
Radiation Therapy for Eye Tumors (Radiation Therapy for Ocular Tumors)
1. What is radiotherapy used for eye tumors?
Section titled “1. What is radiotherapy used for eye tumors?”Radiation therapy (radiotherapy) is a treatment that uses high-energy electromagnetic waves or particle beams to irradiate a tumor, damage its DNA, and suppress or destroy the growth of tumor cells. In the field of eye tumors, it is widely used together with surgery and chemotherapy as a way to control the tumor locally while preserving the eyeball and visual function.
The significance of radiation therapy for eye tumors lies in the following three points.
- Eyeball preservation: Tumors can be controlled while avoiding surgical removal (orbital exenteration or enucleation).
- Local control: For highly radiosensitive tumors such as lymphoma, cure may be expected with radiation therapy alone.
- Adjuvant therapy: Used after chemotherapy or surgery to suppress residual tumor or recurrence.
Radiation therapy is selected according to the tumor type, size, location, and effects on surrounding normal tissue. The main irradiation methods are five types: external beam radiation therapy (EBRT), stereotactic radiotherapy, proton therapy, carbon ion therapy, and plaque brachytherapy.
Overview of the main radiation methods
Section titled “Overview of the main radiation methods”- External beam radiation therapy (EBRT): Conventional irradiation using X-rays or electron beams. Widely used for orbital lymphoma, PIOL, and metastatic eye tumors.
- Stereotactic radiotherapy: Concentrated irradiation of the tumor using Gamma Knife, CyberKnife, or a linear accelerator. Used for diseases that require precise irradiation, such as optic nerve sheath meningioma.
- Proton therapy: Uses the Bragg peak characteristics of proton beams to deliver a highly concentrated dose to the tumor and minimize effects on surrounding normal tissue. For uveal melanoma, local control rates above 90% and eye preservation rates of about 80% at 10 years have been reported [1,2]. It has been covered by insurance for orbital rhabdomyosarcoma since April 2016.
- Carbon ion therapy: Uses carbon ions, which have a higher biological effect than proton beams. It is promising for hard-to-treat tumors such as lacrimal gland adenoid cystic carcinoma and uveal melanoma, and the reported 5-year eye preservation rate for lacrimal carcinoma with orbital extension is 86% [5]. Neovascular glaucoma is a relatively common complication with this treatment.
- Plaque brachytherapy: A plaque (applicator) containing a radioactive isotope is sutured to the scleral surface corresponding to the tumor, and the tumor is irradiated directly. It allows local treatment and has a high eye preservation rate.
There are five types: external beam radiation therapy (EBRT), stereotactic radiotherapy (Gamma Knife, CyberKnife, and linear accelerator), proton therapy, carbon ion therapy, and plaque brachytherapy. The appropriate irradiation method is selected according to the type of disease, tumor size, and location.
2. Radiation dose and indications by disease
Section titled “2. Radiation dose and indications by disease”The recommended radiation dose and irradiation method differ depending on the type of eye tumor. The following outlines the radiation therapy used for major diseases.
The correspondence between disease-specific radiation doses and the irradiation methods used is as follows.
| Disease | Approximate radiation dose | Main radiation method |
|---|---|---|
| Orbital low-grade lymphoma | 30 Gy | External beam radiation therapy (EBRT) |
| Orbital intermediate- to high-grade lymphoma | 40 Gy | External beam radiation therapy (EBRT) |
| Orbital undifferentiated carcinoma (maximum dose) | 70 Gy | External beam radiation therapy (EBRT) |
| Intraocular lymphoma (PIOL) | 30 Gy | External beam radiotherapy (EBRT) |
| Metastatic uveal tumor | 40–50 Gy | External beam radiotherapy (EBRT) |
| Retinoblastoma | 40–46 Gy | External beam radiotherapy (fractionated X-rays) |
| Optic nerve sheath meningioma | Depends on the facility | Stereotactic radiotherapy |
| orbital rhabdomyosarcoma | 40–50 Gy | proton therapy (covered by insurance) |
| lacrimal gland adenoid cystic carcinoma | depends on the institution | carbon ion therapy |
Orbital lymphoma
Section titled “Orbital lymphoma”Because malignant lymphoma is highly radiosensitive, external beam radiation is used for malignant lymphoma confined to the orbit. About 30 Gy is given for low-grade lymphoma, and about 40 Gy for lymphoma of intermediate or higher grade. When the dose exceeds 30 Gy, the risk of complications such as radiation cataract, retinopathy, and optic neuropathy increases. For orbital undifferentiated carcinoma and similar tumors, about 70 Gy, which is considered the maximum dose, may sometimes be given with awareness of the risk of complications.
Primary intraocular lymphoma (PIOL)
Section titled “Primary intraocular lymphoma (PIOL)”For local eye lesions of primary intraocular lymphoma (PIOL), radiation therapy with a total dose of about 30 Gy is effective. Chemotherapy is combined for systemic disease.
Metastatic uveal tumor
Section titled “Metastatic uveal tumor”For metastatic tumors to the eye, irradiation of 40–50 Gy is used. It is often used for symptom relief (palliative irradiation).
Retinoblastoma
Section titled “Retinoblastoma”Fractionated X-ray irradiation at 40–46 Gy is used. However, with advances in chemotherapy and local treatments (plaque therapy, laser treatment, and cryotherapy), external beam irradiation is now limited to cases that cannot be controlled with other treatments. External beam irradiation in children is carefully considered because it carries a risk of secondary cancer and impaired orbital growth.
Optic nerve sheath meningioma
Section titled “Optic nerve sheath meningioma”It has been reported that stereotactic radiotherapy (LINAC, Gamma Knife, CyberKnife) can preserve visual function and suppress tumor growth. Because complete surgical removal may sacrifice the optic nerve, radiotherapy is the main treatment.
Orbital rhabdomyosarcoma
Section titled “Orbital rhabdomyosarcoma”The standard treatment is a combination of chemotherapy (VAC therapy) and radiotherapy. Proton therapy has been covered by insurance since April 2016, making it possible to deliver radiation while minimizing effects on surrounding normal tissues. For stage (IRS group) II to IV disease, chemotherapy and radiotherapy are combined, and 4,000–5,000 cGy (40–50 Gy) is delivered. With proton therapy, the dose to nearby structures such as the lens and orbital bones can be reduced much more than with photon therapy, and in pediatric cases excellent tumor control and fewer long-term complications have been reported [6].
Lacrimal gland adenoid cystic carcinoma
Section titled “Lacrimal gland adenoid cystic carcinoma”For unresectable adenoid cystic carcinoma, carbon ion radiotherapy is used. It is a promising treatment that can control the tumor while preserving the eyelid, eyeball, and orbit, and even in cases with extraorbital extension, a 5-year local control rate of 62% and an overall survival rate of 65% have been reported [5].
Low-grade lymphoma is treated with about 30 Gy, and intermediate- or high-grade lymphoma with about 40 Gy. In cases such as orbital undifferentiated carcinoma, very high-dose irradiation of about 70 Gy may be given. When the dose exceeds 30 Gy, the risk of radiation cataract, retinopathy, and optic neuropathy increases.
3. Plaque therapy (brachytherapy)
Section titled “3. Plaque therapy (brachytherapy)”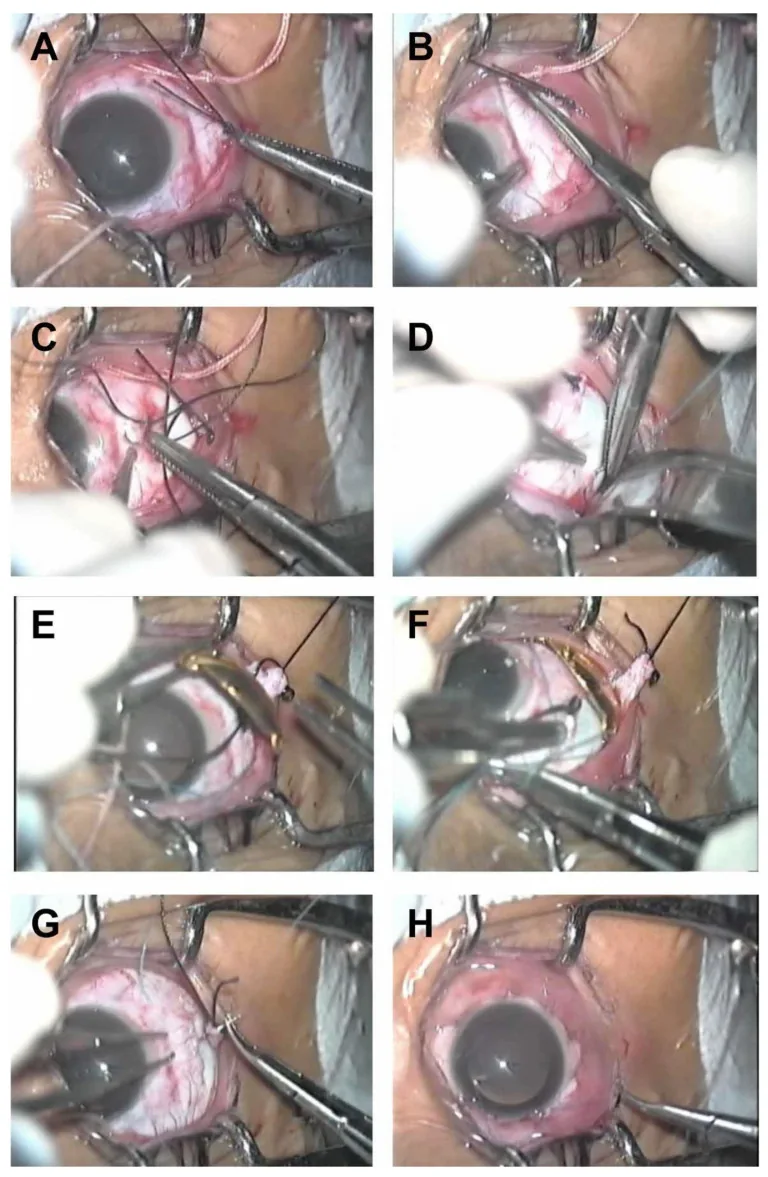
Plaque therapy is a local treatment in which a plaque (disk-shaped applicator) containing a radioactive isotope is temporarily sutured to the scleral surface corresponding to the tumor, delivering radiation directly into the tumor. It is positioned as a major eye-preserving treatment for uveal melanoma and retinoblastoma (recurrent or residual cases).
Radiation sources used
Section titled “Radiation sources used”The radiation source used varies by region.
- ¹⁰⁶Ru (ruthenium, β emitter): Mainly used in Japan and Europe. It emits beta rays (electron beams) and selectively irradiates the tumor.
- ¹²⁵I (iodine, γ emitter): Mainly used in North America. It emits low-energy gamma rays.
Indications
Section titled “Indications”The tumor criteria for ¹⁰⁶Ru plaque therapy are as follows.
- Tumor thickness: 5 mm or less
- Tumor diameter: 15 mm or less
- Tumor location: Localized tumor away from the optic disc
If the tumor is touching the optic disc or macula, or if the tumor is large, treatment may be difficult.
Local control rates and treatment characteristics
Section titled “Local control rates and treatment characteristics”Local control of 80% to 90% is possible. In the COMS (Collaborative Ocular Melanoma Study) trial, no significant difference in survival was reported between ¹²⁵I plaque brachytherapy and enucleation for medium-sized choroidal melanoma, and it has been established as an eye-sparing treatment [3]. Long-term outcomes of ¹⁰⁶Ru plaque therapy showed 5-, 7-, and 9-year survival rates of 99%, 97%, and 85%, respectively, with a local recurrence rate of about 1%, which is favorable [4]. Plaque therapy is pinpoint irradiation limited to the scleral surface corresponding to the tumor, and its advantage is less impact on surrounding normal tissue than external beam radiation.
It requires specialized surgical skill for plaque suturing and removal, and because a dedicated treatment room for radiation management is needed, the number of facilities that can perform it is limited.
Plaque therapy is a local irradiation method in which a radioactive plaque is directly sutured to the scleral surface corresponding to the tumor, so it concentrates the dose on the tumor and has little effect on surrounding normal tissue. External beam radiation irradiates the entire tumor area from outside the body, so it can treat broader tumors and multiple lesions, but it delivers more dose to surrounding structures such as the anterior orbit, lens, and optic nerve. The indication is selected according to tumor size, location, and type.
4. Side effects and management of radiation therapy
Section titled “4. Side effects and management of radiation therapy”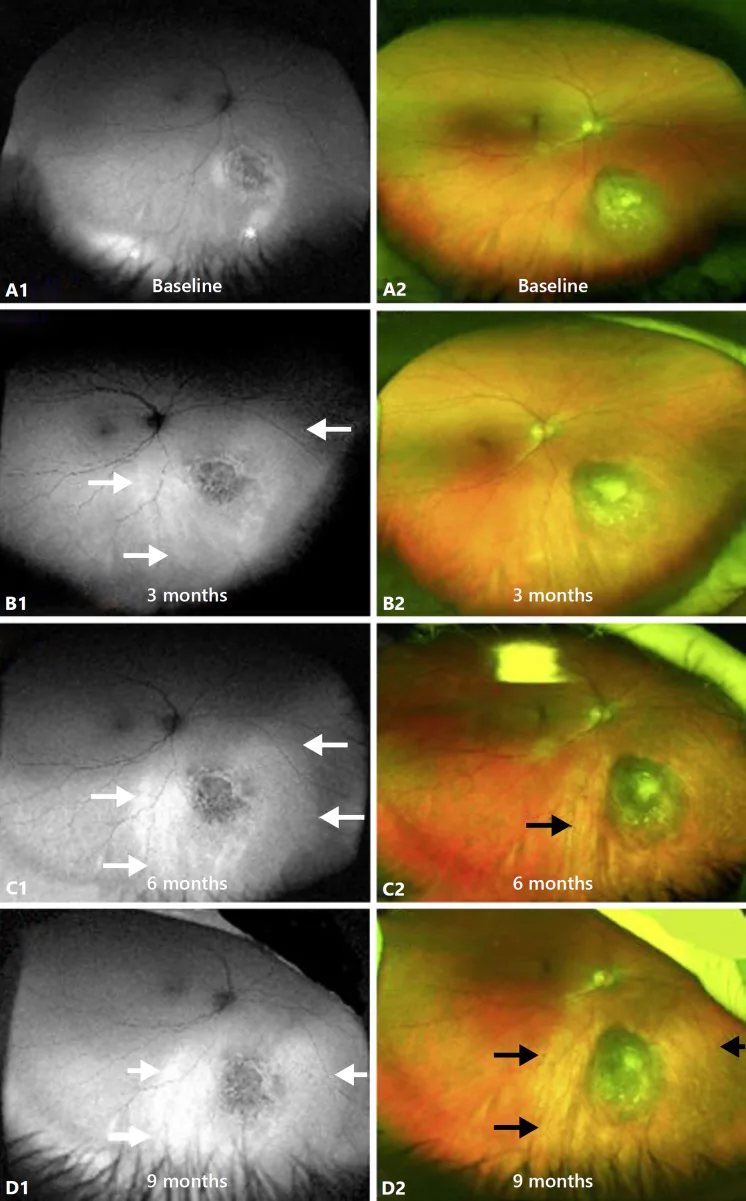
In radiation therapy for eye tumors, the treatment effect on the tumor comes at the cost of effects on surrounding normal tissues (side effects). Side effects vary depending on the radiation dose, treatment area, and type of therapy.
Main ophthalmic side effects
Section titled “Main ophthalmic side effects”- Radiation cataract: Risk increases when the irradiation dose exceeds 30 Gy. The lens is highly radiosensitive, and it often appears as posterior subcapsular cataract. Cataract surgery with phacoemulsification may be indicated.
- Radiation retinopathy: Capillary occlusion and retinal ischemia can cause exudative changes, neovascularization, and macular edema. It has been reported to occur in 20–53% after plaque brachytherapy [7]. Anti-VEGF therapy and laser photocoagulation are used for treatment, and prophylactic bevacizumab may reduce the development of macular edema [7].
- Radiation optic neuropathy: Irradiation of the optic nerve impairs optic nerve blood flow, causing decreased vision and visual field defects. It can lead to irreversible visual impairment.
- Dry eye: Caused by irradiation of the lacrimal gland and conjunctival goblet cells. It is managed with artificial tears and anti-inflammatory eye drops.
- Neovascular glaucoma: A relatively common complication after heavy ion therapy that requires intraocular pressure control.
- Orbital growth retardation: Especially in children, irradiation can impair the growth of the orbital bones and cause facial asymmetry. Proton therapy and heavy ion therapy can reduce the dose to surrounding normal tissues compared with conventional external beam X-ray therapy.
Secondary cancer risk (children)
Section titled “Secondary cancer risk (children)”External beam radiation in children, especially those with retinoblastoma, increases the risk of secondary cancers within the radiation field, such as osteosarcoma and soft tissue sarcoma. In hereditary retinoblastoma (biallelic RB1 mutations), the risk of secondary cancer is even higher, so the indication for external beam radiation must be considered carefully. Proton therapy is expected to reduce the risk of secondary cancer by lowering the dose to surrounding normal tissues.
Key points for follow-up
Section titled “Key points for follow-up”- After radiation therapy, continue regular ophthalmic examinations at least every 3–6 months.
- To detect radiation retinopathy, cataract, and optic neuropathy early, perform fundus examination, optical coherence tomography (OCT), and visual field testing regularly.
- In diseases with a risk of neovascular glaucoma (such as after heavy ion therapy), add intraocular pressure measurement and gonioscopy.
5. Treatment facilities and insurance coverage
Section titled “5. Treatment facilities and insurance coverage”The number of facilities where treatment can be performed and the status of insurance coverage differ depending on the type of radiation therapy.
Proton therapy
Section titled “Proton therapy”Since April 2016, proton therapy for orbital rhabdomyosarcoma has been covered by insurance. Proton therapy facilities are limited nationwide, so referral to a nearby facility may be needed.
Heavy-ion therapy
Section titled “Heavy-ion therapy”Heavy-ion therapy for hard-to-treat eye tumors, including lacrimal gland adenoid cystic carcinoma, is being performed at facilities in Japan. The range of approved conditions and the number of facilities are increasing.
Plaque therapy
Section titled “Plaque therapy”Because this requires a special treatment room and specialized technique, the number of facilities that can perform it is limited. Referral to an ophthalmology specialty facility that performs plaque therapy is necessary.
External beam and stereotactic radiotherapy
Section titled “External beam and stereotactic radiotherapy”External beam radiation using a linear accelerator can be performed at radiation therapy facilities nationwide. Stereotactic radiotherapy (Gamma Knife and CyberKnife) is performed at some facilities, and its use for eye tumors requires coordination between ophthalmology and radiation oncology.
6. Pathophysiology: How radiation works and the basis for dose setting
Section titled “6. Pathophysiology: How radiation works and the basis for dose setting”Effects of radiation on tumor cells
Section titled “Effects of radiation on tumor cells”Radiation (X-rays, gamma rays, and particle beams) causes double-strand breaks in cellular DNA and stops cell division. Because tumor cells have a lower ability to repair DNA than normal cells, they are more sensitive to radiation (a relative difference in sensitivity). The basic idea of radiation therapy is to use this principle to selectively kill tumor cells.
How the Dose Is Determined
Section titled “How the Dose Is Determined”The dose of irradiation (gray, Gy) is determined by balancing the tumor’s radiosensitivity with the tolerance dose of the surrounding normal tissues.
- Malignant lymphoma: It is highly radiosensitive, and cure can be expected with a relatively low dose of 30–40 Gy.
- Adenocarcinoma and sarcoma: Sensitivity is moderate to low, and a high dose of 40–70 Gy is needed.
- Optic nerve and retina: The tolerance dose to radiation is low (the lens has a cataract risk at around 2–4 Gy), so optimizing the irradiation field is essential.
Meaning of Fractionated Irradiation
Section titled “Meaning of Fractionated Irradiation”Usually, external beam radiation is divided into fractions of 1.8–2 Gy per session, five times a week over several weeks (fractionation). Fractionation gives normal cells time to repair DNA between sessions, while tumor cells receive the next dose with incomplete repair, optimizing the balance between treatment effect and side effects.
Physical Characteristics of Particle Beam Therapy
Section titled “Physical Characteristics of Particle Beam Therapy”Proton beam and heavy particle beam (carbon ion beam) therapy form a concentrated dose region called the “Bragg peak” at the end of the irradiation path. Whereas X-rays continuously release energy as they pass through tissue, particle beams release energy sharply at a specific depth and then drop to nearly zero. This makes it possible to deliver a high dose deep in the tumor while reducing dose to normal tissues behind the tumor at the same time. Carbon ion beams have an even higher relative biological effectiveness (RBE), and are expected to have greater killing effects than X-rays even against radioresistant tumors (such as adenoid cystic carcinoma).
7. References
Section titled “7. References”- Mishra KK, Daftari IK. Proton therapy for the management of uveal melanoma and other ocular tumors. Chin Clin Oncol. 2016;5(4):50. PMID: 27558251. doi:10.21037/cco.2016.07.06
- Chan AW, Lin H, Yacoub I, et al. Proton Therapy in Uveal Melanoma. Cancers (Basel). 2024;16(20):3497. PMCID: PMC11506608.
- Diener-West M, Earle JD, Fine SL, et al; Collaborative Ocular Melanoma Study Group. The COMS randomized trial of iodine 125 brachytherapy for choroidal melanoma, III: initial mortality findings. COMS Report No. 18. Arch Ophthalmol. 2001;119(7):969-982. PMID: 11448319.
- Cennamo G, Montorio D, D’Andrea L, et al. Long-Term Outcomes in Uveal Melanoma After Ruthenium-106 Brachytherapy. Front Oncol. 2022;11:754108. doi:10.3389/fonc.2021.754108
- Hayashi K, Koto M, Ikawa H, Ogawa K, Kamada T. Efficacy and safety of carbon-ion radiotherapy for lacrimal gland carcinomas with extraorbital extension: a retrospective cohort study. Oncotarget. 2018;9(16):12932-12940. PMID: 29560121.
- Yock T, Schneider R, Friedmann A, Adams J, Fullerton B, Tarbell N. Proton radiotherapy for orbital rhabdomyosarcoma: clinical outcome and a dosimetric comparison with photons. Int J Radiat Oncol Biol Phys. 2005;63(4):1161-1168. PMID: 15950401.
- Mularska W, Chicheł A, Rospond-Kubiak I. Radiation retinopathy following episcleral brachytherapy for intraocular tumors: Current treatment options. J Contemp Brachytherapy. 2023;15(5):372-382. PMID: 38026080. PMCID: PMC10669920.