
There is also a foldable version, Artiflex/Veriflex (polysilicone material). Models for myopia, astigmatism, and hyperopia are available. A large incision is required, and postoperative astigmatism must be considered. Chronic corneal endothelial cell loss is a concern, but it is safer than the angle-supported type 9).
Posterior chamber (ICL)
Visian ICL (STAAR Surgical): Placed in the ciliary sulcus behind the iris and in front of the crystalline lens.
Can be inserted through a 3.0 mm small incision. EVO/EVO+ (with central hole) is currently the mainstream, with the most abundant evidence of safety and efficacy. It is located away from the corneal endothelium, so the risk of endothelial cell loss is low.
In 1986, Fyodorov first reported the anterior chamber type. STAAR Surgical began development of the posterior chamber ICL in 1993, and it received FDA approval in the United States in 2005. In Japan, it was approved in 2010, and the EVO ICL (with central hole KS-AquaPORT) was approved in 2014. In March 2022, EVO/EVO+ received FDA approval, and over 2 million lenses have been used worldwide 1).
The latest EVO ICL features a central port (KS-Aquaport) with a diameter of 0.36 mm. This has brought the following advantages:
Eliminates the need for Nd:YAG laser iridotomy required in previous models
Maintains physiological aqueous humor circulation
Reduces the incidence of anterior subcapsular cataract and pupillary block
QCan a phakic IOL be removed in the future?
A
Reversibility (explantability) is one of the greatest advantages of phakic IOLs. If a cataract develops, the phakic IOL can be removed, cataract surgery performed, and a standard intraocular lens implanted. Since there is no effect on the cornea, it does not interfere with IOL power calculation for future cataract surgery1).
Patient Selection and Preoperative Counseling for Phakic IOL
Proper patient selection and informed consent are key to the success of phakic IOL surgery. The Refractive Surgery Guidelines (8th edition) emphasize the importance of informed consent before the procedure6), and the following points must be explained:
There are uncertainties regarding the long-term prognosis of refractive surgery
It is an intraocular surgery that invades the normal anterior segment of the eye
The existence of other correction methods such as glasses and contact lenses
Disadvantages of myopia within 3D when reaching presbyopic age
When visiting a doctor for other diseases after surgery, inform the attending physician of the history of this surgery
Indications are determined after comprehensive evaluation of the patient’s occupation, lifestyle, degree of myopia, corneal shape, and general condition.
Relationship between phakic IOL and myopia management
Phakic IOL is a surgery for correcting myopia in adults and does not suppress myopia progression. It is not indicated for progressive myopia (during growth period). In Japan, the ideal flow is to suppress myopia progression in childhood with myopia control glasses (MiYOSMART®, Stellest®), low-dose atropine eye drops, orthokeratology, etc., and then consider phakic IOL in adulthood after correction stabilizes.
Phakic IOL surgery is not a one-time procedure; it requires lifelong continuous follow-up. The Refractive Surgery Guidelines (8th edition) recommend regular postoperative observation6).
Vault tends to decrease over the years due to age-related swelling of the crystalline lens. In particular, after age 40, vault decreases due to increased lens thickness, so enhanced follow-up is recommended 8). Corneal endothelial cells are relatively stable with posterior chamber ICL, but chronic decrease can occur with anterior chamber types, so continuous measurement is necessary 9).
Early postoperative period (within 1 month): Do not rub the eyes vigorously. Avoid swimming in the sea or using pools (infection risk). Sports (especially contact sports) are restricted for 1 month after surgery.
Dry eye care: Phakic IOL has a lower risk of dry eye than LASIK because corneal nerves are preserved, but temporary dryness may occur after surgery. Use of artificial tears is effective.
Importance of regular check-ups: Regular check-ups 1–2 times a year are necessary throughout life to monitor changes in vault over time and corneal endothelial cells 6).
Pregnancy and childbirth: Attention to refractive changes during pregnancy is necessary. If the change in prescription is significant, consult a specialist.
Future cataract surgery: After ICL removal, standard cataract surgery is possible. Since corneal data remain accurate, IOL calculation is not affected (an advantage over LASIK).
Phakic IOL surgery is not covered by insurance (private practice) in Japan. The cost is often around 500,000 to 700,000 yen for both eyes (varies by facility and lens used). It may be eligible for medical expense deductions (check the latest National Tax Agency notice on whether IC IOL surgery for refractive correction qualifies). Surgery for visual function recovery (e.g., keratoconus) may be covered by insurance, so confirm that it can be covered for indicated conditions.
Role of Refractive Surgery in the Era of Myopia Epidemic
Against the backdrop of the global myopia epidemic, demand for refractive surgery including phakic IOL is expected to increase. A “two-stage approach” is considered ideal: after controlling myopia progression in childhood (with myopia control glasses, orthokeratology, atropine eye drops, etc.), once the prescription stabilizes in adulthood, phakic IOL or corneal refractive surgery can be chosen. In high myopia, there is a risk of retinal complications (tears, detachment, myopic maculopathy), so preoperative and postoperative fundus management is essential. The goal of modern refractive medicine is to optimally combine glasses, contact lenses, and refractive surgery according to the patient’s needs, eye condition, and lifestyle.
Based on US FDA approval, the indications for Visian ICL are age 21-45 years, spectacle refraction of -3.0D to -20.0D, and anterior chamber depth of 3.0mm or more1).
For moderate myopia with a correction amount less than 6D, corneal refractive surgery (LASIK/SMILE) is a common option. For high myopia of 6D or more or cases with insufficient corneal thickness, phakic IOL is advantageous.
Because corneal biomechanics can be preserved, it is said to cause less biomechanical change compared to LASIK and SMILE7). This is an important advantage that helps avoid the risk of post-refractive ectasia.
QWhich is better, LASIK or this?
A
The choice depends on the amount of correction, corneal thickness, and age. For moderate myopia less than 6D, corneal refractive surgery is widely chosen. For high myopia of 6D or more, or when the cornea is thin, phakic IOL is advantageous. Phakic IOL preserves corneal biomechanics, so it is said to cause less biomechanical change than LASIK 7). There is also no risk of dry eye or corneal ectasia1).
Measurement of anterior chamber depth and sulcus-to-sulcus diameter
Horizontal corneal diameter (white-to-white; WTW) is an essential parameter for ICL size determination. Direct measurement of the sulcus-to-sulcus (STS) diameter using anterior segment OCT or UBM provides better vault prediction accuracy than WTW nomogram alone and is recommended 11). ICL sizes include 13.2 mm, 13.7 mm, 14.0 mm, and 14.5 mm; appropriate size selection is key to vault management.
Power calculation for iris-fixated (Artisan) IOL: Use the Van der Heijde nomogram to calculate power from refractive value, corneal power, and anterior chamber depth 9).
Since the EVO ICL has a central hole, peripheral iridotomy is not required. In the conventional model (without central hole), Nd:YAG laser iridotomy was performed at two superior sites 2-3 weeks before surgery 1).
The ideal central vault (the gap between the ICL and the anterior lens surface) is 250–750 μm 2).
Vault <250 μm: Risk of anterior subcapsular cataract formation due to contact with the crystalline lens
Vault >750 μm: Risk of angle narrowing and pupillary block due to anterior iris displacement
Sun Y, Li X, Sun H, et al. The long-term observation of the rotation of implantable collamer lens as the management of high postoperative vault. Front Med (Lausanne). 2023;10:1104047. Figure 2. PMCID: PMC9995363. License: CC BY.
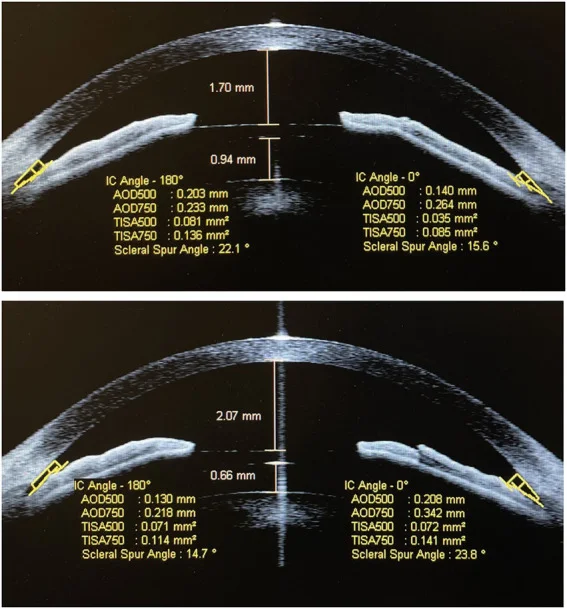
Horizontal section image of anterior segment OCT (CASIA) showing the vault (distance from the posterior ICL surface to the anterior lens surface) and anterior chamber depth (ACD) indicated by yellow measurement lines. This corresponds to the postoperative management of vault (250–750 μm) discussed in section “4. Surgical Technique.”
If an abnormal vault is detected, ICL size change or exchange is required.
QCan surgery be performed on both eyes at the same time?
A
Simultaneous bilateral surgery is possible. However, in cases deemed to have a high infection risk, it is preferable to perform surgery on one eye at a time 6). Because transient intraocular pressure elevation may occur postoperatively, observation for at least 2 hours on the day of surgery is recommended.
An overview of postoperative complications is shown below 6). The mean corneal endothelial cell loss rate at 6 months for EVO ICL is 2.2% 1), and at 8-year follow-up it stabilizes at 3.6 ± 7.9% 8).
Summary of long-term outcomes:
UDVA 20/20 or better achievement rate: 94.5% at 6 months in EVO ICL FDA trial1)
Within ±0.50D: 91.5%1)
CDVA maintenance rate: 98.0%, safety index 1.211)
Long-term stability has been reported in 5-year follow-up of Toric ICL (simultaneous correction of myopia and astigmatism)10)
Preoperative retinal examination / prophylactic photocoagulation if needed
Photopsia
Originating from iridotomy/iridectomy site
Reduced with EVO ICL
The mean corneal endothelial cell loss rate at 6 months after EVO ICL implantation was 2.2% 1). At 8-year follow-up, the loss rate stabilized at 3.6 ± 7.9% 1).
According to the guidelines (8th edition), visual acuity, refraction, vault, corneal endothelial cell density, intraocular pressure, and fundus should be checked at 1 day, 1 week, 1 month, 3 months, and 6 months postoperatively, and then every 6 to 12 months for life 6). Since the vault value tends to decrease over time due to age-related thickening of the lens, special attention is needed after age 40.
Differential Diagnosis and Management of Elevated Intraocular Pressure
Li et al. (2023) reported two cases of delayed TASS occurring one week after phakic IOL surgery 3). Keratic precipitates on the corneal endothelium and fibrin formation in the anterior chamber were observed, but improved with systemic and topical steroid therapy (prednisolone 0.5 mg/kg orally + 1% eye drops every hour) for 4-5 weeks. The incidence was 0.24% (2 out of 827 eyes).
Zheng et al. (2023) reported a case of Staphylococcus epidermidisendophthalmitis occurring 20 days after phakic IOL surgery 4). Intravitreal injections (vancomycin 1 mg + ceftazidime 2 mg) were administered twice, and visual acuity recovered to 22/20 without ICL removal or vitrectomy. The incidence is estimated at approximately 0.017-0.036%.
Collamer has extremely high biocompatibility. Examinations using specular microscopy and laser flare cell meter have confirmed the absence of inflammatory reactions 1). Due to its collagen content, it has high affinity with biological tissues and excellent permeability to gases and metabolites.
Physical properties of Collamer:
Refractive index: 1.452 (close to normal aqueous humor and biological tissues)
Water content: approximately 36% (provides high flexibility and moderate mechanical strength)
Oxygen permeability: Relatively high Dk value, expected to provide metabolic support to avascular tissue (anterior lens surface)
UV absorption: Blocks UV below 360 nm via 3.8% benzophenone
The optic zone of the ICL is positioned in an arch above the crystalline lens. Proper maintenance of the vault between the ICL and the lens allows aqueous humor to flow over the lens surface, preventing cataract formation.
The central port (KS-Aquaport) of the EVO ICL enables physiological aqueous humor flow from the posterior chamber to the anterior chamber. This provides prevention of pupillary block, maintenance of nutrient supply to the lens, and reduction of the risk of anterior subcapsular cataract.
Phakic IOLs do not ablate the cornea, thus preserving corneal biomechanics. Compared to LASIK and SMILE, they are associated with fewer biomechanical changes7). This is an important advantage in avoiding the risk of post-refractive ectasia.
Postoperative changes in corneal biomechanical parameters:
Preservation of corneal biomechanics is an important advantage for preventing future risk of corneal ectasia (post-refractive ectasia) 7). Even if cataract surgery becomes necessary in the future, phakic IOLs allow IOL power calculation to be performed normally because the corneal shape remains unchanged.
Toric ICL (toric implantable collamer lens) can correct both myopia and astigmatism simultaneously. Accurate axis alignment is important because postoperative rotation affects the correction effect 5). In a 5-year follow-up by Alfonso et al., long-term axis stability and good refractive predictability of Toric ICL were confirmed 10). Astigmatism of 1.0 to 4.0 D is the main indication range (Japanese Ophthalmological Society guidelines) 6), and residual astigmatism is likely to occur after surgery for high astigmatism exceeding this range.
An 8-year follow-up study of posterior chamber phakic IOLs confirmed stable long-term predictability of spherical equivalent 8). In addition to the natural annual decrease of 0.5–1.0% in corneal endothelial cell density, phakic IOLs cause an additional decrease (more pronounced with anterior chamber IOLs, mild with posterior chamber IOLs) 9). Vault tends to decrease over time due to age-related lens thickening, so regular vault monitoring is necessary.
The incidence of cataract was approximately 2–5% over 5 years with pre-EVO ICL models, but with EVO ICL, the rate has decreased due to improved vault 1). A 5-year follow-up study also reported long-term efficacy and safety 10).
When cataract surgery is needed after phakic IOL implantation, the ESCRS guidelines recommend checking for iris damage, patency of peripheral iridotomy, and corneal endothelial cell density and morphology in cases of iris-fixated IOLs 12). For posterior chamber ICLs, the ICL is removed first, then standard cataract surgery is performed, and IOL power calculation uses pre-refractive surgery data.
7. Latest research and future perspectives (investigational reports)
Research is underway on a system that uses AI to analyze anterior segment OCT and UBM data to predict optimal vault. It is expected to surpass the accuracy of conventional nomograms (WTW + ACD). Sun et al. (2023) reported improvement in high vault cases by rotating the ICL 90°, reducing mean vault from 1,249 μm to 459 μm 13).
With the global increase in myopia, the demand for phakic IOLs is expected to rise. It is reported that by 2050, 4.9 billion people worldwide will have myopia and 940 million will have high myopia14), increasing the role of phakic IOLs as refractive surgery for high myopia. Packer’s meta-analysis (2016) confirmed that central-hole (EVO) ICLs significantly reduce the risk of anterior subcapsular cataract, angle closure, and pupillary block compared to non-central-hole designs 15).
Toric ICL (simultaneous correction of myopia and astigmatism)
Toric ICL corrects both myopia and astigmatism in a single surgery. Postoperative axis rotation (rotational deviation) is a clinical challenge, but stable long-term results have been reported 10).
An innovative phakic IOL that received CE mark approval in July 2020. It features an aspheric extended depth of focus (EDOF) optical system and provides correction for near and intermediate vision. The target age range is 21-60 years, and it is awaiting FDA approval in the United States 1).
A method called “bioptics,” in which residual refractive errors after ICL insertion are touched up with corneal refractive surgery (LASIK/PRK), is performed at some facilities. Its potential to expand the range of correction for high myopia is being investigated. Phakic IOLs preserve corneal biomechanics and are therefore considered suitable as a preliminary step to corneal refractive surgery.
Research is progressing on systems that analyze anterior segment OCT and UBM data with AI to predict the optimal vault. This is expected to achieve predictive accuracy beyond conventional WTW + ACD nomograms. It is thought that inputting preoperative anterior segment analysis data into machine learning models will enable personalized lens size selection.
Packer M. The EVO implantable collamer lens for moderate myopia: results from the US FDA clinical trial. Clin Ophthalmol. 2022;16:3981-3991.
Moshirfar M, Moin KA, Pandya S, Karimian F, Zaugg B, Khan S, et al. Severe intraocular pressure rise after implantable collamer lens implantation. Journal of cataract and refractive surgery. 2024;50(9):985-989. doi:10.1097/j.jcrs.0000000000001534. PMID:39183446; PMCID:PMC11338031.
Li L, Zhou Q. Late-onset toxic anterior segment syndrome after ICL implantation: two case reports. BMC Ophthalmol. 2023;23:61. doi:10.1186/s12886-022-02713-3.
Zheng K, Zheng X, Gan D, Zhou X. Successful antibiotic management of Staphylococcus epidermidis endophthalmitis after implantable collamer lens implantation. BMC ophthalmology. 2023;23(1):410. doi:10.1186/s12886-023-03127-5. PMID:37828437; PMCID:PMC10568818.
Zhang W, Li F, Zhou J. Anterior Segment Hemorrhage after Implantable Collamer Lens Surgery. Ophthalmology. 2025;132(4):e72. doi:10.1016/j.ophtha.2024.06.015. PMID:39046379. 2023.
Wang Y, Xie L, Yao K, Sekundo W, Alió JL, Mehta JS, Goel S, Elmassry A, Schallhorn J, Shilova T, Cao H, Xu L, Chen X, Zhang F, Bai J, Zhang W, Liu Q, Zhou X, Chen Y, Wang Z, Jhanji V, Yang K, Writing Committee for the Guideline Working Group. Evidence-Based Guidelines for Keratorefractive Lenticule Extraction Surgery. Ophthalmology. 2025;132(4):397-419. doi:10.1016/j.ophtha.2024.11.016. PMID:39577672.
Igarashi A, Shimizu K, Kamiya K. Eight-year follow-up of posterior chamber phakic intraocular lens implantation for moderate to high myopia. American journal of ophthalmology. 2014;157(3):532-9.e1. doi:10.1016/j.ajo.2013.11.006. PMID:24239774.
Kohnen T, Kook D, Morral M, Güell JL. Phakic intraocular lenses: part 2 — results and complications. J Cataract Refract Surg. 2010;36:2168-2194. doi:10.1016/j.jcrs.2010.10.007. PMID:21111322.
Alfonso JF, Baamonde B, Fernández-Vega L, Fernandes P, González-Méijome JM, Montés-Micó R. Posterior chamber collagen copolymer phakic intraocular lenses to correct myopia: five-year follow-up. Journal of cataract and refractive surgery. 2011;37(5):873-80. doi:10.1016/j.jcrs.2010.11.040. PMID:21511154.
Du Y, Jin C, Yin S, Wang G, Ma Q, Li Y, Chen B, Wang H, et al. Comparison of Vault Measurements Using a Swept-Source OCT-Based Optical Biometer and Anterior Segment OCT. Frontiers in medicine. 2022;9:865719. doi:10.3389/fmed.2022.865719. PMID:35814765; PMCID:PMC9259877.
European Society of Cataract and Refractive Surgeons (ESCRS). ESCRS Clinical Guidelines for Cataract Surgery. Brussels: ESCRS; 2024.
Jiang Y, Luo Y, Li Y, Lu T. The long-term observation of the rotation of implantable collamer lens as the management of high postoperative vault. Frontiers in medicine. 2023;10:1104047. doi:10.3389/fmed.2023.1104047. PMID:36910497; PMCID:PMC9995363.
Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036-1042. doi:10.1016/j.ophtha.2016.01.006. PMID:26875007.
Packer M. Meta-analysis and review: effectiveness, safety, and central port design of the intraocular collamer lens. Clinical ophthalmology (Auckland, N.Z.). 2016;10:1059-77. doi:10.2147/OPTH.S111620. PMID:27354760; PMCID:PMC4907705.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.