Eye tumor excision is a general term for surgery to remove tumors arising in eye tissues such as the eyeball, orbit, eyelids, and conjunctiva.
The surgical method varies greatly depending on the tumor’s site of origin, histologic type, and whether it is benign or malignant.
Reconstructive surgery is performed to make up for cosmetic and functional deficits after removal, and includes placement of an ocular prosthetic base, fitting of an artificial eye, eyelid reconstruction, and orbital wall reconstruction.
By combining the two, the goals are tumor control and preserving the patient’s quality of life at the same time.
For orbital tumors, the goal is complete removal, but depending on the tumor’s biological characteristics, adjuvant therapy after biopsy or orbital exenteration may be selected.
The surgical strategy for each disease follows the basic principles of tumor surgery and is determined by combining preoperative imaging and histopathological diagnosis.
Orbital tumor resection involves several approaches depending on the site and pattern of spread.
Anterior approach (anterior approach): Used for tumors located anteriorly or anterolaterally. It provides direct access through the eyelid or conjunctiva and is minimally invasive.
Lateral approach (lateral approach): Indicated for lacrimal gland tumors and intraconal tumors. It is often combined with bone removal of the lateral orbital wall to secure a wide operative field.
Lacrimal sac transection approach: Used for tumors extending into the lacrimal sac and nasolacrimal duct region.
Transcranial approach (transcranial approach): Used for tumors at the orbital apex or extending intracranially. Cooperation with neurosurgery is required.
Transnasal/transantral approach (transnasal/transantral approach): Indicated for tumors adjacent to the medial or inferior orbital wall. It may also be combined with endoscopic sinus surgery.
By combining these approaches, tumors involving the entire orbit can be treated.
QHow is the approach for orbital tumor resection determined?
A
The choice depends on the tumor’s location, size, and the degree of invasion into adjacent structures (bone, intracranial space, and sinuses). Anteriorly located small tumors are treated with an anterior approach, while lacrimal gland tumors and intraconal tumors are better suited to a lateral approach with bone removal. In cases with orbital apex or intracranial extension, a transcranial approach is chosen, and for medial or inferior lesions, a transnasal/transantral approach is selected. A preoperative three-dimensional assessment of tumor extent with CT and MRI is essential.
The main symptoms and clinical findings seen before surgery for orbital tumors are shown below.
The nature of the symptoms varies depending on the tumor’s growth rate, location, and whether it is benign or malignant.
Proptosis: Forward displacement of the eyeball caused by a mass inside the orbit. Benign tumors usually grow slowly, while malignant tumors enlarge quickly.
Eye deviation: The eyeball shifts in the direction of the tumor’s location. For lacrimal gland tumors, a downward and inward deviation is typical.
Detailed preoperative testing is necessary to decide the surgical plan.
CT scan: Evaluates the tumor’s location, bone changes, and calcification. Whether bone invasion is present directly affects the choice of approach.
MRI scan: Evaluates soft tissues and checks for involvement of the optic nerve or spread into the skull. T2-weighted images and contrast-enhanced images are important.
Systemic evaluation (PET/CT, chest and abdominal CT): In suspected malignant tumors, it is necessary to look for distant metastasis and the primary site.
Histopathological examination (biopsy): Confirming the histologic type is essential for deciding the treatment plan. However, if pleomorphic adenoma is suspected, biopsy may be avoided to prevent capsular rupture.
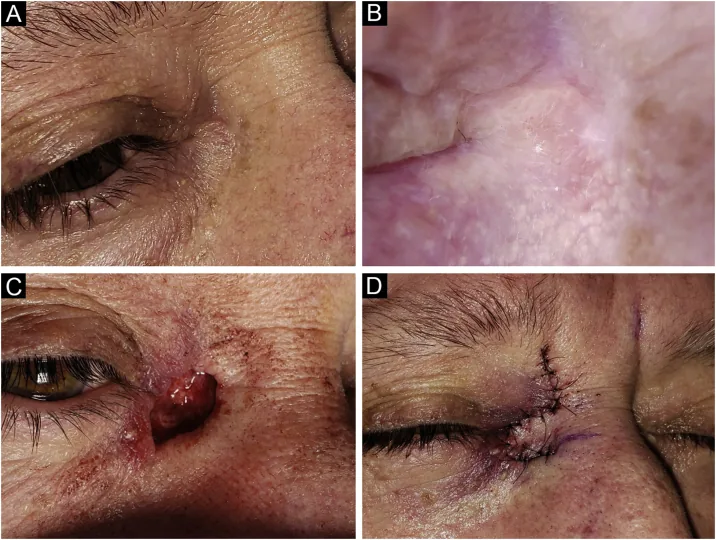
Peirano D, et al. Management of periocular keratinocyte carcinomas with Mohs micrographic surgery and predictors of complex reconstruction. An Bras Dermatol. 2024. Figure 3. PMCID: PMC10943309. License: CC BY 4.0.
A four-panel set of preoperative and immediate postoperative photos showing closure of the defect with a rhomboidal flap after Mohs micrographic surgery confirmed tumor-negative margins in two stages for a small nodular basal cell carcinoma at the medial orbital rim. This corresponds to Mohs surgery and flap reconstruction for eyelid tumors described in the section “Surgical strategy by disease.”
The goals of surgery and the procedure used vary greatly depending on the histologic type of the disease. For skin cancer–type lesions such as eyelid basal cell carcinoma and squamous cell carcinoma, Mohs micrographic surgery is established as the first-choice treatment to reduce recurrence [1,2]. For conjunctival epithelial tumors such as conjunctival intraepithelial neoplasia and squamous cell carcinoma, ocular surface reconstruction with amniotic membrane transplantation after excision and cryotherapy has shown good long-term results [8].
Shown here as a representative example of pleomorphic adenoma of the lacrimal gland.
Complete excision is the rule: Remove the tumor completely in one piece without breaking the capsule.
Importance of the first surgery: If complete removal is not achieved at the first surgery, recurrence or malignant transformation (carcinoma ex pleomorphic adenoma) may occur later.
Lateral approach plus osteotomy: For pleomorphic adenoma of the lacrimal gland, combine a lateral approach with osteoplastic bone removal.
Biopsy and needle biopsy should generally be avoided: Capsular rupture can spread tumor cells into surrounding tissue and greatly increase the recurrence rate [6].
Indications for orbital exenteration (orbital exenteration): Chosen for adenocarcinoma and adenoid cystic carcinoma when complete removal is also difficult and postoperative adjuvant therapy is not expected to be effective.
Postoperative reconstruction: Cosmetic reconstruction of the eyelids and orbit is an important issue.
Benign tumors (pleomorphic adenoma, etc.)
Goal: Complete excision without breaking the capsule
Approach: Lateral approach + osteotomy are common
Contraindication: Biopsy and needle biopsy (risk of capsule rupture)
Prognosis: Good if completely excised at the first surgery
Malignant lymphoma
Goal: confirm the histologic type by biopsy
Approach: diagnostic excision (5 mm³ or more)
Adjuvant treatment: radiotherapy and chemotherapy
Prognosis: depends on the histologic type (MALT type is relatively favorable)
Refractory malignant tumor (adenocarcinoma, etc.)
Goal: local control (curative resection or debulking)
Procedure: orbital exenteration may be indicated
Adjuvant treatment: radiotherapy and carbon ion therapy
Reconstruction: orbital implant, orbital reconstruction, prosthesis
Orbital exenteration is chosen for malignant tumors that are difficult to remove completely and for which postoperative adjuvant treatment is not expected to be effective (adenocarcinoma, adenoid cystic carcinoma, etc.). A systematic review and meta-analysis reported a 5-year overall survival rate of about 50% after this procedure and a weighted mortality rate of about 39%; prognosis is poor for malignant melanoma and adenoid cystic carcinoma of the lacrimal gland, while non-squamous-cell carcinoma-type malignant tumors of the eyelid show relatively better survival [3,4,5].
This is a real intraoperative photo showing an oculoplastic surgeon performing enucleation, with the eyeball being removed in a sterile setting. It corresponds to the surgical procedures for enucleation and orbital exenteration discussed in the section on “Orbital Exenteration and Reconstruction.”
Resection range: The orbital contents, including the eyeball, orbital fat, extraocular muscles, and optic nerve, are removed en bloc.
Eyelid handling: Depending on the extent of tumor spread, the eyelids may be preserved (lid-sparing) or removed (non-lid-sparing).
Periosteal handling: This is divided into periosteum-preserving and periosteum-removing types; with the periosteum-preserving type, postoperative prosthetic socket formation is easier.
Postoperative reconstruction and cosmetic management
Tan JA, Khoo ET, Al-Chalabi MMM, Mohd Zainal H, Wan Sulaiman WA. Orbital Exenteration and Reconstruction Using a Free Radial Forearm Flap in Conjunctival Melanoma: Old but Gold. Cureus. 2023;15(7):e42572. doi:10.7759/cureus.42572. PMID:37637587. PMCID:PMC10460132. Figure 3. License: CC BY 4.
This photo shows the appearance two weeks after orbital exenteration for conjunctival malignant melanoma, with the orbital defect covered by a free radial forearm flap. It confirms flap survival and appearance. It corresponds to postoperative flap reconstruction and cosmetic management discussed in the section on “Orbital Exenteration and Reconstruction.”
Cosmetic management after orbital exenteration greatly affects a patient’s psychological and social adjustment.
Insertion of an orbital implant: After enucleation, inserting an orbital implant (such as hydroxyapatite or silicone) helps the prosthetic eye move better.
Fitting a prosthetic eye: After the orbital implant is placed, an ocularist makes and adjusts the prosthetic eye.
Facial prosthesis: After orbital exenteration, a facial prosthesis that covers the entire orbit may be used.
Flap reconstruction: When there is extensive tissue loss, orbital reconstruction is performed using a free flap or a pedicled flap.
Osseointegration (bone-anchored implant): A prosthesis attached to an implant fixed in the orbital bone is used as a cosmetically favorable method.
QWhat is daily life like after orbital exenteration?
A
After surgery, vision in one eye is lost, so adjustments in daily life are needed. In many cases, a cosmetic appearance can be restored by fitting an ocular implant and prosthetic eye, and a facial prosthesis is also one option. Ophthalmology, plastic surgery, ocularists, and psychologists work together to support rehabilitation. Regular postoperative ophthalmic follow-up also helps detect recurrence early.
Orbital undifferentiated carcinoma, etc. (maximum dose)
About 70 Gy
Irradiation given despite known complication risks
Radiation therapy is effective for malignant lymphoma, which is highly radiosensitive, when it is confined to the orbit.
When the irradiation dose exceeds 30 Gy, the risk of complications such as radiation-induced cataract, radiation-induced retinopathy, and radiation-induced optic neuropathy increases.
Heavy-ion therapy is used for tumors that are difficult to treat with conventional external beam radiation, such as adenoid cystic carcinoma.
Its use is expanding to orbital tumors (adenoid cystic carcinoma and lacrimal gland carcinoma), and a technique originally developed for intraocular malignant melanoma has been extended to orbital tumors.
In a retrospective study of carbon-ion therapy for lacrimal gland carcinoma with extraorbital extension, a 5-year local control rate of 62%, an overall survival rate of 65%, and an ipsilateral eye preservation rate of 86% were reported. It is a useful option for radioresistant tumors, but late complications such as optic nerve damage, cataract, and glaucoma occur with some frequency[7].
Neovascular glaucoma is relatively common with this treatment, so regular post-treatment monitoring of intraocular pressure and the fundus is needed.
Differential diagnosis with malignant lymphoma: Malignant lymphoma can also shrink to some extent with steroids, so it is a mistake to judge it as nonmalignant based on shrinkage alone.
Differential diagnosis with fungal infection: If an inflammatory-appearing lesion, especially at the orbital apex, is actually a focus of fungal infection, steroids can worsen and enlarge the lesion and put the patient’s life at risk. Giving steroids before the diagnosis is confirmed is contraindicated.
Systemic malignant lymphoma: Chemotherapy (such as CHOP and R-CHOP) is the first-line treatment.
Chemoreduction for malignant tumors of the paranasal sinuses: After shrinking the tumor with chemotherapy, surgical removal is performed. The goal is to improve resectability.
Hormone therapy: It may be effective for breast cancer and prostate cancer that have spread to the orbit.
Molecular targeted drugs (immune checkpoint inhibitors such as nivolumab): Their use is beginning to be indicated for liver metastases from ocular melanoma.
Regular imaging is essential for monitoring recurrence after surgery.
Recurrence assessment with MRI/CT: Imaging is performed every 3 to 6 months after surgery to check for local recurrence, lymph node metastasis, and distant metastasis.
Eye care after radiotherapy: After irradiation, the development of radiation cataract, radiation retinopathy, and optic neuropathy should be checked regularly. This is especially important in cases where the radiation dose exceeds 30 Gy, with regular tests of intraocular pressure, fundus, and visual fields.
Intraocular pressure management after carbon ion therapy: Because neovascular glaucoma is likely to occur, regular management with intraocular pressure measurement, angle examination, and fluorescein fundus angiography is necessary.
Maintenance of the prosthetic eye: The prosthetic eye should be cleaned, adjusted, and replaced regularly by an ocularist. In general, it needs to be remade every 5 to 7 years.
Management of the orbital implant: After blood vessel growth in the hydroxyapatite implant is complete (about 6 months after surgery), placing a prosthetic peg can improve movement of the prosthetic eye.
Psychological support: Loss of an eye and changes in facial appearance can place a heavy mental burden on the patient. Postoperative psychological support is an important part of care.
Lacrimal gland pleomorphic adenoma (complete resection cases): Prognosis is good. However, incomplete resection cases have a high recurrence rate, and repeated recurrences increase the risk of malignant transformation.
Adenoid cystic carcinoma: The prognosis is poor, with an average survival of 36 months and a 10-year survival rate of 20–30%. About 50% develop lung or bone metastases. A systematic review and meta-analysis found that multidisciplinary treatment with surgery + intra-arterial chemotherapy + postoperative chemoradiotherapy gave the best results, with a 5-year survival rate of 78%; surgery + radiation therapy gave 67%; and surgery alone gave 50%, showing that prognosis improves as treatment intensity increases [6].
Orbital malignant lymphoma (MALT type): Response to radiation therapy is good, and the prognosis is relatively favorable. Prognosis worsens in cases with systemic spread.
Orbital metastatic cancer: The prognosis is determined by the overall condition of the primary disease. The goal is to relieve local symptoms (reduce eye protrusion and preserve vision).
Orbital tumor removal using a transnasal endoscopic approach is being performed at some centers.
It is minimally invasive and has the advantage of leaving no facial scar, and its use is expanding for medial and inferior orbital lesions.
However, its indications are limited by the tumor’s location and size, and it should be performed at specialized centers.
Techniques are advancing in which titanium implants are osseointegrated into the orbital bone, and prostheses are attached with magnetic or bar fixation.
Compared with conventional adhesive methods, these offer greater attachment stability and better cosmetic results, and they have been reported to contribute to improved quality of life for patients.
Application of immune checkpoint inhibitors to ocular tumors
The use of immune checkpoint inhibitors such as nivolumab (an anti-PD-1 antibody) and pembrolizumab is being considered for expanded indications in cases of metastatic ocular malignant melanoma.
Clinical trials are underway internationally to evaluate the effectiveness and safety of these treatments for orbital metastatic cancer and ocular malignant melanoma.
Peirano D, Vargas S, Hidalgo L, et al. Management of periocular keratinocyte carcinomas with Mohs micrographic surgery and predictors of complex reconstruction: a retrospective study. An Bras Dermatol. 2024;99(2):202-209. doi:10.1016/j.abd.2023.05.004. PMID: 37989688.
Patel SY, Itani K. Review of Eyelid Reconstruction Techniques after Mohs Surgery. Semin Plast Surg. 2018;32(2):95-102. doi:10.1055/s-0038-1642058. PMID: 29765274.
Qedair J, Haider AS, Balasubramanian K, et al. Orbital Exenteration for Craniofacial Lesions: A Systematic Review and Meta-Analysis of Patient Characteristics and Survival Outcomes. Cancers (Basel). 2023;15(17):4285. doi:10.3390/cancers15174285. PMID: 37686561.
Martel A, Baillif S, Nahon-Esteve S, et al. Orbital exenteration: an updated review with perspectives. Surv Ophthalmol. 2021;66(5):856-876. doi:10.1016/j.survophthal.2021.01.008. PMID: 33524457.
Nagendran ST, Lee NG, Fay A, Lefebvre DR, Sutula FC, Freitag SK. Orbital exenteration: The 10-year Massachusetts Eye and Ear Infirmary experience. Orbit. 2016;35(4):199-206. doi:10.1080/01676830.2016.1176210. PMID: 27322708.
Yan HH, Liu R, Wang N, et al. Treatment of lacrimal gland adenoid cystic carcinoma: a systematic review and Meta-analysis. Int J Ophthalmol. 2024;17(1):164-172. doi:10.18240/ijo.2024.01.22. PMID: 38239951.
Hayashi K, Koto M, Ikawa H, Ogawa K, Kamada T. Efficacy and safety of carbon-ion radiotherapy for lacrimal gland carcinomas with extraorbital extension: a retrospective cohort study. Oncotarget. 2018;9(16):12932-12940. doi:10.18632/oncotarget.24390. PMID: 29560121.
Palamar M, Kaya E, Egrilmez S, Akalin T, Yagci A. Amniotic membrane transplantation in surgical management of ocular surface squamous neoplasias: long-term results. Eye (Lond). 2014;28(9):1131-1135. doi:10.1038/eye.2014.148. PMID: 24993317.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.